Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
LUPUS NEPHRITIS & Its Management
By
Dr. Ahmed Rabie El-Arbagy
Professor Of Renal Medicine
Head of Internal Medicine Dep.
Faculty Of Medicine- Menoufia University
AGENDA
Definition
Epidemiology, Aetiology & Pathogenesis
LN Manifestations
SLE Diagnosis & DD
Renal biopsy & Pathology in LN
Treatment of LN
Special situations
CONCLUSION
LN, Definition
LN is a common& serious features of SLE.
A combination of clinical & laboratory features.
Need at least 4 criteria for diagnosis of lupus according to
the American College of Rheumatology( ACR).
If at least 4 of the 11 criteria develop at one time or
individually over any period of observation, then the
patient can be classified as an SLE patient for research
purposes.
However, a diagnosis of SLE can be made in a patient
having fewer than four of these symptoms( 1 clinical & 1
immunological / SLICC).
LN, Epidemiology
Age : Peak incidence of lupus is 15-45ys
Sex : Female > male( 10:1)
LN affect both genders equally( more severe in
children, less in older adults)
Race: more common in African American,
Afro-Caribians, Asians&
Hispanic Americans than
in Caucasians.
LN , Additional risk factors for renal disease
Younger age,
Lower socioeconomic status,
More ACR criteria for SLE,
Longer duration of disease,
F/H of SLE & HTN
LN, Etiology & Pathogenesis
Genetics, Enviromental, Hormonal & Animal Models, certain
medications &? Viral
Genetics
* Clustering in families,
* Racial differences in susceptibility,
* Multiple genes predispose to lupus,
17 loci associated with increased risk of SLE
Environmental
* Sun or U/V light exposure & sunburn can precipitate &
exacerbate SLE & LN.
LN, Etiology & Pathogenesis
Hormonal Factors
* Strong female predisposition,
*Exacerbation during or shortly after pregnancy.
* Role of hormonal treatment & ablation in
animal models of LN.
Exposure to certain medications
Can produce SLE or lupus-like syndrome,
renal disease is frequent in these patients
Viral pathogenesis of SLE & LN?
Spontaneous & inducible models of SLE in mice
Some models have defective apoptosis lead to defective clonal
deletion & B- cell proliferation.
LN, Autoimmunity in S LE
- SLE patients typically develop a wide range of autoantibodies
- Disease process starts with a breakdown in self tolerance &
autoantibody production.
- The pathogenesis may be dysregulated cellular apoptosis
resulting in autoantibodies against nucleosomes;
antibody/nucleosome complexes then bind to components of
the glomerulus to form immune complex(IC) glomerular
disease.
- Subsequently, deposition of ICs & the inflammatory
responses in various organs dictate the nature & extent of
disease.
A number of mechanisms may contribute to
autoimmunity in SLE
* Failure to remove or to sielence autoreactive B & T
cells
* Abnormal exposure to or presentation of self Ags
* T cell hyperactivity
* Increase B cell- stimulating cytokines & B hyperactivity
* Failure of apoptotic mechanisms to delete or to
sielence autoreactive cells(tolerance)may allow clonal
expansion of such cells later in life, leading to autoreactive
cells & autoantibody production.
* End result is the loss of tolerance & production of a
wide array of autoantibodies.
LN, Pathogenesis
*Autoantibodies combine with antigen to produce
Ics that if not adequately cleared may deposit in
various organs, inciting inflammatory responses.
*Autoantibodies against dsDNA
*Localization of ICs in glomerulus leads to
complement activation & complement- mediated
damage
*Intraglomerular HTN & activation of coagulation
cascades contributes to glomerular injury.
*Vascular damage in LN( simple localization of ICs to
a necrotizing vasculitis & tubulointerstitial disease.
LN, Clinical Manifestation
-SLE can affect any organ in body
- Disease course is characterized by
episodes of Illness (flares) followed by
episodes of relative Quiescence
( remissions).Earthquake style.
- Scoring systems to follow activity of
an individual patient with SLE
-SLE disease Activity Index ( SLEDAI)
LN, Renal Manifestations
At Presentation: 30- 50% of SLE patients will have
clinically evident renal disease.
*During follow up: renal involvement will occur in 60%
of young adults and a greater % of young children.
Renal involvement is manifested by:
- Proteinuria - Active urinary sediment with microhematuria(>
macro)
- Dysmorphic erythrocytes & erythrocytes casts & - HTN
- In many cases with major renal involvement, the
nephritic
syndrome develops in association with proliferative
GN
- Decline in GFR
- Specific histologic glomerular findings
Infrequently, renal involvement presents with tubular disorders
e. g. RT acidosis with hypokalemia( type 1 RTA) or hyperkalemia
(type 4 RTA)
- Thrombotic disorders associated with a secondary
antiphospholipid syndrome .
LN, Extrarenal manifestations
*Non specific complaints: malaise, low grade fever,
poor appetite & weight loss.
*Other common features include: patchy alopechia, oral or
oronasal ulcerations, arthralgias and nondeforming arthritis and
*A variety of dermal findings including:
Photosensitivity, Raynoud,s phenomenon, and the classic (
butterfly) fascial rash
*Livedoreticularis is seen in up to 15% of cases and may be
associated with: Miscarriage,
- Thrombocytopenia and
- Presence of antiphospholipid antiboies(APA).
*Neuropsychiatric involvement presents with:
Headache, nerve palsies, frank coma and psychosis.
LN, Extrarenal manifestations
* Serositis: pleuritis or pericarditis( affects ~ 40 % of cases)
* Pulmonary HTN (due to multiple pulmonary emboli or
intravascular coagulation in association with APA or be caused by
nonthrombotic pulmonary arterial disease
*Endocarditis, mitral valve prolapse
Splenomegaly & lymphadenopathy in
~ fourth of patients
*Hematologic abnormalities in SLE include:
- Anemia( impaired erythropoiesis,
autoimmunehemolysis & bleeding).
- Thrombocytopenia &leucopenia
( either part of disease or complications of treatment).
- Thrombotic events should prompt a search
for APA and other procoagulant abnormalities.
Diagnosis & DD of SLE & LN
The onset of lupus may be acute, resembling an infectious
process, or it may be a progression of vague symptoms
over several years. As a result, diagnosing SLE is often a
challenge.
-It may be obvious & easy in a young female patient in
presence of classic manifestations & serologic markers.
- Less typical presentations can result in multiple physician
consultations and diagnosis delay. This is due to varied
features of the disease S&S in SLE evolve over time.
-In some cases of LN patient with membranous LN may
present with renal disease as initial presentation without
other systemic features.
American College Of Rheumatology(ACR) Criteria For SLE
diagnosis
The presence of 4 ACR criteria carries a 96% sensitivity &
specificity for SLE.
1- Malar rash 2- Discoid rash 3- Photosensitivity
4- Oral ulcers 5- Nonerosive arthritis 6- Pleruopericarditis
7- Renal disease( proteinuria & or cellular casts)
8- Neurologic disorders( seizures or psychosis in the
absence of precipitating circumstances)
9- Hematologic disorder( hemolytic anemia,
leucopenia,lymphopenia, thrombocytopenia)
10- Positive LE cell preparation, raised anti-DNA
antibody, anti-Sm present, false- positive
antitreponemal test).
11- Positive fluorescent antinuclear antibody test
DD Of SLE
*Other diseases mimicking SLE:
- Fibromyalgia - Sjogren,s syndrome
- Hematologic diseases ( thrombotic microangiopathies) and
primary antiphospholipid syndrome
- Other autoimmune rheumatologic disorders ( dermatomyositis
& systemic sclerosis) can be confused with SLE.
DD Of SLE
*Other diseases associated with renal involvement:
-Mixed connective tissue disease with nephritis
(absence of anti- dsDNA antibodies).
-Rheumatoid arthritis( RA) and mesangial proliferative GN or renal
disease due to AA amyloidosis. Also, some older lupus patients can
present with joint deformities typical of RA.
-Differentiate LN from other common features of GN: HenochSchonlein purpura may present with a purpuric rash, systemic
symptoms, arthritis, abdominal pain &nephritis with prominent IgA
deposits in glomeruli.
In LN, most active proliferative biopsy specimen will show a
predominance of IgG & C1q.
-Bacterial endocarditis & cryoglobulinemia can also mimick lupus
especially in presence of low complement.
Immunologic Tests In Lupus
Autoantibody production is a hallmark
A firm diagnosis of LN should be made without the
presence of some serum ANA
ANA present in > 90% of untreated patients, non-specific
and found in other rheumatologic & non-rheumatologic diseases.
Some lupus- like patients with negative ANA test results will be
found to have APA.
Autoantibodies against dsDNA are far more specific, being
present in ~ 3/4th.of untreated lupus patients.
High titres of anti dsDNA antibodies correlate with SLE and use to
follow course of LN.
Antibodies to C1q (anti-C1q) have been more closely associated
with the activity of LN than anti dsDNA antibodies and may have a
prognostic role in the follow up of patients with LN.
Immunologic Tests In Lupus
Serum levels of total hemolytic complement & complement
components C3 & C4.
Either C3 & C4 are both depressed or C4 is preferentially
depressed in lupus patients, reflecting preferential activation of
the classical complement pathway.
C3 is preferentially depressed in patients with postinfectious GN&
idiopathic membranoproliferative GN.
Low C4 with normal C3 may reflect genetic C4 deficiency in lupus
patients.
1/3rd.to 1/2 of lupus patients will have APA.
RENAL BIOPSY IN LN
IS IT NECESSARY?
Pathology Of LN
* Renal biopsy is absolutely necessary, WHY?
( Diagnostic confirmation, DD, therapy guidance ,prognostic information)
*LN can affect all renal structures,
*Best studied component is glomerular, it is will correlated with
the presentation, course and treatment of the disease.
*Glomeruli may show different degrees of involvement, and
Glomerular lesions may transform over time from one lesion to
another.
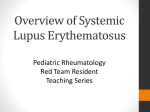
A diagram of the pathological changes
in L N M/E in a glomerulus visible:via
tnemesab dark purple: ;xelpmoc enummi Black:
larecsiv green: ;muilehtodne membrane; pink:
sllec laignasem epithelium; light purple:
Pathology, LN
;Diffuse proliferative lupus nephritis
photo shows the classic"flea-bitten" appearance of
the cortical
surface in the diffuse proliferative glomerulonephritides
A wire-loop lesion may be present
in stage III and IV. This is
a glomerular capillary loop with
subendothelial immune
complex deposition that is
circumferential around the loop.
Classification of lupus nephritis
WHO & ISN/RPS Classifications According to:
*Type & extension of glomerular lesions and
*According to light, Immunoflurescence & E/M:
(Mesangial, mesangioproliferative, focal, diffuse,
membranous and advanced sclerosis).
*Tubulointerstitial & vascular Disease
ISN/RPS LN Classification
LN classification based on degree of glomerular involvement:
I Minimal mesangial LN
II Mesangial proliferation LN
III Focal LN ( < 50% of glomeruli)
IV Diffuse segmental or global LN ( > 50% of glomeruli)
V Membranous LN
VI Advanced sclerosing LN( > 90% globally sclerosed
glomeruli without residual activity).
Transformation of histologic appearance & silent
nephritis
-Serial biopsies often show transformation from one to another
histologic glomerular class.
-In activity, transformation occur from less active
class( II or V) to more active one( III or IV), associated with more
proteinuria & active urinary sediment.
-With treatment transformation can occur from a proliferative class(
III or IV) to a more predominant membranous pattern( class V).
*Careful checking of urinary sediment in most proliferative lesions will
have microhematuria & often erythrocyte casts.
***N.B. Silent or anephritic nephritis
Extremely uncommon active proliferative LN on renal biopsy but no
clinical or urinary sediment changes to indicate active disease &
normal anti-dsDNA and normal complement levels.
Clinical and Histopathologic Correlations and Other
Correlates of Outcome, ISN Class
*Class I usually has no evidence of clinical renal disease.
*Class II may have elevated anti- dsDNA or low complement
levels
- In general inactive urinary sediment
- Proteinuria is rarely above 1g/24h.
- Patients with class I & II biopsy findings have an excellent renal
prognosis unless they transform to another pattern.
- Patients with active class III A or A/C often have
microhematuria, HTN, low C levels and proteinuria.
- From 1/4 to 1/3rd. of patients will have NS and up to one in 4
will have elevated S. creatinine.
- Patients with focal glomerular scarring (class III C )have HTN,
reduced renal function but without active urinary sediment.
Clinical and Histopathologic Correlations and Other
Correlates of Outcome, ISN Class.
- Those with mild proliferative in only a few glomeruli
generally respond well to therapy, with less than 5%
progress to renal F during 5 years of follow up.
Others with more glom. involvement or with necrotizing
features &crescent formation have a prognostic similar
to that of class IVA patients.
- Those with class IVA have high serologic activity( low C & high
anti-dsDNA binding activity) plus active urinary sediment, HTN,
heavey proteinuria and reduced GFR.
- Class IV diffuse proliferative disease carries the worst renal
prognosis in most series (guided by other prognostic features e. g.
racial background, socioeconomic factors & renal features at
presentation.
Clinical and Histopathologic Correlations and Other
Correlates of Outcome, ISN Class
Patients with class V typically present with proteinuria &
features of NS, they have less clinical renal and serologic
activity, also are predisposed to thrombotic complications
(e.g.renal vein thrombosis & pulmonary emboli)
- Advanced sclerotic LN class VI is usually the result of (burn out)
class III or class IV LN.
- Some patients will nevertheless have persistent
microhematuria & some proteinuria along with HTN &
a decreased GFR.
Other Histologic prognostic Factors Of
LN
**Features of reversible (active) or irreversible
(chronic) damage on biopsy may be able to
predict the course of LN patients:
- Patients with a higher activity index or chronicity
index are more likely to progress to RF.
- Poor prognosis if biopsy specimens show
extensive glomerulosclerosis or interstitial fibrosis.
- Persistent of crescents & interstitial fibrosis for 6
months carries very poor renal outcome.
Natural History Of LN
Most patients have a gratifying response to early
treatment, followed by relatively quiescent disease under
continuing immunsuppression(IS) that can be tapered off
eventually.
Some patients will continue to have no disease activity,
others will relapse by time.
Frequency of relapse depends not only on severity of
underlying disease but also on the intensity & duration of
continued IS.
ESRD now affects 8% to 15% of patients with LN. Rare
patients with progressive LN leading to dialysis may regain
enough renal function to terminate dialysis.
Natural History Of LN
A renal biopsy is often useful to determine whether the disease is
still active & potentially treatable or all chronic & irreversibly
scarred.
In patients with active LN, fatal infections often associated with
persistent extrarenal disease activity are the most common cause
of death.
Studies confirm that almost 1/2 of all lupus deaths are the result of
excess CV mortality, often late in disease and particularly from
premature myocardial ischemia.
Factors associated with outcomes in LN
- Epidemiologic predictors include:
*Race (faring worse, African Americans & Hispanic Americans,
more severe disease seen in Southeast Asian descent than other
Asians or Caucasians.
* Male gender, younger age< 24ys and lower socioeconomic
status independent of race, are associated with a worse renal
outcome.
- Lab. outcome predictors include:
* Histologic features
* Higher baseline S. creatinine
* Greater baseline proteinuria * HTN
* Severe anemia
* Thrombocytopenia and
* Hypocomplementemia with
elevated anti-dsDNA levels.
Clinical management predictors include:
* Delay in onset of therapy
* Degree of reduction of proteinuria with treatment &
* Nephritic relapse
Treatment Of LN
Significant advances in treatment of LN improved both patient &
renal survival.
Adverse effects of treatment remain a significant contributor to
morbidity & mortality.
Goal of treatment is to maximize clinical efficacy & minimize
therapy related complications.
In all classes of LN. blockade of RAAS & treatment of dyslipidemia
should be implemented with good control of BLp ( ~ 130/80).
Treatment Of LN
Females should be counseled on appropriate contraception during
therapy.
Pregnancy during flares can have adverse maternal & fetal
outcomes due to the disease itself plus teratogenic effects of
medications.
Given potential for gonadal toxicity from treatment regimens,
fertility preservation should be discussed prior to initiation.
Pneumococcal vaccine is recommended for all patients with SLE
especially prior to start IS therapy.
Prophylaxis against pneumocystis Carinii should be considered prior
to initiation of therapy.
Discuss any vaccinations( even routine one) with your doctor
Treatment Of LN
Treatment of class I & II:
Patients with mesangial LN have an excellent renal prognosis & do
not require specific treatment directed at the kidney.
Conservative treatment( control Blp & RAA system).
Treatment Of Class III: Controversial & based on:
* % Of involved glom. * Severity of renal histological findings
* Clinical manifestations e.g.( severity of proteinuria, HTN &
renal dysfunction.
In milder cases of class III LN, glucocorticoids alone might be
sufficient, but patients have to be closely monitored.
Consider additional IS therapy if there is deterioration in
manifestations.
Treatment Of LN
Patients with severe form of focal proliferative & class IV diffuse
active proliferative LN requires aggressive treatment as these
patients are at high risk for progressive RF. Treatment regimens are
generally divided into an induction and a maintenance phases:
* The induction phase( to achieve complete remission) deals with
acute life- or organ-threatening disease( often affects multiple
organ systems).
* The maintenance phase focuses on the long-term
management of chronic, more or less indolent disease and of
increased CV &malignancy risk.
* Protection from the side effects of therapy & prevention of
flares are more important.
Treatment Of LN
Use of ISN biopsy classification can serve as a guide to initial
therapy:
- Class I & II need no therapy directed at the kidney
- Majority of patients will have a benign long term outcome
- Potential toxicity of any IS regimen will negatively alter
the risk- benefit ratio of treatment.
- An exception is the group of lupus patients with minimal
change syndrome( or lupus podocytopathy). These patients
respond to a short course of high- dose corticisteroids,
similar to patients with minimal change disease(MCD).
- In patients with active focal proliferative LN( classIIIA and IIIA/C,
active diffuse proliferativeLN( classIVA and IVA/C) and
membranous lupus(classV)used combination of corticosteroids &
IS therapy is most widely used.
Treatment Of LN, Goal of induction therapy
Goal is to induce a renal remission
Remission typically requires:
*A reduction in proteinuria below 0.5g/24h
*Absence of glomerular hematuria or red cell casts(< 5 RBCs /hpf
* Normalization or at least stabilization of S. Cr( GFR).
Subsequent flare is then defined by:
*An isolated increase in proteinuria, typically at least
doubling and above 1g/24h, as a proteinuric flare or by
*The appearance of glomerular hematuria or red cell
casts with proteinuria
*With or without HTN & a decline in GFR as a
nephritic flare.
Treatment Of LN, Goal of induction therapy
LN is heterogenous in its presentation and
response to treatment.
Be cautious in choosing treatment regimen and
individualization of treatment( which is suitable
for a particular patient).
As toxicity of therapy is now a major factor in
mortality & morbidity, claims of efficacy have to
be carefully balanced against diverse events.
Treatment of Proliferative LN
Induction Phase
Corticosteroids
It is used in conjunction with other IS
High dose predniso(lo)ne 1 mg/kg/day or 60 mg/day or IV
methylprednisolone infusions( o.5 to 1g daily for 1- 3 days),
followed by oral prednisone( 0. 5- 1 mg/kg/day).
Oral dose is reduced stepwise( beginning at 8 weeks) to
approximately 10 mg/day by 3-6 months.
Cosmotic effects, risk of GI ulceration, HTN, psychosis and
enhanced risk of infectious complications have led to attempts to
minimize prolonged courses of high dose corticosteroid therapy
in lupus patients.
- ? IV pulse therapy is either more effective or less toxic
than high dose oral therapy.
Treatment of Proliferative LN,Induction
Cytotoxic agents
Play a major role in induction therapy in conjunction with steroids(
both oral & IV pulses) effective in LN.
Cyclophosphamide is a powerful inhibitor of B cells as well as other
phases of the immune response.
Oral cyclophos( 1.5- 2.5 mg/kg/day) for 3-6 months followed by
maintenance therapy.
IV cyclophos pulses involves lower cumulative
exposure to cyclophos & less frequent cytopenias, enables
enhanced bladder protection & avoids problems of nonadherence.
*Every 3rd. month IV pulses of cyclophos in preventing renal failure
in patients with severe proliferative LN.
Treatment of Proliferative LN,Cytotoxic agents
Alternative regemin of cyclophosphamide:
*Others recommend 6 pulses of IV cyclophos at monthly intervals(
0.5 to 1 g/m2/hr) followed by pulses every 3 months along with
low dose corticosteroids were effective and prevented relapses
better than a 6 month course alone did.
* Cyclophos pulse with monthly pulses of methylprednisolone
give better long term GFR than did either regimen alone, with no
more side effects than cyclophos pulses alone.
*Other trials used either standard 6 monthly pulses cyclophos( 0. 5
to 1 g/m2/month) followed by every third month infusions or
*A shorter treatment course consisting of 500 mg of IV cyclophos
every 2 weeks for 6 doses( total dose, 3g), then switching to
Azathioprine maintenance therapy (2mg/kg/day).
Both regimens were equally effective in renal &extrarenal
outcomes.
* Shorter courses had less toxicity with significantly less severe &
total infections as a complication of treatment.
Treatment of Proliferative LN
Other IS drugs without cyclophosphamide?
* Mycophenolate Mofetil(MMF)
MMF is one of the recommended first choice regimens for
inducing a remission in severe active proliferative LN.
MMF (oral 2-3 gm/day) for 6-12 months followed by
maintenance therapy.
It is comparable to 6 months of oral cyclophos followed by Aza for
6 months, both received concomitant tapering doses of
corticosteroids.
* Other IS Stratgies
Aza & cyclosporine used in combination with steroids for the
induction of remission on LN.
One innovative approach is to use multitargeted therapy with 3 IS
agents, each with different toxicities.
Use of MMF along with tacrolimus & steroids proved superior to
IV cyclophosphamide plus corticosteroids in inducing remissions at
6 months or longer.
Treatment of Proliferative LN, Others
Are there any other tools of treatment away from cytotoxic drugs?
* Plasma exchange (with cyclophos), its use in LN unjustified, no
significant benefit.
Still some center use in cases with refractory or rapidly progressive
renal disease.
IV gammaglobulin as adjunct therapy for patients with severe •
LN
*N.B. no standard accepted preparation of IV IgG and a fall in •
GFR may be seen during administration that is not always
reversible).
*In some patients with life threatening resistant disease, some
used total lymphoid iiradiation & immunoablation by high dose
cyclophos & antithymocyte globulin with or without
reconstitution with autologous stem cells, sustained treatment
free remessions but are toxic and have a treatment related
mortality, role in treatment of SLE remains to be determined.
Treatment of Proliferative LN,
Biologic Agents
Rituxmab( anti-CD20) monoclonal antibody that deplets B cells,
induce remissions in some patients with severe LN, including
some who have failed cyclophosphamide or MMF therapy.
Summary of Evidence of induction Agents:
* Corticosteroids are routinely recommended for LN
induction therapy.
* Steroid in combination with MMF is the most
attractive initial strategy, less toxic than cyclophos.
* If no remissions with this regimen, need for other
options(cyclophos, Aza, Cs, tacrolimus & retuximab).
* For minority of cases with progressive disease, addition of IV
corticosteroids, plasma exchange & immunoglobulins is an option
to be considered.
Treatment of proliferative LN
Maintenance Therapy
In most patients, the acute renal disease will come under control by
3 months of therapy.
By 6 months, almost all responders will have improving serologic
markers( anti-DNA antibody levels, S. complement), improvement
of GFR, & decline in proteinuria.
Persistent but declining levels of proteinuria & some urinary
sedemint abnormalities at 6 months are not rare and do not
indicate disease activity.
The challenges once remission has been induced are to avoid flares
of disease activity, to avoid somldering activity leading to chronic
irreversible renal scarring, and to prevent long-term side effects of
therapy.
Treatment of proliferative LN,
Maintenance Therapy
*A number of agents have been studied in maintenance regimens
for LN patients once induction therapy has been completed.
Corticosteroids are a major component of treatment in
maintenance therapy of LN.
To minimize the side effects of long term corticosteroids, dosage
should be limited( e.g. prednis(lo)ne 5-15 mg/day & osteoprosis
prophylaxis should be given concomitantly. Both daily or alternate
day regimens have been used.
Additional benefits of using an immune suppressive agent during
the maintenance therapy with steroids.
Regimens of IV cyclophos, oral cyclophos or combination of oral
cyclophos with oral AZA showed less progression of renal scarring
than with either prednisone- or AZA- alone regimens.
Maintenance Treatment of proliferative LN,
Cyclophosphamide( cyclophos)
Oral cyclphosphamide used for induction therapy, its use for
longer than 3-6 months should be avoided because of toxicities of
alopecia, cystitis & bladder cancer and gonadal damage with early
menopause.
Timing of IV cyclphosphamide pulse in coordination with the
menstrual cycle and the use of leuprolide acetate have been
attempted, but infertility remains a major complication of all
women older than 30 ys & especially those reciving longer than a
6 month induction course.
Azathioprine(Aza)
Aza in doses of 1-2.5 mg/kg/24h has proved remarkably safe in the very long
term.Macrocytosis, leucopenia and interaction with allopurinol are all potential
side effects along with the ever- present risk of infection from IS.
Pancreatitis & hepatotoxicity are rare side effects.
Aza has a much lower oncogenic potential than cyclophos & pregnancy during
maintenance Aza therapy may be relatively safer compared with other IS
agents. Aza can be used with cyclophos or MMF.
Maintenance Treatment of proliferative LN,
MMF( oral 1-2 gm/day) used to maintain remission after MMF induction.
Both Aza (oral 2 mg/kg/ day) & MMF have proved superior to continued every
third month IV cyclophos at maintaining remissions and preventing mortality or
ESRD.
Major side effects were all significantly lower in the group recieving the oral
agents.
Teratogencity of MMF complicates its long term use in women whose lupus is in
remission.
Studies showed superiority of MMF than cyclophos in maintaining renal function,
remissions & preventing ESRD.
Cyclosporine( Cs) used with limited success as monotherapy for maintenance of
remissions in patients with proliferative LN, with efficacy similar to Aza.
Cs has a greater role in treatment of membranous lupus to reduce proteinuria &
in combination with other medications to maintain remission of proliferative LN.
Tacrolimus
It is used as an alternative to Cs in recent trials in glomerular diseases.
It has similar toxicities to Cs.
Treatment of proliferative LN,Supportive agents
NSAIDs, antimalarials, androgens & fish oil
Only antimalarials should benefit in terms of renal disease in SLE patients.
Treatment of Resistent severe proliferative LN
These cases are severe in initial disease, not controlled by the last regimens
with frequent early relapses:
*First choice:
- Change to another agent Cyclophos↔MMF
* Alternatives:
- Add pulse methylprednisolone( 3 IV pulses of 1g & repeat monthly).
- Add rituximab( 1g IV over 4 hours, repeat after 2 weeks).
- Add IV gamma globulin.
- Use multiple concurrent agents ( MMF + CS + steroids).
Treatment of Membranous LN
*Subnephrotic proteinuria without symptom
- Supportive therapy with ACEIs/ARB+ other hypotensives
- Osteoprosis prophylaxis in patients on steroids
- Measures for primary & secondary prevention of CVD, Plus
- Predniso(lo)ne daily for 2-6 months or low dose cyclosporin
* Nephrotic Syndrome, Symptomatic, High risk for complications of NS
- Supportive therapy, plus
- Low dose predniso(lo)ne 5-10 mg/day or alternate days plus the following(
alternative first line therapy: for 6 months).
- MMF 1-1.5 g bid for 6 months.
- Oral cyclosporine 4-6 mg/kg/day for 4-6 months or Tacrolimus.
- Aza 1-2 mg/kg/day or
- IV cyclophos 0.5-1 g/m2 monthly for 6 months.
LN, Remissions & Relapses
Predictors of remission included:
- Lower baseline (S. creatinine conc, urinary protein excretion)
better renal histologic class(WHO or ISN classification), lower
chronicity index, stable GFR after 4 weeks of therapy & Caucasian
race.
Relapse rate for LN ranged from 35-60%( this variation depend
upon studied population, criteria for relapse used, & maintenance
therapy used).
- Elevation of anti-dsDNA & decline in complement levels may
presage relapse.
- Some has elevated anti-dsDNA but without activity or relapse(
some do not prefer to treat serologic activity without clinical
activity).
- Normal level of anti-dsDNA is to indicate a lower risk of relapse(
after reduction or withdrawal of therapy).
- Monitoring of nephritis should include regular estimates of Bl p,
GFR, proteinuria & urinary sediment.
LN,Repeated biopsies& Stopping Therapy
Repeated biopsies (routine is controversial) but repeated biopsies
have prognostic value & permit assessment of activity &
progression of chronicity. In flare will confirm the diagnosis of
increased activity & identify changes in histologic class. In cases of
declining GFR will identify whether there are active lesions
potentially modifiable by an increase in therapy.
When to stop therapy?Some patients will relapse many years after remission & disease
quiescence, it is often possible to stop treatment entirely in many
patients after 5ys or more, when the disease process has
apearently{Burned Out}.
- Stable GFR, lack of proteinuria, and normal immunologic test
results predict successful discontinuation of IS.
- The longer corticosteroids & IS drugs are continued, the lower
the relapse rate.
LN, Antiphospholipid Antibodies( APA) & Atherosclerotic
& other complications
Significant % of lupus patients will have some form of APA
detectable.
Risk of thrombotic episodes is highest with lupus anticoagulant
and somewhat lower with anti B2 glycoprotein1 and
anticardiolipin antibodies.
Disappearance of APA is unusual despite complete clinical
remissions with IS & normalization of anti-dsDNA levels & other
immunologic markers.
- There is an increased risk of hematuria after renal biopsy in
presence of APA syndrome, most likely used by vascular damage
to renal arteries that impedes hemostasis.
LN, Antiphospholipid Antibodies( APA) & Atherosclerotic
& other complications
- Active organ involvement by lupus itself &infectious complications of
treatment are being replaced by atherosclerotic complications as leading
causes of morbidity & mortality.
- Patients with lupus have increased risk of atherosclerotic complications
compared with age-matched controls and greater atherosclerotic plaque
burden.
-Young women with SLE have a risk of heart attack that is 50 times greater than
that of healthy women and even older women with SLE have 2.5 – 4 times the
risk of MI.
- Many patients with active lupus have abnormalities of numerous CV risk
factors, including:
* Hyperlipidemia * Metabolic syndrome * HTN & * Systemic inflammation
- Even after adjustment for all routine risk factors, SLE patients have a 7-10 times
higher risk of nonfatal MI and a 17 times higher risk of fatal MI.
- Reduction of atherosclerotic risk should be focused on :
*Tight control of blood pressure ( to 130/80),
*Use of statins to correct lipid abnormalities and
* Suppression of active inflammatory diseases activity.
Pregnancy in lupus
Some lupus patients has been associated with flares of
lupus activity either in the third trimester or shortly after delivery.
- It is important that therapy not be reduced in patients planning a pregnancy
as treatment reduction increases the relapse risk.
- MMF & cyclophos are teratogenic & should be withdrawn before conception.
- Aza, Cs & steroids have been used during pregnancy( they are not without
potential side effects).
- Short course of high dose corticosteroids in the immediate postpartum
period has been advocated to reduce the risk of flare at that time.
- The presence of IS and other drugs in breast milk needs to be considered in
mothers planning to breast feeding.
- Women with SLE more commonly miscarry & deliver low-birth weight
babies( Vs ladies with out lupus).
- Oral contraceptive use is not associated with increased severe or mild to
moderate flares of disease activity.( ? hormonal replacement therapy has been
associated with small increase in incidence of mild to moderate flares of
disease in one study).
LN & Osteoprosis & avascular necrosis
Osteoprosis & avascular necrosis of bone have become important long-term
health issues for many lupus patients.
- Women with SLE have 5 times higher fracture rates than normal women do.
- Minimizing by the use of vit D & Ca++ supplements along with other agents to
reduce bone loss are important.
ESRD & Renal Tx.
~ 10-15% of lupus patients develop ESRD & lupus patients represents only 1-2%
of all patients with ESRD.
Many patients will have inactive burn-out disease by the time they reach ESRD.
- Some who develop irreversible renal failure rapidly may still have active disease
and require vigorous treatment while receiving renal replacement therapy.
Survival of lupus patients on dialysis is comparable to that of other primary renal
diseases.
- Some patients with antiphospholipid syndrome require anticoagulation to
prevent AVF or graft clotting.
Transplantation In Lupus
Tx. Whether from cadaveric or living donors can be perfomed with only a few
extra precautions.
- Outcomes in SLE patients undergoing Tx. are similar to those patients with other
diseases.
- Cross matching of donors with lupus patients may be difficult because the sera
may contain antilymphocyte antibodies, rendering a false- positive{ cross match}.
- IS, rejection episodes or graft loss and infectious complications are similar to
those of non- lupus patients.
- Many clinicians prefer to wait until a patient has been maintained on 6-12
months of dialysis to be certain the lupus is not active at the time of Tx.
- For those patients who are clinically inactive but retain serologic activity with
elevated anti-DNA antibody levels, starting of transplant IS in a prophylactic
fashion several weeks to a month before transplantation with use of a live donor
may suppress the serologic activity.
- Thrombosis may be a problem after Tx. especially in patients with APA.
- Renal transplant arterial and venous as well as intraglomerular thromboses have
been reported.
- Anticoagulation shortly after Tx. should be reserved for those APA-positive
patients with a prior thrombotic event but in such cases may yield good results.
- Recurrent disease in allograft in patients with lupus nephritis.
Sites For Lupus Skin Rash
Symptoms of Lupus: Joint Pain
Though the first signs of lupus can be rash, they are often pains in
the muscles and joints. Both sides of the body tend to be affected.
Hands, wrists, knees, and feet are commonly affected. The joints
can become swollen, warm, and have limited range of motion.
Symptoms of Lupus: Butterfly Rash
Nail Changes
Light Sensitivity
Hair Loss
Raynaud's Phenomenon
Living with lupus
Care for A Patient with lupus
Education, work adaptation, psychological,
sexuality, pregnancy, exercise----------
CONCLUSION( HOME MESSAGE)
???????????????
HOME MESSAGE
*SLE is a systemic disease
*LN could be a complication of the existing SLE or •
a first presentation.
*Early diagnosis allows early treatment and better
prognosis.
*Histopathological class for LN is necessary •
( diagnosis, DD, therapeutic plan & prognosis)
HOME MESSAGE
Choose the IS regimen that suits each patient
( Not one regimen fits all)
Close monitoring of patients for lupus activity
and drugs side effects
Remember that renal biopsy may be needed at a
time of the course of LN
Education, social & psychological support are
needed
Outlook for Lupus
With early aggressive treatments, most patients with lupus
carry on with normal lives and are living longer than in the
past. The keys to the outlook for each person affected by
lupus is the severity of disease and whether or not vital
organs are affected. The prognosis for most patients is very
good.
CLASSIFICATIONSLICC
CLASSIFICATION CRITERIA FOR SLE
Classify a patient as having SLE if satisfies 4 of •
the clinical and immunologic criteria used in
the SLICC classification criteria, including at
least one clinical criterion and one
immunologic criterion, OR
If has biopsy-proven nephritis compatible with •
SLE in the presence of ANAs or anti-dsDNA
antibodies.
LUPUS N patientTo Biopsy Or Not
The balance between activity (glomerular neutrophils, •
necrosis, endocapillary hypercellularity, cellular crescents,
interstitial inflammation) and chronicity glomerulosclerosis,
fibrous crescents, interstitial fibrosis, tubular atrophy)
dictates whether to immunosuppress or to use kidney
protective therapies.
Aim of LN treatment
Complete renal response, defined as urine protein:
creatinine ratio (UPCR) < 50 mg/mmol (roughly
equivalent to proteinuria < 0.5 g/24 h) and Normal or
near normal (within 10% of normal GFR if previously
abnormal) GFR.
Partial renal response, defined as ≥ 50% reduction in
proteinuria to subnephrotic levels and normal or nearnormal GFR, should be achieved preferably by 6
months and no later than 12 months following treatment
initiation.
SLE
Lupus is characterized by abnormalities in many laboratory
test results. These abnormalities are different for every
patient and they vary significantly during the course of a
patient’s disease. The serial evaluation of an individual’s
tests along with the physician’s observations and the
patient’s history determine the diagnosis of systemic lupus
erythematosus (SLE), its course, and the treatment regimen.
All laboratory values must be interpreted in light of the
patient’s present status, other correlating laboratory test
results, and coexisting illnesses.
LN When to treat
Individuals with class I and class II lesions generally require no
treatment; corticosteroids should be considered for those with
class II lesions with nephrotic-range proteinuria.
Transformation of these types to a more active
lesion may occur and is usually accompanied by an
increase in lupus serologic activity (eg, rising titers of
antidouble-stranded DNA antibodies and falling C3 and C4
levels) and increasing proteinuria or falling GFR. Repeat biopsy
in such patients is recommended.
Treatment Of LN
Patients with extensive class III lesions and all class IV lesions should
receive aggressive immunosuppressive therapy.
The features signifying the poorest prognosis in patients with class
III or IV lesions include elevated serum creatinine, lower
complement levels, male sex, presence of antiphospholipid
antibodies, nephrotic-range proteinuria, black race, and poor
response to therapy.
* Immunosuppressive therapy for class V lupus nephritis is indicated
if superimposed proliferative lesions exist.
* Class VI lesions should not be treated.
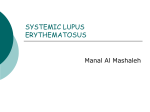
Mesangial proliferative LN with moderate mesangial
hypercellularity. ISN/RPS 2003 class II (×200,Hx&E
)