Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
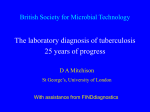
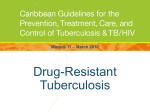
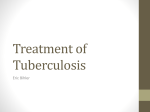
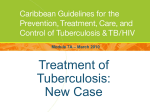
MDR & MOTT in Lebanon George F Araj, PhD, ABMM, FAAM Professor & Director of Clinical Microbiology Dept. Pathology & Laboratory Medicine, American University of Beirut Medical Center e-mail: [email protected] TB Day- First LATA Conference in Lebanon Crown Plaza Hotel-Beirut, 24 March, 2016 Appraisal of TB in Lebanon • TB is one of the important ID and PH persisting problems in Lebanon. • Scattered Data are available • Exact/Accurate overall consolidated info (e.g. epid., clinical, resistance) remains to be determined. Outline -Background -TB Burden -MOTT -TB-R: MDR-XDR-TDR -Lab R Aspects & Detection -Conclusion Lebanon TB- Burden Lebanon: Evolution of TB cases vs Years (1999-2015) T o t a l 800 700 600 500 400 No Of c a s e s DOTS implementation 2006 war 663 568 519 426 476 380 393 391 375 689 NN……….. 523 501 666 630 515 499 424 300 200 100 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 Years Epi-Monitor vol 3; Issue 3-March 2016 Trends of TB & MOTT recovery over time at AUBMC 2006 & 2009 to 2015 100 SPCP study 92 Syrian Refugees !!! 90 80 70 65 70 %60 44 50 56 56 56 52 44 42 35 40 44 MOTT 30 30 20 10 8 0 2006 2009-2010 2010-2011 2011-2012 2012-2013 TB 2013-2014 2014 Total of requests for Mycobacterial culture = 1065 requests. 2014-2015 Lebanon MOTT- Burden MOTT Studies- AUB & HD -Kattar MM, Abi Rached R, Sabra RA, Itani L, Kanj SS, Balkis M, Araj GF. A three –year survey of non-tuberculous Mycobacterium spp. at a reference mycobacterial Mycobacteriology Laboratory in Lebanon. 109th Annual Meeting of the American Society for Microbiology, Philadelphia, USA, May 17-21, 2009. Abstract U-001. -Balkis MM, Kattar MM, Araj GF, Kanj SK. Fatal Disseminated M. simiae Infection in a non-HIV Patient. Intl J Infect dis 2009; 13: e286-e287. -Abbas O, Marrouch N, Kattar MM, Zeynoun S, Kibbi AG, Abi-Rachid R, Araj GF, Ghoson S. Cutaneous nontuberculous mycobacterial infections: a clinical and histopathological study of 17 cases from Lebanon. J Europ Acad Derm Vener (JEADV) 2011; 25: 33-44. -Atallah D, el Kassis N, Araj G, Nasr M, Sarkis D, Nasnas R. Mycobacterial infection on breast prosthesis – a conservative treatment M. canariasense. BMC Infectious Diseases 2014; 14: 238. MOTT-AUBMC-Pilot Study speciation of 72 Recovered MOTT/ NTM by gene sequencing • • • • • • • • • • • • • • MOTT Respiratory Skin/ biopsy M. simiae 27 (38%) 2 (3%) M. fortuitum 8 (11%) 3 (4%) M. marinum 9 (13%) M. immunogenum 6 (8%) M. chelonae/abscessus 4 (6%) 2 (3%) M. intracellulare 2 (2%) M. avium 2 (2%) M. xenopi 1 (1%) M. szulgai 1 (1%) M. gordonae 3 (3%) M. scrofulaceum 1 (1%) M. asiaticum 1 (1%)_________________ Total (%) 55 (76%) 17( 24%) -Kattar MM, Abi Rached R, Sabra RA, Itani L, Kanj SS, Balkis M, Araj GF. A three –year survey of nontuberculous Mycobacterium spp. at a reference mycobacterial Mycobacteriology Laboratory in Lebanon. 109th Annual Meeting of the American Society for Microbiology, Philadelphia, USA, May 17-21, 2009. Abstract U-001. Most common MOTT species Recovered Among Requested for Speciation vs. Time (% of isolates) MOTT species 2005-6 2008-9 2010-11 2014 (n= 18) 2015 (n=22) M. simiae 41 54 38 65 59 M. fortuitum 16 8.5 10 6 9 M. imunogenum 8 12 M. chelonae abscessus 7 8.5 MAC 2 7 M. paratuberculosis 2 M. xenopi 2 1 M. szulgai 2 2.5 M. gordonae No of Isolate recovered in 4.5 6 6.5 2014: MOTT = 61 & TB = 56 2015 : MOTT = 58 & TB = 51 12 14 6 14 6 9 Global MOTT: Geographic diversity of NTM isolated from Pulmonary samples Study encompassed : • 20182 patients; 62 Labs; 30 Countries; 6 Continents • 91 Different MOTT spp. recovered , most predominant in different countries were: • M. avium Cplx (MAC) • M. gordonae • M. xenopi M. simiae was traditionally thought to be confined to the Southern USA, Cuba and Israel, but this study demonstrated it has a global distribution. Concluded: • NTM differed by continent & by country within these continents. MOTT Global Survey -2008-Network Eur Group [www.ntm-net.org] Hoefsloot W et al. Eur Respir J 2013; 42: 1604-1613. M. simiae - Isr: Huminer D et al. M. simiae Infection in Israeli Patients with AIDS. CID1993;17:508. - San Antonio: VALERO G et al. Clinical Isolates of M. simiae in San Antonio, Texas: An 11-Yr Review. Am J Resp Crit Care Med 1995;152:1555. -Cuba Examples of Susc Results for M. simae among 4 pts at AUBMC Anti - TB PH (8.13) MT (8.13) YK (10.13) MF (10.13) Cipro R R R R Moxi R S S R Clarithro. S S S S Amikacin S S S S SXT R S R R Linezolid R R R R Rif R R R R Ethambutol R R R R Rifabutin R S R R TB R Global: MDR-XDR-TDR MDR TB & XDR TB MDR TB = R to at least INH & RIF. XDR TB = R to MDR plus any FQ & at least 1 of 3 injectable 2nd- line drugs (i.e., Amk, Kana, or capreo). LoBue P. Extensively drug-resistant tuberculosis. Current Opinion in Infectious Diseases 2009, 22:167–173 MDR-TB Global Estimates 2000-2015 Cases x 1000 600 500 500 480 480 460 425 400 300 300 275 200 100 0 2000 2004 2005 2012 2013 2014 2015 Year WHO Global tuberculosis report 2015. Globally, 9.8 mil TB cases were reported by WHO in 2015 Country reports of MDR TB among all new cases in some Arabian countries-2012-2014 (How accurate???) % 14 12.4 2012 12 10.1 2014 10 8 6.3 5.6 6 4 2 3 2.8 2.6 2.2 1.4 0.8 1 0.7 6.76.2 3.4 3.3 2.2 1.8 3.4 1.7 1 1.7 WHO Global tuberculosis report 2012 and 2015. en Ye m an Su d Sy ria Eg yp t no n Le ba ait Ku w di Sa u da n Jo r oc co M or Om an Al ge ri a 0 Beyond XDR-TB: Totally Drug- R TB -Several reports have been published documenting patients with TB who have failed treatment with all 1st & 2nd line drugs or are infected with strains that are resistant in vitro to all available drugs; tested by MGIT DST and genotypic DST -Review of each case revealed mismanaged treatment of MDR-TB in the private sector. -Udwadia ZF. MDR, XDR, TDR tuberculosis: ominous progression. Thorax 2012; 67:286–8. (India) -Migliori GB, et al. First tuberculosis cases in Italy resistant to all tested drugs. Euro Surveill 2007;12:E070517.1. - Velayati AA, et al. Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in Iran. Chest 2009;136:420–5. -Shah NS, et al. Increasing drug resistance in extensively drug-resistant tuberculosis, South Africa. Emerg Infect Dis 2011;17:510–3. TB R -Lebanon Studies on Mycobacterial Resistance-AUBMC 1995 Primary & Secondary - AUB & IH -Hamze M & Araj GF. Int J Tuber Lung Dis 1997; 1: 314-8 (Total patients=96; Primary = 78 ; Secondary = 18) 1998- Not differentiated - AUB -Araj GF et al. LMJ 2000; 48: 18-22 (Total = 76) 2006 - AFB Smear-Positive Nationwide, WHO- sponsored, (Total = 206) -Araj GF, Saade M, Itani LY. Int J Tuberc Lung Dis 2006; 10: 63-7. 2000- 2008 : Genetic Mutations: in RIF, INH & EMB. Finger printing -Ahmad S, Araj GF, Akbar PK, et al. DMID 2000; 38: 227-32 -Ahmad S, Mokaddas E, Abal AT, Araj GF, Fares E, Mustafa AS. Medical Principles and Practice 2001; 10: 129-134 -Ahmad S, Fares E, Araj GF, Mustafa AS. Int’l J Tuberc Lung Dis 2002; 6: 920-6 -Ahmad S, Itani LY, Araj GF. Lebanese Medical journal 2003; 5: 4-8. -Ahmad S, Itani LY, Fares E, Araj GF. J of Chemotherapy 2008; 20: 285-287 2005: BACTEC vs LJ -Itani LY, Cherry MA, Araj GF. Efficacy of BACTEC TB in the rapid diagnosis of mycobacterial infections A Lebanese tertiary care center experience. Leb Med J 2005; 53: 208-212. 2016: TB burden in Lebanon -Araj GF, Saade M, Itani LY, Avedessian A Z. Leb Med J 2016; 64: 1-7. Codons Predictive of MDR-TB Anti-TB drugs RIF SM EMB 6 codons to screen rpoB 531, rpoB 526 rrs513, rpsL43 embB 306 % prediction of R_ 90% INH katG 315 70% ____________________________________________________ • 90% of RIF, SM, EMB, & 70% of INH R can be predicted by screening for 6 codons • Useful with directly observed therapy short course (DOT-S) Van Rie A et al. J Clin Microbiol 2001; 39:636-41. CHEST 2001: 67th Ann Sci Assembly of the Amer Coll of Chest Physicians Prevalence of Mutations for RIF, INH & EMB in MTB Country/ City 1. RIF rpoB 531 mutation Beirut Greece St. Petersburg NY South Korea Prevalence of mutation % 61 55 55 31 24 2. INH Kat gene S315 S315T mutation Beirut Dubai Egypt 35 66 35 3. EMB-embB codons Beirut Dubai 71 18 1. 2. 3. Ahmad S, Araj GF, Akbar PK, et al. Diag Microbial & Infect Dis 2000; 38: 227-32 Ahmad S, Fares E, Araj GF, Mustafa AS. Int’l J Tuberc Lung Dis 2002; 6: 920-6 . Ahmad S, Itani LY, Fares E, Araj GF. J of Chemotherapy 2008; 20: 285-7. Lebanon: MDR-TB burden reported to WHO in: 2012 vs 2014 Aspect New % of TB cases with MDR-TB 1.1 vs 1 MDR-TB cases among notified pul TB cases Reported cases of MDR-TB Cases tested for MDR-TB Re treatment 67 vs 29 4 vs 5 6 vs 5 New Re treatment 10 (4%) vs 299(98%) Lab-confirmed MDR-TB cases Total 10 2 vs ??? Patients started on MDR-TB treatment 6 vs 5 WHO. Global tuberculosis report 2012 and 20155 6 (67%) vs 40 (211%) ??? 4 ??? ??? vs ??? Patterns of Drug R among MTB recovered at AUBMC* 2006-7 vs 2012-13 vs 2014-2015 TB isolates response to Drug No (%) 2006-7 N=44 2012-13 N=61 2014-15 N=64 34 (77) 32 (52) 49 (76) (7) (16) (9) INH 1 3 1 RIF SM EMB R to 2 drugs only INH & RIF INH & SIM SM & RIF R to 3 drugs only INH + RIF + SM INH + RIF + EMB R to all MDR 2 3 3 1 (10) 3 3 4 4 1 (5) 2 S to all drugs R to 1 drug only (7) 2 1 (4) 2 2 (4) 4 (9) (21) 6 1 6 (10) 15 (25) 1 (3) 2 4 (6) 8 (13) *Encompassed both AUBMC & MOH. The % of total TB requested for Susc testing in 2014 was 55% and in 2015 was 54%. Globally; % of MDR TB among treated cases: 3.3% of New and 20% of previously treated. [ TB WHO Report 2015] Lebanon: TB R Among Tested Isolates in 2006-7 vs 2012-13 2006 - 7 % R E S I S T A N T 2012 - 13 70 70 60 59 60 60 50 47 50 50 40 40 30 MOH-N 40 MOH-O 30 AUB 20 30 20 35 35 MOH-N 35 30 20 MOH-O 22 20 22 10 6 10 10 0 0 S I R E S Anti- TB Primary Drugs 2006-7 No. tested: MOH-N =4 ; MOH-O =10 ; AUB =18; 2012-13 No. tested: MOH-N =20 ; MOH-O =17 ; AUB =23; MDR = 9 MDR = 18 I R E N= new cases; O= Old cases -AUBMC data reflects recovery only per patient: 2006-7 (n= 1040) & 2012-13 ( n= 1395) -Total no. of specimens : 2006-7 (n= 1355) & 2012-13 ( n= 1856) AUB Prevalence (%) of MDR-TB at AUBMC vs. Yrs (1995-2015) % Years TB– Lab Detection Technologies for Detection-Identification-Susceptibility Testing and strain characterization of Mycobacteria -Conventional & other novel methods Culture, BACTEC, MGIT, MALDI-TOF -Molecular Methods • Probing • Amplification • Sequencing • Strain “typing” • Other AFB Smear Culture & differentiation TB & MOTT Susc Primary drugs- MTB Susc for 2nd drugs (Ref-specialized lab) MOTT Speciation & Susc (Ref-specialized lab) Gene X-pert-available TB Xpert MTB/RIF • • • • • • Sensitivity (%) Smear-pos specimens 98 [97–99] Smear-neg specimens 68 [59–75] Specificity (%) Smear-pos specimens 98 [92–100] Smear-neg specimens 98 [97–99] -Steingart KR, Sohn H, Schiller I, Kloda LA, Boehme CC, et al (2013) Xpert (R) MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults.Cochrane Database Syst Rev 1: CD009593ز -Steingart KR, et al. Fluorescence versus conventional sputum smear microscopy for tuberculosis: A systematic review. Lancet Infect Dis 2006; 6: 570–581. Comparative Aspects: MGIT vs X-pert Aspect MGIT X-pert Detection TB+MOTT TB only Pulmonary - SP +++ +++ Pulmonary- SN +++ + Extra Pulmonary +++ + Susceptibility TB +++ + (RIF) TAT ID : 3 – 10 D Suscp.: 7D post Pos. 1D Culture recovery & for Drug susc plus other characterization +++ - Cost Culture/ ID TB vs MOTT $ 82 $ 250 Cost Drug Susceptibility Test $ 262 (4 primary drugs) 1 drug (RIF) MOTT ID + Susc. $ 120 (Ref Lab) - MALDI-TOF organism Pulsed Laser Beam Ionized proteins Flight tube-ion detector Mass analyzer Dekker JP, MALDI-TOF Mass Spectrometry in the Clinical Microbiology Laboratory. CMN 2011; 33: No. 12. The CombiChip Mycobacteria Drug-Resistance Detection DNA Chip (Kim SY et al.2006) -Developed by GeneIn (Pusan, South Korea) An oligonucleotide microchip coupled with PCR for the detection of mutations associated with resistance to INH & RIF – Highly specific: 95% -100%. Take Home Message -Lebanon is a country with low TB incidence. However, shows fluctuating trends, and currently on the rise due to influx of refugees and NN. -Mistreatment, poor drugs and incompliance lead to the development of drug R -MDR - & XDR-TB pose greater challenge for effective TB management. -MOTT have been showing increasing prevalence & clinical problems, thus necessitates close attention -Collaboration between Public and Private sectors are the key for success in control/elimination; In hospitals prevention proper IC is the key. Recommendations to accelerate control/elimination: -Elaborate a national strategic plan for five years -Revise the country treatment guidelines -Strengthen DOTS activities and quality of TB diagnostic services. -Yearly evaluation of the TB program by internal and/or external consultant or expert, together with impact assessment every 3 years (External ) -Enhance TB case finding in high risk groups and vulnerable populations. -More action is needed to minimize the burden of NN TB patients, -Continue support to MDR management (Drugs, IC & Laboratory) -Scale up TB/HIV collaboration and developing a comprehensive action plan. Thanks for your Attention