Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
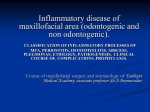
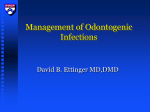
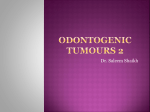
Dentomaxillofacial Radiology (1998) 27, 30 ± 35 1998 Stockton Press All rights reserved 0250 ± 832X/98 $12.00 Central calcifying odontogenic cyst. A review of the literature and the role of advanced imaging techniques JH Erasmus1, IOC Thompson2, LJ van Rensburg3,4 and AJ van der Westhuijzen1 1 Departments of Oral and Maxillofacial Surgery, 2Oral Pathology and 3Oral and Maxillofacial Radiology, Oral and Dental Teaching Hospital, University of Stellenbosch, Tygerberg; 4Bellville, Panorama, Republic of South Africa The central calcifying odontogenic cyst (CCOC) is a rare lesion. This paper reports a new case, reviews the clinical, histomorphological and radiographic features reported in the literature and describes the CT and MRI features of this new case. We postulate that, as part of an evolutionary process, cystic COCs originate as unilocular lesions but may later become multilocular. The role of advanced imaging and histology in the diagnostic process are discussed. Keywords: tomography, x-ray computed; magnetic resonance imaging; odontogenic cysts; diagnostic imaging Introduction Report of a case The central calcifying odontogenic cyst is a rare lesion. Its clinical and radiological features are not pathognomonic,1,2 and it is characterized by histological diversity. Radiographically, it presents as a unilocular or, occasionally, multilocular radiolucency that may contain calci®ed radiopacities or tooth-like densities. Unilocular lesions are therefore compatible with dentigerous, radicular or residual cysts, while multilocular lesions may resemble ameloblastomas or odontogenic keratocysts. The correlative diagnostic imaging and histological ®ndings of some odontogenic tumours and cysts have been reported in the recent literature3 ± 6 In these cases, while CT displayed aspects of bone morphology not visible on plain ®lms, MRI provided essential macropathlogical detail which correlated well with the histological ®ndings. The features identi®ed by these combined imaging techniques are helpful in differentiating cysts from other neoplastic lesions and can thus alter surgical management. The purpose of this report is to present a calcifying odontogenic cyst that occured in the anterior region of the mandible, to review the relevant literature and to describe its CT and MRI features, which has to our knowledge, have not been reported before. A 29-year-old female was referred to the Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, University of Stellenbosch with a painful swelling in the anterior mandible that had been present for approximately 1 year. No unusual features were noted on extra-oral examination. Intraorally, there was a well-de®ned ®rm swelling, of 3.562 cm, with a smooth surface on the lingual aspect of the anterior mandible. The lesion extended from the right lateral incisor to the left canine and ¯uctuation of the thinned, expanded lingual cortex could be demonstrated. The mucosa overlying the lesion was intact. The right central incisor, both left incisors and the left canine did not react to cold or electrical stimulation and the left central and lateral incisors were mobile. There was no buccal expansion or paraesthesia of the lower lip. Her medical history was noncontributory. Radiographic examination disclosed a well-de®ned unilocular radiolucency of the anterior mandible, extending transsymphyseally from the right lateral incisor to the left canine. Root resorption of both the left central and lateral incisors was evident. (Figures 1 and 2). A single calci®ed focus was noted on the occlusal view (Figure 2). The dierential clinical diagnosis included cystic ameloblastoma and odontogenic keratocyst. CT and MRI were performed to characterize the lesion further. Five mm thick axial CT scans with both soft tissue and bone algorithms showed a wellcorticated, partially septated, predominantly lingually expansile cystic lesion in the anterior mandible, Correspondence to: Dr JH Erasmus, Faculty of Dentistry, University of Stellenbosch, Private Bag X1, Tygerberg 7505, South Africa Received 2 May 1997, accepted 23 September 1997 Calcifyng odontogenic cyst J Erasmus et al 31 measuring 362 cm. Although the lingual cortex was very thin there was no loss of continuity. The cyst contents measured 26 Houns®eld units consistent with a ¯uid more dense than water (Figure 3). MRI at 0.5 tesla included T2-weighted FSE images (long TR/TE, 4725/120 ms) and T1-weighted (short TR/TE, 520/25 ms) SE images before and after intravenous gadolinium-DTPA (`Magnevist'1 0.1 mmol/kg) Schering, Berlin, Germany). On T2-FSE images the cyst contents displayed an homogenous high signal intensity, similar to cerebrospinal ¯uid (CSF). The incomplete septum was clearly identi®ed on the T2 FSE images and displayed uptake of the contrast by the overlying epithelium on T1weighted images (Figures 4 and 6). The major component of the cyst extended into the left sublingual space but there was no extraosseous spread. (Figure 4). On short TE/TR images (T1-weighted) the cyst contents displayed a degree of T1 shortening and appeared isointense with muscle, indicative of a high protein content (Figure 5). Short TE/TR (T1-weighted) images showed uptake of contrast in the lining epithelium which was of varying thickness (Figure 6). However, no calci®cations were identi®ed on either CT or MRI. A plexiform follicular ameloblastoma was considered the most likely diagnosis. L Figure 1 Cropped panoramic radiograph showing a well de®ned unilocular radiolucency of the anterior mandible. Root resorption of the left central and lateral incisors is evident Figure 3 Axial 5 mm CT Scan shows bony septum anteriorly (arrow A) and the well corticated lingual expansion (arrow B) Figure 2 Oblique occlusal radiograph showing the thin lingual expansion, root resorption of the left central and lateral incisors and a small nonspeci®c linear shaped calci®ed focus in relation to the left lateral incisor. This opacity could be identi®ed retrospectively on the panoramic radiograph Figure 4 Axial 5 mm T2-Fast Spin Echo MR scan showing the lesion ®lled with homogenous, high signal intensity ¯uid extending into the left sublingual space, and the incomplete septum, anteriorly Calcifyng odontogenic cyst J Erasmus et al 32 Figure 7 Photomicrograph of the cyst wall showing the odontogenic epithelial lining with sheets of ghost cells (original magni®cation 6200) Figure 5 Axial 5 mm T1-SE MR image showing the cyst contents isointense with muscle Figure 8 Photomicrograph showing sheets of ghost cells with areas of calci®cation (original magni®cation 6200) Figure 6 Axial 5 mm T1-SE MR image scan following the administration of contrast showing the varying thickness of the enhanced epithelium The cyst was enucleated under general anaesthesia and con®rmed the imaging ®ndings. The non-vital teeth were endodontically treated. The postoperative course was uneventful. Histological examination con®rmed the diagnosis of calcifying odontogenic cyst. Discussion An incisional biopsy was performed under local anaesthesia. Histological examination showed a cystic lesion with a ®brous capsule lined by odontogenic epithelium of varying thickness. The basal cells of the epithelium were predominantly columnar with features similar to those of ameloblasts, while the overlying cells were more loosely arranged resembling stellate reticulum. (Figure 7). Sheets of eosinophilic ghost cells with areas of calci®cation were a prominent feature. (Figure 8). Dysplastic dentine (dentinoid) was observed in the connective tissue adjacent to the epithelium and the capsule contained a chronic in¯ammatory cell in®ltrate. The lesion was diagnosed as a calcifying odontogenic cyst. Epithelial-lined cysts seldom occur in skeletal bones, because embryonic epithelial rests are normally not found in them. They do, however, occur in the jaws where the majority are lined by epithelium derived from remnants of the odontogenic apparatus. These odontogenic cysts are classi®ed as either of developmental or in¯ammatory origin.7 The calcifying odontogenic cyst (COC) is a rare example of a developmental odontogenic cyst. Gorlin and colleagues (1962)8 were the ®rst to describe this entity. They initially regarded it as the oral analogue of the cutaneous calcifying epithelioma of Malherbe but later labelled it the calcifying Calcifyng odontogenic cyst J Erasmus et al 33 odontogenic cyst. Prior to this, Rywkind (1932) described it as a variant of the cholesteatoma, while Maitland (1947)10 regarded it as a type of ameloblastoma. The COC has also been reported under a variety of other designations including: dentinogenic ghost cell odontogenic tumour,11 epithelial odontogenic ghost cell tumour,12 ghost cell cyst,13 calcifying ghost cell odontogenic tumour,14 and dentino-ameloblastoma.15 The WHO presently describe the calcifying odontogenic cyst as a non-neoplastic cyst, but classify it as a benign tumour.16 Langlais and colleagues (1995)17 proposed the term calcifying odontogenic lesion (COL), which encompasses both the cystic and tumorous forms as well as combined lesions containing elements of both. The odontogenic origin of the COC is widely accepted.18 Praetorius et al11 suggested that it develops in the dental follicle, gingival tissue or bone from remnants of either odontogenic epithelium or reduced enamel epithelium. The pathogenesis is, however, still controversial.15 While it is accepted that the epithelial lining may induce the production of dentinoid or an odontoma, the question whether COCs that have features of other odontogenic tumours develop them secondarily or whether the COCs are themselves a secondary phenomenon in pre-existing odontogenic tumours, is still unresolved.19 The former concept is widely accepted,13 but several investigators still support the latter possibility.20 ± 22 The majority of COCs arise centrally in bone, but several peripheral (extraosseous) examples have been reported,20,23,24 Both central and peripheral forms occur with equal frequency in the maxilla and mandible.7,24,25 The majority of lesions are located in the incisor-canine area.25 The COC comprises between 0.37 ± 2.1% of all odontogenic tumours.8,15,24,26 The peripheral variant comprises 13 ± 25% of the COCs.7,20,23 Praetorius et al11 reported a bimodal age distribution, with peaks in the second and sixth decades. The odontomaassociated type occurred at an earlier age (17 years), while the neoplastic variant was more common in older patients.7 Buchner found an almost equal gender distribution.25 The highest prevalence occurred in the second and third decades, with a mean age of 30.3 years. The central COC presents as an asymptomatic hard swelling of the jaws that produces expansion rather than erosion of bone.24,25 Pain indicates secondary infection.23 Early lesions are usually detected following routine radiographic examination and they are often associated with an unerupted tooth.1,27 The peripheral COC presents on the gingiva as a non-speci®c wellcircumscribed sessile or pedunculated mass with a smooth surface. They resemble other epulides such as gingival ®bromas or peripheral giant cell granulomas.24 The de®nitive diagnosis of COC is made histologically, due to the lesion's lack of characteristic clinical and radiological features, as well as its variable biological behaviour. Cystic and solid variants of COCs are described with the cystic variant comprising the majority of cases.15,18,25,28,29 The histological features of the COC are complicated by its frequent association 9 with other odontogenic tumours, such as the complex or compound odontoma, ameloblastoma, odontoameloblastoma, ameloblastic ®broma, ameloblastic ®bro-odontoma and the adenomatoid odontogenic tumour.15,18,21,25,26,29 Five malignant tumours have been reported.11,20,30,31 The associated tumour rather than the cyst determines the biological behaviour of these lesions21,23 This histological diversity together with it's variable clinical behaviour illustrate the unusual nature of this lesion and has resulted in dierent classifications.11,25 Many authors accept the classi®cation developed by Praetorius et al11 in an analysis of 16 cases (Table 1). Buchner25 recognized the multicystic COC as a separate entity in an excellent review of 215 cases of central COCs and proposed a more detailed classi®cation that encompass all reported clinical and pathological variations of this lesion (Table 2). Enucleation is the preferred mode of treatment for simple cystic lesions, but, when an odontogenic tumour co-exists, the tumorous part of the lesion determines the type of treatment.11 Recurrence is unusual. Only nine cases have been reported and all recurred within 8 years.25 A follow-up period of at least 10 years is, therefore, recommended. According to Buchner's classi®cation25 this lesion would be classi®ed as a central multicystic COC (type B 1a). The classi®cation of Praetorius does not recognise multicystic lesions as a separate entity. The presence of radiopacities could suggest a diagnosis of an adenomatoid odontogenic tumour, a calcifying epithelial odontogenic tumour or an ameloblastic ®bro-odontoma.1 Nagao and colleagues21 reported in a series of 23 cases only three cases of multilocular lesions, which converts to a ratio of 7.6 : 1. In 33% of cases COCs are associated with unerupted Table 1 Classification of calcifying odontogenic cysts proposed by Praetorius et al11 Type Description 1a 1b 1c 2 Simple unicystic type with little or no dentinoid Odontoma producing type Ameloblasomatous proliferating type Neoplastic variant (dentinogenic `ghost' cell tumor) Table 2 Classification of calcifying odontogenic cysts proposed by Buchner25 Type Description A Peripheral (extraosseous) COC Cystic variant Neoplastic (solid) variant Central (intraosseous) COC Cystic variant Simple (unicystic or multicystic) Associated with an odontoma Associated with odontogenic tumours (other than odontoma) Other variants (such as clear cell variant, pigmented variant) Neoplastic (solid) variant Malignant COC B 1 (a) (b) (c) (d) 2 3 Calcifyng odontogenic cyst J Erasmus et al 34 teeth.7 Root resorption or root divergence may also be observed. The peripheral COC rarely exhibits radiographic bony involvement, but it may causes super®cial erosion of the underlying bone.24,28 CT complements conventional radiographs by depicting the anatomy and topography more accurately. Lesions can be characterized as cystic or solid by virtue of Houns®eld attenuation values. The intraand extraosseous extent of lesions are more accurately determined. Axial sections are invaluable in the assessment of lesions that are situated in the symphysis of the mandible. Conventional and panoramic ®lms provide insucient detail in this area.32 In our case the use of CT virtually excluded the OKC as a dierential diagnosis because it lacked the generally accepted features, namely a thick, sclerotic margin, a cloudy lumen and minimal cortical expansion.17 MRI produces multiplanar, superior imaging of the soft tissues without exposing the patient to radiation. It accurately dierentiates between cysts and solid tumours. Cyst contents can be characterized as ¯uid, keratin or blood degradation products.32 With MRI the margins of cystic lesions can be accurately evaluated for possible soft tissue extension; T2-weighted images re¯ect tumour-tissue margins most accurately.33 Fibrous or incomplete ossi®ed septa and mural nodules can be demonstrated. The latter may be the only diagnostic clue that a mural ameloblastoma is arising in a pre-existing dentigerous cyst. MRI is regarded as superior to CT in the evaluation of mandibular lesions, because it can depict both cortical and medullary involvement.33 The histological nature of the lesion and age of the patient are important factors in recurrence of the COC. Wright and co-workers34 noted that four recurrent cases occured in patients over the age of 60. The histology of three recurrent cases was documented: one solid neoplastic tumour,7 one mixed cystic and solid COC associated with an odontoma34 and one cystic lesion.35 In this case the incomplete bony septum detected with CT and MRI was an unexpected ®nding. A similar phenomenon has been observed in ameloblastomas: MRI demonstrated that apparent incomplete bony septa were in fact completed by soft tissue.6 Based on this observation, we postulate that cystic COCs originate as unilocular lesions but may become multilocular as part of an evolutionary process. The septa are initially ®brous, but may become ossi®ed later. Partially ossi®ed septa may, therefore, be interpreted as an indication of a longstanding lesion. It also implies that apparent unicystic COCs discovered at an advanced age, may often be actual multilocular lesions. It is possible that the recurrent cystic COCs were multilocular, because our case demonstrated that septa may not be evident without the help of advanced imaging techniques. We speculate that multilocularity underlies the role of age in recurrent cystic COCs. Langlais et al17 stated that in some lesions of the exact same histological tissue type, a multilocular pattern may someday prove to be more predictive of recurrence than a unilocular presentation. Except for the bony septum, no other calci®cations were identi®ed on either modality. On ®rst principles, it is expected that MRI using conventional sequences would be insensitive to small areas of calci®cations. Gradientecho recalled sequences should be able to detect subtle calci®cations by virtue of increased susceptibility to artifact.36 High resolution CT scans might also detect more subtle calci®cations. The signi®cance of radiopaque ¯ecks or calci®cations on conventional radiographs has been addressed in the literature.17 The fact that it may actually be septa in the process of ossi®cation, adds more signi®cance to this plain ®lm observation. In conclusion, although the role of CT and MRI in the pre-operative evaluation of this case is well demonstrated, no characteristic features were revealed. Because the COC lacks pathognomonic clinical, radiological, CT and MRI features, it should be included in the dierential diagnosis of cystic lesions that present anterior to the ®rst molar teeth. The plain ®lm observation of a calci®ed focus in a radiolucent lesion can be an important clue to the possibility of a multilocular lesion. The de®nitive diagnosis of this lesion remains dependent on histological evaluation. Acknowledgements Dr L Janse van Rensburg in the practice of Drs Schnetler, Corbett and partners provided imaging facilities to the Dental Teaching Hospital, University of Stellenbosch; Ms P de Klerk, T Jonker, G Claasen, M Davids and J Hans performed the examinations; Schering (SA) provided the contrast material. References 1. Tse KM, To EWH. Central calcifying odontogenic cyst. Case report. Aust Dent J 1995; 40: 357 ± 359. 2. Lello GE, Makek M. Calcifying odontogenic cyst. Int J Oral Maxillofac Surg 1986; 15: 637 ± 644. 3. Janse van Rensburg L, Nortje CJ, Thompson IOC. Correlating imaging and histopathology of an odontogenic keratocyst in the nevoid basal cell carcinoma syndrome. Dentomaxillofac Radiol 1997; 27: 195 ± 199. 4. Thompson IOC, Van Rensburg LJ, Phillips VM. Desmoplastic ameloblastoma: correlative histopathology, radiology and CTMR imaging. Oral Pathol Med 1996; 25: 405 ± 410. 5. Minami M, Kaneda T, Ozawa K, Yamamoto H, Itai Y, Ozawa M, et al. Cystic lesions of the maxillomandibular region: MR imaging of odontogenic keratocysts and ameloblastomas from other cysts. AJR 1996; 166: 943 ± 949. 6. Minami M, Kaneda T, Yamamoto H, Ozawa K, Itai Y, Ozawa M, et al. Ameloblastoma in the Maxillomandibular region: MR imaging. Radiology 1992; 184: 389 ± 393. 7. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology 1st ed. WB Saunders: Philadelphia, 1995, pp 506 ± 509. Calcifyng odontogenic cyst J Erasmus et al 35 8. Gorlin RJ, Pindborg JJ, Clausen FP, Vickers RA. The calcifying odontogenic cyst: A possible analogue of the cutaneous calcifying epithelioma of Malherbe. Oral Surg 1962; 15: 1235 ± 1243. 9. Rywkind AW. Beitrag zur pathologie der cholesteatome. Virchow's Arch Path Anat 1932; 283: 13 ± 28. 10. Maitland GR. Atypical adamantinoma of maxilla: Report of a case. J Oral Surg 1947; 5: 351 ± 355. 11. Praetorius F, Hjorting-Hansen E, Gorlin RJ, Vickers RA. Calcifying odontogenic cyst: Range, variations and neoplastic potential. Acta Odontol Scand 1981; 39: 227 ± 240. 12. Ellis GL, Shmookler BM. Aggressive (malignant?) epithelial odontogenic ghost cell tumor. Oral Surg Oral Med Oral Pathol 1986; 61: 471 ± 478. 13. Farman AG, Smith SN, Nortje CJ, Grotepass FW. Calcifying odontogenic cyst with ameloblastic ®bro-odontome: One lesion or two? J Oral Pathol 1978; 7: 19 ± 27. 14. Fejerskov O, Krogh J. The calcifying ghost cell odontogenic tumor - Or the calcifying odontogenic cyst. J Oral Pathol 1972; 1: 273 ± 287. 15. Shear M. Developmental odontogenic cysts. An update. J Oral Pathol Med 1994; 23: 1 ± 11. 16. Kramer IRH, Pindborg JJ, Shear M. Histological typing of odontogenic tumors. Berlin: Springer Verlag, 1992. 17. Langlais RP, Langland OE, Nortj CJ. Diagnostic imaging of the jaws 1st ed. Williams & Wilkens: Malvern, 1995, pp 305 ± 308. 18. Hong SP, Ellis GL, Hartman KS. Calcifying odontogenic cyst. Oral Surg Oral Med Oral Pathol 1991; 72: 56 ± 64. 19. Shear M. Cysts of the Oral Regions. Bristol, Wright PSG, 1983, pp 59 ± 66. 20. Altini M, Farman AG. The calcifying odontogenic cyst. Oral Surg Oral Med Oral Pathol 1975; 40: 751 ± 759. 21. Nagao T, Nakajima T, Fukushima M, Ishiki T. Calcifying odontogenic cyst: a survey of 23 cases in Japanese literature. J Maxillofac Surg 1983; 11: 174 ± 179. 22. Toida M, Ishimaru JI, Tatematsu N. Calcifying Odontogenic cyst associated with compound odontoma: Report of a case. J Oral Maxillofac Surg 1990; 48: 77 ± 81. 23. Freedman PD, Lumerman H, Gee JK. Calcifying odontogenic cyst: A review and analysis of seventy cases. Oral Surg Oral Med Oral Pathol 1975; 40: 93 ± 106. 24. Swan RH, Houston GD, Moore SP. Peripheral calcifying odontogenic cyst (Gorlin cyst). J Periodontl 1985; 56: 340 ± 343. 25. Bucher A. The central (intraosseous) calcifying odontogenic cyst: An analysis of 215 cases. J Oral Maxillofac Surg 1991; 49: 330 ± 339. 26. Shamaskin RG, Svirsky, JA, Kaugars GE. Intraosseous and extraosseous calcifying odontogenic cyst (Gorlin cyst). J Oral Maxillofac Surg 1989; 47: 562 ± 565. 27. McGowan RH, Browne RM. The calcifying odontogenic cyst: a problem of preoperative diagnosis. Br J Oral Surg 1982; 20: 203 ± 212. 28. Bucher A, Merrell PW, Hansen LS, Leider AS. Peripheral (extraosseous) calcifying odontogenic cyst: A review of 45 cases. Oral Surg Oral Med Oral Pathol 1991; 72: 65 ± 70. 29. Tajima Y, Ohno J, Utsumi N. The dentinogenic ghost cell tumor. J Oral Pathol 1986; 15: 359 ± 362. 30. Ikemura K, Horie A, Tashiro H, Nandate M. Simultaneous occurrence of a calcifying odontogenic cyst and its malignant transformation. Cancer 1985; 56: 2861 ± 2864. 31. Grodjesk JE, Dolinsky HB, Schneider LC, Dolinsky EH, Doyle JL. Odontogenic ghost cell carcinoma. Oral Surg Oral Med Oral Pathol 1987; 63: 576 ± 581. 32. Weber AL. Imaging of cysts and benign odontogenic tumors of the jaw. Oral Maxillofac Surg Clin North Am 1992; 4: 61 ± 74. 33. Van Rensburg LJ, Nortje C. Magnetic resonance imaging and computed tomography of malignant diseases of the jaw. Oral Maxillofac Surg Clin North Am 1992; 4: 75 ± 111. 34. Wright BA, Bhardwaj AK, Murphy D. Recurrent calcifying odontogenic cyst. Oral Surg Oral Med Oral Pathol 1984; 58: 579 ± 583. 35. Slootweg PJ, Koole R. Recurrent calcifying odontogenic cyst. J Maxillofac Surg 1980; 8: 143 ± 145. 36. Makow LS. Magnetic Resonance Imaging: A brief review of image contrast. Radiol Clin North Am 1989; 27: 195 ± 218.