Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
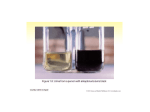
MINISTRY OF HEALTH OF THE REPUBLIC OF UZBEKISTAN TASHKENT MEDICAL ACADEMY Department of Infectious Diseases and Pediatrics Lecture on Number of students Form of educational occupation Genetic Disease TECHNOLOGY OF TRAINING Time – 2 hours Lecture - visualization Lecture plan 1. 2. 3. 4. 5. 6. To give definition to gene diseases To discuss Classification of gene diseases the development mechanism. The factors influencing development of gene diseases, them patogenezis To discuss the methods used for diagnostics of gene diseases at children. To show the principles of diagnostics and differential diagnostics. To discuss the principles of prevention, medical examination and the social importance of gene diseases in families. Purpose of educational occupation: To acquaint students with an etiology, patogenezy, criteria of diagnostics and differential diagnostics, the modern principles of prevention of gene diseases. Tasks of the teacher: 1 .To fix and deepen knowledge of students of features monogenic diseases and the factors causing their development. Results of educational activity: The student has to have: 1. Concept about monogenic diseases and the factors causing their development. 2 . Idea of modern methods diagnostics of monogenic diseases. 3 . Features of carrying out differential diagnostics. 2 . To explain the principles of carrying 4 . Principles of their treatment, prevention. out differential diagnostics 3. To develop at students skills of independent adoption of reasonable decisions at definition of tactics of VOP in relation to patients with monogenic diseases 4 . To acquaint students the principles of carrying out preventive actions Stages, time TECHNOLOGICAL CARD OF LECTURE Occupation singular occupation Plural occupations Teacher students 1 stage Introduction (5 min.) 2 stage Updating of knowledge (20 min.) 1 . Reports the subject name, the purpose, planned results of lecture and the plan of its carrying out 11.With the purpose to staticize knowledge of students asks focusing questions: 1 . Call Mendel's 3 laws 2 . What you know inheritance types? 3.What is the heterozygote and homozygote? 4 . what is the genotype and a phenotype? Carries out a blitz poll. 2.2 . Displays and offers to examine the lecture purpose. Makes comments on the maintenance of a slide. Slide No. 1 2.3 . Displays a slide No. 2 1 . Listen 2.1 . Answer questions 2.2 . Study the maintenance of a slide No. 1 2.3 . Study the contents 3 stage Informatsion ny (55 min.) 4 stage Final (10 min.) 3.1 . Consistently states a material of lecture on plan questions, uses visual materials and system of focusing questions: On 1 question of the plan: Give definition to gene diseases at children? On the 2nd question of the plan: list the main symptoms of gene diseases On the 3rd question of the plan: what mechanisms underlie development of gene diseases? On the 6th question of the plan: What prevention of gene diseases? Focuses attention on the key moments of a subject, suggests them to write down. 3.1 . Discuss the maintenance of the offered materials, specify, ask questions. Write down the main thing 4.1 . Asks a question: 4.1 . Answer a question 1 . List signs characteristic for gene diseases characteristic for FKU. 2 . Than differs hereditary diseases from not hereditary? 4.2 . Gives a task for independent work: Albinism. 4.2 . Listen, write down Genetic disease - is different in clinical group of diseases caused by mutations in single genes. The number of currently known monogenic hereditary disease of more than 4,000 clinical entities. These diseases occur with a frequency of 1: 500 to 1: 100,000 and less. In one and the same variety of gene mutations occur. It is known that one and the same nosological form may be caused by different mutations. For example, in cystic fibrosis gene mutations described above in 1000, about 300 of which causes the clinical manifestations. In more than 30 phenylalanine hydroxylase gene mutations cause the clinical manifestations of phenylketonuria Each gene can occur up to several tens or even hundreds of mutations that lead to disease. Consequently, it is easy to count how many monogenic diseases might be in humans. Actually mutational change primary protein structure often leads to cell death and the mutation does not occur in hereditary disease. These proteins are called monoformnymi. They provide the basic functions of cells, maintaining stability of the specific organization. Features of inheritance of genetic diseases is determined by the laws of Mendel. Mutations can occur in any of the genes resulting in impaired (changes) the structure of the respective polypeptide chains of the protein molecules. As in the human body according to rough estimates are more than 100,000 different proteins, it becomes clear the extreme diversity of clinical manifestations of monogenic diseases. Depending on the function of the protein will be changed biochemical changes in the body, leading to specific clinical picture of hereditary disease. For example, mutations in genes that control the structure of the protein - collagen, there is a generalized loss of connective tissue. Mutation of the gene that determines the sequence of the amino acid phenylalanine - an enzyme hydrolyzing phenylalanine, there is a disease known as phenylketonuria (PKU). When globin gene mutation develops a picture of severe anemia (hemoglobin disorders). Many mutations lead to the formation of the molecular forms of proteins pathogenic action which is detected only in the interaction of the organism with the specific environmental factors. This is the so-called ekzogenticheskie options. For example, individuals with clinically manifested deficiency of glucose-6-fosfatgidrogenazy (G-6-PDG) erythrocytes horsebean use in food or medicines sulfanilamidnymi oral treatment leads to develop hemolytic crisis (intravascular erythrocytolysis). It should be emphasized that the absence of contact with certain substances in carrier "ekzogeneticheskih" mutant alleles did not occur pathological reactions or disease. Start the pathogenesis of any genetic disease associated with a primary defect of the mutant allele. It can manifest itself in the following ways: lack of protein synthesis, synthesis of an abnormal protein in primary structure; quantify the excess protein synthesis, protein synthesis quantitatively insufficient. The fundamental pathogenesis of genetic diseases can be represented as follows: mutant allele → → pathological primary product of the subsequent chain of biochemical reactions cells → → → body organs. Diseases of metabolic disorders of aminoacids The role of amino acids for the human body and especially to the child's extremely high. It is known that amino acids are the basic structural elements of the protein are used for hormone synthesis, immune bodies serve as a source of energy. Nitrogen metabolism involves the reaction of synthesis and breakdown of proteins, nucleic acids, amino acids and nucleotides, as well as a number of other nitrogen-containing compounds. A common feature of nitrogen metabolism in children - a positive nitrogen balance nitrogen, which is a necessary condition for growth. Nitrogen food as much as possible is used by the body for the growing plastic targets. Disturbances in the metabolism of amino acids may represent a significant threat to the normal functioning of the human body. Genetically determined diseases associated with metabolic disorders of amino acids, deserve special attention. Phenylketonuria (PKU) Phenylpyruvic mental retardation was opened in 1934, Felling. It is an inherited disorder of amino acid metabolism caused by mutations in the gene for phenylalanine hydroxylase, liver enzyme phenylalanine hydroxylation reaction was carried out, ie its conversion into tyrosine. Mutations within this large gene of the human genome affect different parts of it and damage the function of different enzyme. Frequency prevalence of this disease varies from 1: 7000 to 1: 10000 and more people. The disease is common in populations where the spread of kinship marriage. Heterozygotes occur in populations with a frequency from 1: 50 to 1: 1000. The disease is transmitted in an autosomal recessive manner. Pathogenesis. Phenylalanine is an essential amino acid for human growth and development and is found in all protein foods. The pathogenesis of disease is the failure of the liver enzyme phenylalanine hydroxylase, which leads to disruption of the exchange of phenylalanine and increasing by more than 10 times the concentration of toxic products of metabolism disorders - phenylacetic, phenyllactic and phenylpyruvic acids, which have neurotoxic effects. Increasing the concentration of phenylalanine, tyrosine and restricts the transport of tryptophan across the blood-brain barrier. The accumulation of phenylalanine in the brain of the patient and depresses the activity of enzymes involved in the synthesis tserebrozidsulfatov that protects the brain from demyelination. CLINIC. The disease usually manifests in the first few months after birth, delayed mental and motor development. Clinical manifestations are very diverse. Often, these patients are diagnosed as cerebral palsy, mental retardation. Early manifestations of the disease are regurgitation, vomiting, and diarrhea. Neurological symptoms appear later in the form of sleep disturbance, seizures, mental retardation. Develops muscular hypo-or hypertension. Motor development is delayed. Children start with late sitting and walking, there is an odor of sweat and urine -'' mouse'' smell. Of the skin marked decrease or absence of pigmentation, dermatitis, eczema, photosensitivity. Hair and irises also lose pigmentation. Violations of the cranial nerves manifest strabismus, nystagmus, loss of coordination of movement. In later years there is a characteristic posture sick -'' tailor'' posture and gait peculiar. Patients are wide apart, legs bent at the knees and hips, lowering his shoulders and head. When walking, make small steps and swaying. In photos 1 and 2 show the brother and sister of PKU patients. At the time of shooting brother, 16 years old, my sister - 14 years old. Children born of consanguineous marriage (cousin brother - sister). Two other children of the family - are healthy. Both children clinic disease is similar. In patients with profound degree of mental retardation. DIAGNOSIS Mounted on the basis of clinical and biochemical data, molecular genetic studies. Because of the clinical polymorphism of PKU should be excluded from each of the retarded child. Sample Felling is the most affordable and simple. By 2-3 ml of acidified urine was added hydrogen chloride reagent Felling (10% solution of ferric chloride of iron - FeCl3) in an amount of 0.5 - 1 ml. The sample is considered positive when a green coloring. Increasing the concentration of phenylalanine in the plasma and urine can be detected by TLC. When determining phenylalanine in the blood plasma sample is used Guthrie based V.subtil good growth in medium containing a phenylalanine. TREATMENT. Phenylalanine is an essential amino acid and a minimum dietary administration is absolutely necessary. For the treatment of PKU amino acid mixture used or protein hydrolysates with a low content of phenylalanine. This basic diet supplemented with protein-free and low-protein foods, vitamins and trace elements. Limited to products containing a large amount of phenylalanine, including breast milk, and animal milk. Such a diet should be administered no later than 2-3 weeks of age and continue until 5 years of age. At older ages, decreasing the sensitivity of the central nervous system to the damaging effects of phenylalanine and products of metabolism, and the main stages of brain development had already been completed. The need for protein is provided by protein hydrolysates or mixtures of amino acids, such as "Gipofenat'''''' etc. Berlafen After reduction of phenylalanine in the blood to normal gradually administered animal proteins under the control of biochemical studies to a total daily phenylalanine intake should not exceed 25 mg per 1 kg of the child. From the diet excludes meat, fish, liver, kidney, eggs, cheese, products made from wheat and rye flour, cottage cheese, nuts, beans, etc. Milk and potatoes are given content of phenylalanine in limited quantities. PREVENTION. In 1954 he has been proven that a diet low in phenylalanine prevents the development of clinical symptoms in patients who were diagnosed at birth. On this basis, was developed and implemented in the practice of public health is the first program of mass screening (ie, screening) newborns for PKU. After this program, mass screening of newborns for PKU quickly spread around the world, and currently about 10 million newborns are tested for PKU annually. Mass screening for PKU give 7-10 - fold economic benefit compared to their life in homes for the disabled. The object of testing in the current programs of mass screening is newborn capillary blood collected and dried in the form of spots on special paper chromatography. The method of testing - often bacteriological test inhibitory Guthrie, at least - fluorometric method for measuring the concentration of phenylalanine. If the screening test is estimated as> 4 mg% phenylalanine in the newborn blood is taken and re-tested. Mass screening of newborns provides secondary prevention of PKU, as it does not prevent the birth of sick children, and only aims to correct the clinical consequences of genetic disease. Primary prevention is possible using the methods of prenatal diagnosis in families with a sick child. At subsequent pregnancy in a family is taken of the fetus biological material for research chorionic biopsy at 8-10 weeks of pregnancy. Cystinosis (Fanconi syndrome) The hereditary disease associated with metabolic disorders of cystine due to the enzymatic block (biochemical mechanism has not been fully elucidated.) Due to the poor solubility of cystine in biological fluids in the excessive accumulation of it in the cells, it is easily precipitated as crystals, causing various operational disturbances in the internal organs, primarily the kidneys. Frequency - 1 600 000. The disease is inherited in an autosomal recessive manner. CLINIC. The disease manifests itself in the late first or early in the second half of life. In patients with worsening appetite, there are constant thirst, constipation, vomiting after eating and drinking, or non-feeding. Reduced resistance to infections a child. Developing eye disease in the form of conjunctivitis, convergent strabismus. In the cornea and conjunctiva of the degenerative changes are observed due to the deposition of cystine crystals in them. Sometimes expressed photophobia. Later, in patients with increased liver and spleen, there is frequent urination with impaired renal function. One of the typical symptoms of the disease is a progressive growth retardation up to severe forms of dwarfism. Then join rahitopodobnyh changes of the skeletal system. However, many children die before deployed rahitopodobnyh changes from hyperthermia, coma, collapse. In a separate part of the skeletal system of children changes the contrary, it is the main sign of the disease. Children are stunted. They are marked curvature of the long bones, the parietal bumps, deformities of the chest, spine, muscle hypotonia, "beads" on the edges, "rachitic bracelets", etc. Clinical and radiological manifestations of these phenomena are similar to rickets associated with a deficiency of vitamin D. From the disease de Toni-Debre-Fanconi cystinosis different development at an earlier age and more unfavorable course. DIAGNOSIS Established on the basis of characteristic clinical picture, data, laboratory studies: giperaminoatsiduriya, phosphaturia, glycosuria, kaltsiyuriya. Cystine crystals may be found in the cornea with a slit lamp examination. With conjunctival biopsy, kidney or lymph node puncture can establish the presence of crystals in it. TREATMENT Not fully developed. Apply large doses of vitamin D (100 000 IU per day), which prevents the progression of rahitopodobnyh changes in the bones and reduces the aminoaciduria, glucosuria, phosphate and kaltsiyuriyu. Displaying treatment of anabolic hormones. In the fight against acidosis shows the assignment of citrate mixture of 4% solution of soda. Application of the penicillin compound promotes formation of cystine, readily soluble in water. FORECAST usually unfavorable, in 2-3 years from the onset of illness comes death. Tyrosinosis Progression of the disease is due to the lack of парагидроксифенилпировиноградной acid oxidase. In healthy individuals, this enzyme converts the said acid gomogentezinovuyu. In the presence of the enzymatic defect exchange disrupted tyrosine, which leads to the development of tyrosinemia and tirozinurii. In the early pathological process involved the liver, kidney, skeletal system (rahitopodobnyh change). The disease is transmitted in an autosomal recessive manner. CLINIC The disease begins to manifest itself in the first months of life vomiting, retarded physical development, enlargement of the liver. In connection with the development of cirrhosis, jaundice, ascites, bleeding into the skin. As a consequence of renal disease develops glyukoaminofosfat diabetes, which causes changes rahitopodobnyh bone: osteoporosis, osteomalacia, bending bones, etc. In many cases, delayed mental development. Diagnosis is based on clinical symptoms, early signs of hepatic insufficiency, as well as the biochemical examination data (positive sample Millon excretion, increased plasma tyrosine to 10 mg% or more, the presence paragidroksifenil-pyruvic acid in the urine). The absence of the enzyme can be installed in histochemically punctates liver. Differential diagnosis of conduct with the syndrome de Toni-Debre-Fanconi, where there is no significant liver damage and negative samples for biochemical tyrosinosis, with inherited prenatal hepatitis, manifested in contrast to the tyrosinosis already at birth with galactosemia, mainly on the basis of biochemical data . Treatment aims to control phenylalanine and tyrosine in the diet and in many ways is similar to the treatment of PKU. FORECAST unfavorable. In the absence of appropriate treatment children die before the age of 10 years from liver failure Homogentisuria The disease is known for more than 100 years. A urine of patients allocated gomogentenzinovaya acid, which is absent in normal. In liver and kidneys of patients no enzyme gomogentenzinovoy acid oxidase, which results in an accumulation and enhanced urinary excretion. The frequency of the disease - 1:1,000,000 population. The disease is inherited in an autosomal recessive way. Pathogenetic mechanism of the disease is not fully understood. CLINIC. The disease is clinically 3 symptoms: dark urine, pigmentation of cartilage and connective tissue, arthropathy. Urine having at normal urination numbers, for 12-24 hours in air darkens. In connection with this disease is detected too late, although there is a birth. In infant colored urine found in the diapers. It is more often from dark pink to red. As a child, this symptom is the only manifestation of the disease. Blue-gray pigmentation (ochronosis) appears after 20-30 years of age. Differential diagnosis of conduct with the syndrome de Toni-Debre-Fanconi, where there is no significant liver damage and negative samples for biochemical tyrosinosis, with inherited prenatal hepatitis, manifested in contrast to the tyrosinosis already at birth with galactosemia, mainly on the basis of biochemical data . Treatment aims to control phenylalanine and tyrosine in the diet and in many ways is similar to the treatment of PKU. FORECAST unfavorable. In the absence of appropriate treatment children die before the age of 10 years from liver failure Homogentisuria (alkaptonyria) The disease is known for more than 100 years. A urine of patients allocated gomogentenzin acid, which is absent in normal. In liver and kidneys of patients no enzyme gomogentenzin acid oxidase, which results in an accumulation and enhanced urinary excretion. The frequency of the disease - 1:1,000,000 population. The disease is inherited in an autosomal recessive way. Pathogenetic mechanism of the disease is not fully understood. CLINIC. The disease is clinically 3 symptoms: dark urine, pigmentation of cartilage and connective tissue, arthropathy. Urine having at normal urination numbers, for 12-24 hours in air darkens. In connection with this disease is detected too late, although there is a birth. In infant colored urine found in the diapers. It is more often from dark pink to red. As a child, this symptom is the only manifestation of the disease. Blue-gray pigmentation (ochronosis) appears after 20-30 years of age. Most often it happens in the ear and the sclera, sometimes on the nose, back, neck and arms. After 30-40 years of joint symptoms occur, determine the severity of the disease. Developing ankylosing "rheumatism", which affects the spine often, less often large joints. It is manifested paroxysmal pain and leads to disability. X-ray examination detects changes in the intervertebral discs, osteophytes and calcification. The disease does not shorten life expectancy. The diagnosis is established when an gomogentenzinovoy acid in the urine. Her blackening by adding a solution NaS03 quite specific to the disease. A reliable diagnosis is made after chromatographic urine. The differential diagnosis spend with porphyria, Argyros, melanoma. Treatment mainly symptomatic. Histidinemia Histidinemia refers to the exchange of hereditary disorders caused by the absence of histidine or insufficient activity of an enzyme gistidazy. The incidence rate is similar to PKU (1: 7000, 1: 10000). The disease is inherited in different ways depending on the genetic variants of the disease. The result is an accumulation of metabolic blocking blood histidine and its derivatives, and reducing the concentration of urocanic, glutamic acid and other acids. CLINIC. For children in the first year of life is an essential amino acid histidine. With a lack of histidine cited poor weight gain, the manifestations of skin exfoliation, eczematous rashes, etc. With a lack of histidine in adult erythropoiesis violation of manifestations, negative nitrogen balance, decreased serum albumin, anorexia, peeling and dry skin, fatigue, erythematous rash and other symptoms of anemia with erythropoiesis violation explains the reduction in the formation of hemoglobin, which includes a large number of histidine. For patients with histidinemia typical blond hair and blue eyes. The clinical picture in the foreground of the nervous system in the form of reduced intelligence, impaired speech, seizures, hydrocephalus is sometimes found, hypo-or hypertonic muscles, cerebellar ataxia. In some cases histidinemia combined with iron deficiency anemia, kidney disease, bone, etc. DIAGNOSIS. Unfortunately diagnosis is only large, well-equipped laboratories, as requires the application of modern biochemical techniques. For patients with a high concentration of histidine in the biological fluids. Histidine excretion by the kidneys is increased. There was an increase of histidine in the cerebrospinal fluid. In connection with the possibility for histidine catabolism main path compensatory increases its conversion to other metabolites. The result is increased excretion imidazolpirovinogradnoy, imidazole-lactic acid and imidazoluksusnoy that is a hallmark of the disease. These acids like phenylpyruvic acid react with a reagent Felling, but the reaction is strongly positive. An important specific feature of the disease is the absence of the main metabolite pathway of histidine (urocanic, glutamic acid, etc.). Confirms the diagnosis of a direct determination of the activity gistidazy in the horny layer of the skin and liver. An important feature of the disease is an abnormal response to an oral load of histidine. After the load level rises histidine even greater extent and reaches up to 300-400 mg / l in 1-3 hours (N - 2 to 25 mg / l) and returns to the original level is not earlier than 5 hours. In healthy after histidine load level reaches the specified value and returns to normal after 3-4 hours. Differentiate histidinemia to PKU. Treatment consists in assigning low-protein diet with a reduced content of histidine. Prognosis of the disease depends on the genetic variants of the disease. Homocystinuria Disease is based on the absence or inactivation of the enzyme tsistationinsintetazy that causes a violation of the exchange of methionine. Patients found to increase blood concentrations of methionine and homocysteine (not in the norm) and a decrease of cystine, the appearance in the urine of homocysteine and cysteine. The disease is inherited in an autosomal recessive way. The disease manifests itself marfanopodobnymi syndromes. Symptom-complex of homocystinuria: 1) The skeletal anomalies: the disparity physique as shortening the torso, limb lengthening, chonechondrosternon, incorrect posture, "winged" scapula, "tower" skull, malocclusion of the teeth and growth, high palate, valgus deformity of the knee, limiting the mobility of the joints, flat feet, osteoporosis, susceptibility to fractures; 2) changes in the nervous system: loss of intelligence, it is depleted, dizlaliya, spastic gait, episyndrome; 3) breach of view lens subluxation, secondary glaucoma, changes in the fundus; 4) of the cardiovascular system: a violation of metabolic processes in the myocardium, the tendency to arterial and venous thrombosis; 5) The external features: light, soft, large curls curly hair, blue iris. Homocystinuria genetically heterogeneous. In addition to classical, there are still two forms: a deficiency of vitamin B6 and folic acid metabolic disorders. Diagnosis is based on the determination of cystine and methionine in serum and urine tsistationinsintetazy determining activity in the liver. Differential diagnosis of the disease should be done with Marfan (violation of connective tissue metabolism). For more Marfan's disease is characterized by: 1) The mitral and aortic valves; 2) muscular dystrophy; 3) intelligence is not always reduced, episyndrome missing. Treatment consists in the appointment of a diet enriched with cystine and methionine lacking. The effect of treatment depends upon the destination therapy. We also obtain satisfactory results from treatment with pyridoxine, which stimulates other pathways serosoderzheschih amino acids. The therapeutic effect of vitamin B6 is associated with increased activity tsistationin sintetazy. Disorders of carbohydrate metabolism disorders Carbohydrate ingested in the form of monosaccharides (glucose, fructose), disaccharides (lactose, maltose, sucrose), and polysaccharides (glycogen, starch). During the first months of life is a major carbohydrate food disaccharide lactose or milk sugar comprising glucose and galactose. Lactose content of human milk is an average of 70 g / l, bovine - 48 g / l. The centerpiece of the carbohydrate metabolism is glucose. Disaccharides and polysaccharides are digested in the gastrointestinal tract to monosaccharides. Galactose is converted to glucose in the liver and erythrocytes. Of key importance in this process is an enzyme galactose -1 - phosphate uridiltransferaza. Galactosemia Galactosemia refers to a group of abnormalities of carbohydrate metabolism, characterized by lesions of the central nervous system, muscular system, liver problems, abnormal red blood cells, hypoglycemic state. A typical variant of galactosemia inherited as an autosomal recessive. The incidence is approximately 1: 30 000 live births, but according to different authors, it ranges from 1:8000 to 1: 187,000 population. The basis of the primary biochemical defect is galactosemia enzyme deficiency of galactose1-fosfaturidiltransferazy (HA-1-BOP), resulting in the tissues of the body accumulates excess galactose-1-phosphate and other products of incomplete decomposition of lactose causing clinical manifestations galactosemia. In classic galactosemia type are still two possibilities: Duarte form of a 50% enzyme activity and Negro type in which the enzyme activity is reduced only in certain cells (red cells, fibroblasts). CLINIC Can be of varying severity. Most mild cases are found in families where there are patients with galactosemia. These children early refuse the breast and can not tolerate milk. In the most severe clinical signs are detected in the first days after birth. Body weight at birth, usually contained large (over 4 kg). In patients after breast-feeding is plentiful and there is persistent vomiting, diarrhea, weight loss, jaundice, hepatomegaly increases, there bleeding and hemorrhages in the skin. Often marked hypoglycemia, seizures, cataracts appear in the future, the signs of cirrhosis of the liver, and the lag in the neuro-psychological and physical development. DIAGNOSIS. The large number of phenocopies and complexity of biochemical methods of diagnosis of galactosemia explain the fact that the disease is not always recognized in a timely manner. Often children with galactosemia come to the clinic with a diagnosis of sepsis, biliary cirrhosis, acute indigestion, prolonged neonatal jaundice etc. A number of diseases of the newborn period has similarities with the clinical manifestations of galactosemia, hemolytic disease of the newborn, congenital hepatitis, biliary atresia, cytomegalovirus, toxoplasmosis congenital, hereditary hyperbilirubinemia (such as Crigler Najjar), etc. The need for difdiagnostiki can occur when a prolonged jaundice and preterm infants. Establishing an accurate diagnosis of galactosemia requires complex diagnostic procedures. Detection of galactose in the urine of a newborn child is the basis for his diligence for galactosemia. The most reliable diagnostic methods include determining the concentration of blood galactose by chromatography paper, direct determination of the activity of the enzyme galactose-1-phosphate - uridiltransferazy (HA-1-BOP) in erythrocytes and galactose determination in urine. In addition to the diagnosis may help correct the assembled family history. TREATMENT. From the first days of life, the child should be transferred to a dairy-free diet. As milk substitutes can be used a mixture prepared by almond and soy milk. Dextrinosis Under this general title brings together a group of diseases for which the characteristic accumulation of glycogen in tissues and organs associated with the violation of the activity of an enzyme involved in the metabolism of glycogen. Disease are inherited in an autosomal recessive way. Frequency of glycogen storage of all types of 1: 40,000 people. The most well-described 6 types of glycogen storage disease, although they are at much greater. CLINIC. Common clinical symptoms are: onset in childhood, symptoms of hypoglycemia (vomiting, convulsions, loss of consciousness, coma). Glycogen is the most intensively accumulated in those organs in which it is synthesized, ie in the liver, kidney and muscle. Depending on which organ is most involved in the pathological process, distinguish three main forms of the disease: 1. Hepatic form 2. Muscular form 3. Generalized form Hepatic form The symptoms usually appear during the first year of life, although the child's development in this period is going well or somewhat slower. Starting with 8-9 months of life, 1 every 2 months or more frequent episodes of hypoglycemia (loss of consciousness, clonic spasms of limbs). Seizures begin before a meal or early in the morning, their appearance can be prevented reception of sweet water. Appearance of patients: small stature, big belly, disproportionately thin limbs, "doll face." The liver is enlarged. The most difficult disease occurs between the ages of 4-5 years. Intercurrent disease heavier during the main pathological process. With age, the condition of patients can be improved, which can be explained by the development of compensatory mechanisms for the exchange. Intelligence is usually not disturbed. Muscular form The main symptoms of this form of the disease occur from 7 - 10 years. Patients become inactive, tired quickly during physical exertion. In the future, muscle weakness progresses. Aching muscles after intensive prolonged exercise, there is tachycardia, shortness of breath. These symptoms generally appear for 25-35 years. Appearance patients usually does not change. The boundaries of the heart usually expand. Of the liver and kidney marked changes do not happen. Prognosis mostly favorable, although known deaths in the age of 25-30 years. Generalized form This form of glycogen storage disease characterized by the fact that in almost all organs and tissues of the patient collects a significant amount of glycogen. The clinical picture of this form is not like the picture of the liver and muscle forms. This form includes biochemical types of glycogen storage disease type III and IY (diseases and Corey Anderson). Biochemical types of glycogen storage disease: 1.Bolezn Gierke (I type) - deficiency of the enzyme glucose-6-phosphatase. 2.Bolezn Pompe (II type) - deficiency of the enzyme acid glucosidase. 3.Bolezn Corey (W type) - deficiency of the enzyme 1,6-glucosidase. 4.Bolezn Andersen (IY type) - branching enzyme deficiency. 5.Bolezn McArdl (Y type) - deficiency of the enzyme phosphorylase muscles. 6.Bolezn Hers (YI type) - deficiency of the enzyme phosphorylase liver. DISEASE Gierke (I type) Clinical illness caused by the absence of a specific enzyme activity of glucose-6-phosphatase activity in the intestinal mucosa and liver, and in some cases and in the kidneys. The clinical picture of the disease mainly causes the metabolism of glycogen in the liver. Clinical disease is very similar to the shape of the hepatic disease, which has been described above. In the neonatal period are the cardinal symptoms of hypoglycemic seizures, and hepatomegaly. Stunting starts celebrated from the 1st year of life. Characterized by the appearance of patients: big head, "doll face", a short neck, a big belly. A feature of this type of glycogen storage disease is that in children aged 5-7 years are hemorrhagic rash, and frequent nosebleeds. In 10% of cases there is xanthelasmatosis. The disease is inherited in an autosomal recessive manner. Pompe disease (II type) The disease caused by the absence of the enzyme - acidic alpha - glucosidase or gamma amylase in liver and muscle, which leads to destructive changes in tissue and primarily intensive muscle such as the heart muscle. The disease usually manifests itself in the first year of life as a complex sipmtomo heart failure. Shortly after the birth of a child develops anxiety, there is increasing cyanosis, respiratory distress. On examination found "globular" heart, hepatomegaly, mild muscle hypertrophy, macroglossia. Unlike glycogenosis type I not marked hypoglycemia and acidosis. Sick children are killed at 1 year of age. In the mild form of Pompe disease is absent activity of alpha-glucosidase only in the muscles. In these cases, the disease usually appears later in life and on the clinical picture is similar to the myopathy. The prognosis of this form is different, possibly fatal. Treatment of glycogen storage is not enough developed. The use of adrenaline, hydrocortisone able to increase the rate of sugar in the blood due to the breakdown of glycogen was ineffective. Some authors recommend the use of small doses of glucagon and tireoidina. The importance placed on diet, which is an increase in carbohydrate intake of patients and in quickening the meal. FRUKTOZEMIYA The cause of the disease is a deficiency of the enzyme fructose - I-mono-phosphate aldolase in the liver, kidneys, mucous membrane, as well as decreased activity of fructose-1 ,6difosfataldolazy. Changes in any of the enzyme affects the other. Deficiency of these enzymes leads to the accumulation of blood and tissue fructose and fructose-I-phosphate, having a toxic effect, and determining the disease symptoms. The most severe pathological changes occur in the liver: cirrhosis, steatosis, necrosis of the cells. The frequency of the disease-1:130000 population. The disease is inherited in an autosomal recessive manner. CLINIC. The disease manifests itself in a period when infants give fruit juices, sugar or early transfer of children to mixed and artificial feeding. In children, there is persistent anorexia, vomiting, malnutrition, hepatomegaly and jaundice have been observed in severe disease. In benign form of early childhood observed only gastro-intestinal disorders and difficulty in feeding. Children refuse foods containing glucose. With age, the patients begin easier to carry small amounts of foods containing fructose. By increasing the amount of fructose in the diet of patients with the condition worsens because of hypoglycemia and giperfruktozemii. Disorders of lipid metabolism disorders The role of lipids in the life of the human large. It is known that at different stages of ontogeny lipid metabolism has its own characteristics. In young children for normal processes of growth and development is very strong demand for plastic materials and energy. Thus, the younger organism, the above need. In this regard, important in lipid metabolism belongs quality food composition. One of the features of the body of the young child is prone to ketosis, ie tissue accumulation of ketone bodies. Lipid disorders are a frequent companion of pathological processes in children. In its genesis, they can be divided into 2 groups: Hereditary and acquired diseases. Hereditary defects in lipid metabolism are divided into 2 groups: 1). Lipidoses or sfingolipidozy - diseases violation katobolizma structural lipids, leading to accumulation of sphingolipids in the cells of various tissues; 2). Diseases caused by metabolic disorders of lipids contained in the blood. Allocate about 10 sfingolipidozov for which clarified the biochemical defect. Most of these forms have a similar clinical picture due to violation of katobolizma different but structurally related sphingolipids. The clinical picture is characterized by progressive dementia, movement disorders, bone disease, internal organs (liver, spleen, kidney), skin and eyes. The value of lipoproteins in the body is to transport and allocation of organs cholesterol and triglycerides. Lipoprotein metabolism is not only controlled by genetic factors, but also depends largely on the nature of the food. Therefore, disorders of lipid metabolism of blood plasma are a complex group of states, of which only in recent years have been due to isolate monogenic forms. Hyperlipidemia is an important factor in the development of atherosclerosis and coronary heart disease. For most forms of hyperlipidemia is characterized previously (aged 15-20 years) development of the atherosclerotic process with the clinical picture of angina pectoris, myocardial infarction, xanthelasmatosis. Most hyperlipidemia is inherited in an autosomal recessive manner. Clinical symptoms and biochemical changes characteristic of hyperlipidemia, highly variable and may be changed under the influence of a change of diet and other factors. Therefore, the diagnosis can be made on the basis of the whole complex of clinical symptoms, the history and laboratory findings. Inherited disorders of lipid metabolism have attracted the attention of researchers in that they cause the development of atherosclerosis and other forms of cardiovascular disease. According to statistics, coronary heart disease (CHD) is one of the first places in the structure of morbidity and mortality. A clear relationship between hyperlipidemia and increased risk of coronary heart disease has been repeatedly confirmed by various researchers. The degree of risk is determined based on the level of cholesterol in blood. The incidence of this disease in the population is quite high - from 7 to 28%. Amavrotiches idiocy ( Tay - Sachs disease) Amavrotiches idiocy Tay - Sachs disease occurs predominantly among Ashkenazi Jews. The incidence is 1: 6000 among Ashkenazi Jews and 1: 500,000, among other nationalities. The frequency of heterozygous carriers of the recessive gene among Ashkenazi Jews is 1: 40, among other nationalities - 1: 380. Heterozygous carriers of the abnormal gene reduced the activity of the enzyme hexosaminidase A and the contents of sphingomyelin and kephaline in red blood cells. The disease is inherited in an autosomal recessive manner. CLINIC. The disease begins to manifest itself in the age of 4-6 months. A child who was previously active, and gradually loses interest in the outside world, no longer laugh, to play, to learn the parents. Sooner found decreased vision. The child can not stare. In the fundus revealed a symptom of "cherry pit." In the subsequent atrophy of the optic nerve and blindness. In children, there is a decrease of intelligence to the level of idiocy. Movement disorders lead to total immobility. Children startled by the sharp sound may experience seizures. In the final stage of the disease develop cachexia and the state of decerebrate rigidity. Death occurs within an average of 1.5 - 2 years after the onset of the disease. DIAGNOSIS. In the blood plasma of patients with elevated cholesterol levels, and reduced the number of glycolipids. In patients erythrocytes also increases cholesterol and the amount of phospholipids is reduced. Patients glutaminschavelevouksusnoy transaminase enzyme activity increased 3-4 times the activity of the enzyme fructose-I-phosphate aldolase reduced. Niemann-Pick disease/ This form sfingolipidoza is a relatively frequent and severe lipidosis, which occurs in 50% of cases among Ashkenazi Jews. The disease is associated with a congenital deficiency of an enzyme sfingomielinidazy. Enzyme unit leads to the accumulation of sphingomyelin in tissues. When this sphingomyelin and cholesterol accumulates in almost all organs and tissues from a primary lesion of the CNS, spleen, liver, bone marrow, lung, etc. The disease is inherited in an autosomal recessive manner. CLINIC. The disease begins to manifest itself in the first months after the birth of dyspeptic disorders, deterioration of general condition, copious sweat, weight loss, frequent pulmonary complications. The disease is characterized by brownish or greyish-yellowish pigmentation of the skin and mucous membranes. On the tongue and gums are often observed inky blue spots. Syndrome is the leading hepatosplenomegaly. Often marked by generalized lymphadenopathy, osteoporosis. Neurological syndrome characterized by muscular hypertension and disappearance of physical activity. Mental degradation occurs gradually, reaching a total idiot. In the fundus there is a bright red spot, characteristic amavroticheskoy idiocy Tay-Sachs disease. Hearing gradually weakened to a full hearing. The disease progresses continuously and ends in death within a few years. Diagnosis is based on clinical presentation and on the detection of decreased activity of the enzyme sfingomielinidazy punctates in the liver and kidneys. Gaucher disease Clinical picture. Known 3 clinical forms of the disease, different start time and the prevalence of a symptom. With early dominated by neurological disorders. From birth, a marked malnutrition, bulbar disorders, soundless scream (Athos), impaired swallowing (dysphagia), lockjaw, sagging of the lower jaw. Death occurs from aspiration of food masses, pneumonia. In older children and adults, the clinical picture is dominated by an enlarged spleen, hemorrhagic syndrome, anemia. Moderately enlarged liver. Bone changes are manifested as pain, deformities, pathologic fractures. There are muscle rigidity, incoordination, convulsions. The disease progresses slowly. In the terminal stages of severe neurological symptoms appear. Survival to 20-30 years of age and die of cachexia, hemorrhage. Inheritance - autosomal recessive. Diagnosis is based on clinical presentation, detection of metabolic defect caused by the lack of the enzyme glucosidase. Recommended reading: 1. NP Bochkov, AF Zakharov, VI Ivanov, "Medical Genetics", M - 1984 2. KN Nishonboev, F.A-Khamrayeva, O.E-Eshonkulov "TIBBIYOT genetikasi" Tashkent 2000 3. NP Bochkov, "Clinical Genetics", M - 1997 4. SI Kozlov et al, "Hereditary syndromes and medical genetic counseling ', M - 1987 5. RM Cohn, KS Roth, "Early diagnosis of metabolic diseases," M 19971. 6. VN Gorbunov, V. Baranov, "Introduction to molecular diagnostics and gene therapy of inherited diseases", St. Petersburg, 1997