Survey
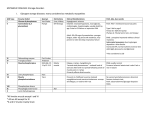
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
PEDIATRIC GRAY MATTER DISEASES Degenerative neurological diseases presenting in the 1st six years of life A whirlwind tour of eponyms and other hard-to-remember minutiae Steven Leber, M.D., Ph.D. January 7, 2016 Developmental level Normal Delayed Regression Age HOW DO WE CLASSIFY NEUROMETABOLIC DISORDERS? • • • • • • • • • • • Disorders of lipid metabolism Disorders of carbohydrate metabolism Disorders of urea cycle enzymes Disorders of amino acid metabolism Disorders of organic acids Mucopolysaccharidoses Mucolipidoses Disorders of trace metal metabolism Disorders of purine & pyrimidine metabolism Mitochondrial disorders Peroxisomal disorders “GRAY MATTER” vs “WHITE MATTER” Gray White Early seizures Common Uncommon EEG Sharp Slow Dementia Early Variable Motor deficit Variable early; later severe Prominent early Visual deficit Early; usually Later; optic nerve or retinal; abnormal usually tract; ERG abnormal VER CLASSIFICATION • Infantile vs late infantile • With or without visceral storage INFANTILE, WITHOUT VISCERAL STORAGE • • • • • • • • • • • Tay-Sachs Alper Menke Rett Farber Pompe Leigh Infantile neuroaxonal dystrophy "Cerebral" GM1 gangliosidosis (type II) Infantile neuronal ceroid lipofuscinosis (NCL, CLF) Congenital disorder of glycosylation type Ia INFANTILE, WITH VISCERAL STORAGE • • • • • • Generalized GM1 gangliosidosis Gaucher's (infantile) Niemann Pick, type A Sandhoff Wolman Glycolipid and glycoprotein disorders(fucosidosis, mannosidosis, sialidosis, I-cell disease) LATE INFANTILE, WITHOUT VISCERAL STORAGE • • • • • Neuronal ceroid lipofuscinosis Juvenile Tay-Sachs Progressive myoclonus epilepsies Huntington disease Xeroderma pigmentosa LATE INFANTILE, WITH VISCERAL STORAGE • Gaucher Type III • Niemann Pick, type C • Mucopolysaccharidoses – Hurler's – Hunter's – Sanfilippo's INFANTILE, WITHOUT VISCERAL STORAGE • • • • • • • • • • • Tay-Sachs Alper Menke Rett Farber Pompe Leigh Infantile neuroaxonal dystrophy "Cerebral" GM1 gangliosidosis (type II) Infantile neuronal ceroid lipofuscinosis (NCL, CLF) Congenital disorder of glycosylation type Ia TAY-SACHS DISEASE (GM2 GANGLIOSIDOSIS) • Onset: 0-6 months, usually 1-3 • Early myoclonus (startle, without habituation, especially to noise [hyperacusis]) and irritability • Seizures in first six months (infantile spasms, gelastic or other partial, generalized). • Dementing • Hypotonic at first; progressively weak; later spastic • Macrocephaly usually begins at ~ 18 months (brain weight often > 2000 gm) • Progressive; most die in 2nd or 3rd year • Milder forms exist TAY-SACHS DISEASE • Cherry-red spot – Usually seen within first few months – Accumulation of storage material, with degeneration of parafoveal ganglion cells – Choroid visible and appears red and is surrounded by gray ring – Not specific for TS • Blindness by 1 year • Normal pupillary reaction and ERG; VER abnormal TAY-SACHS DISEASE - Genetics • Not only Ashkenazi Jews • Carrier frequency – Ashkenazi Jews: 1 in 30 • Those from small area near Lithuania: 1 in 19 • Prior to screening, 1 in 2500-3600 Ashkenazi Jews were affected; screening has ↓’d by >90% – Non-Jews 1 in 300 • Pockets of higher incidence – – – – Western China French Quebec Pennsylvania Dutch Louisiana Cajun Ceramide GANGLIOSIDE NOMENCLATURE • G: ganglioside • M: how many sialic acids – A 0, M 1, D2, T3 • Number: position on band – Smaller (few hexoses) migrate faster • 4 sugars: 1 (e.g., GM1) • 3 sugars: 2 • 2 sugars: 3 TAY-SACHS DISEASE • Hexosamindase A = α β • Hexosamindase B = β2 • Tay-Sachs: α-subunit mutation – Chromosome 15 – Hexosaminidase A deficiency • Cannot breakdown GM2 ganglioside • Accumulates in lysosomes • Sandhoff's: β-subunit mutation – – – – Hexosaminidase A & B Like Tay-Sachs but with visceromegaly Rarer than Tay-Sachs Death usually by age 4 TAY-SACHS DISEASE - Pathology • Ballooned cells with swollen axons (torpedoes) and membranous cytoplasmic bodies • If survive long enough, often cystic white matter changes ALPER (progressive infantile poliodystrophy) • Controversial and difficult to define • Triad of progressive: – Refractory epilepsy – Dementia – Liver failure • Familial in some • Onset in neonatal period to 1st few years • Arrested head growth microcephaly • Vegetative after 1-3 years ALPER • Severe cortical neuronal degeneration (especially layers III and IV) • No visceral or brain storage • Liver cirrhosis in some • Pathologic diagnosis, plus one of exclusion and family hx • Can be caused by mutation in the nuclear gene encoding mitochondrial DNA polymerase gamma (POLG), leading to mitochondrial DNA depletion • Risk of valproate-induced hepatic failure! MENKE • X-linked recessive – Xq13 • • • • • Onset: 1st weeks to months Prominent seizures and myoclonus at onset Severe dementia and regression Hypotonic with brisk DTRs Hypothermia, hypoglycemia, and prematurity common MENKE • Hair – “short, sparse, coarse, and twisted” – kinky, coarse, unpigmented – Pili torti: twisted shafts – Trichorexis nodosa: fragmentation – Monilethrix: periodic narrowing MENKE • Copper and ceruloplasmin both low – in brain and liver (high in intestine, kidney, and fibroblasts) – Intestinal malabsorption – Cu++ and ceruloplasmin may be nl 1st few weeks of life • Menkes gene (MNK) product copper-transporting ATPase • Copper-dependent enzymes (e.g., cytochrome-coxidase, dopamine ß-hydoxylase) malfunction – Parenteral copper injections help survival and neurologic symptoms in pts with certain mutations if treatment started in the neonatal period MENKE • Vasculopathy; tortuous cerebral vessels • Pathological fx’s • Pathology – Diffuse atrophy plus focal infarctions – Subacute inflammatory meningoencephalitis – Hemorrhages common (ddx – abuse) RETT SYNDROME • Almost exclusively girls • Common; one of most common genetic causes of mental retardation in girls • Incidence in US: up to 1 in 10,000 female births RETT SYNDROME: 4 clinical stages • Normal at birth • I. At 6-18 months: Developmental arrest – – – – Development slows and then arrests Possible decrease in eye contact and communication Diminished interest in play Head growth decelerates • Acquired microcephaly – Seizures not common but can occur RETT SYNDROME: 4 clinical stages • II. 1-4 years (usually 2nd year): rapid regression – Phase lasts days to months – Dramatic deterioration; can appear encephalitic or toxic • Loss of language skills • Autistic behavior • Decreased purposeful use of hands • Stereotyped hand-wringing, slapping, or hand-to mouth movements RETT SYNDROME: 4 clinical stages • Stage II, continued: – – – – – – – – – Ataxia of trunk and extremities Gait apraxia Seizures (GTC, complex partial, atypical absence) Apnea, then hyperventilation, only during wakefulness Episodes of jerky movements Insomnia and sleep disturbance Self-abusive behavior Bruxism, aerophagia GI problems (constipation, GER, poor growth) RETT SYNDROME: 4 clinical stages • III. 2-10 years of age: pseudostationary – Lasts months to years – Apparent stabilization – Autistic behavior less prominent, improved personality, eye contact – Increased rigidity, bruxism – Continued seizures and gait ataxia/apraxia – Continued sleep problems – Poor weight gain – Prolonged QT RETT SYNDROME: 4 clinical stages • IV. Teenage years: late motor deterioration – – – – – – – – Slow deterioration Ambulation lost Spasticity plus LMN signs Dystonia, parkinsonian features may occur Scoliosis, foot deformities Reduced seizure frequency Improved eye contact Most survive to 5th or 6th decade RETT SYNDROME - Etiology • Pathology: Moderate neuronal loss and cortical/dendritic atrophy • Despite developmental regression, not felt to be degenerative • Gene MeCP2 identified in 1999 – Methyl-CpG binding protein-2 – Affects regulation of other genes (“expression silencer”) – MeCP2 protein binds to methylated DNA, activating histone deacetylase – Mutations allow gene to be inappropriately turned on • Testing is now 96% sensitive (CDKL5, FOXG1 in ddx) RETT SYNDROME - Genetics • Phenotypic severity correlates with proportion nl vs mutant X-chromosome inactivated • Spontaneous mutations 99%, familial 1% • Spontaneous mutations almost always occur in sperm • Boys: familial cases or in-ova mutations RETT SYNDROME- Variants • Females – Classic – Preserved speech variant (Zappella variant) – Early seizure variant (Hanefeld variant) – Mental retardation and seizures – Pure autism – Angelman-like – Mild mental retardation • Boys – Severe neonatal encephalopathy; usually die in 1st year – Mild MR, seizure, ataxia – Bipolar or schizophrenic • Whom to test???? – Tremor seems to be prominent in most FARBER LIPOGRANULOMATOSIS • Extremely rare • Presents soon after birth with hoarse cry, respiratory distress, hyperesthesia over joints • Then painful joint swellings and rigidity, subcutaneous nodules, especially around tendons and joints FARBER LIPOGRANULOMATOSIS • • • • Hypotonia Usually dementing, but some normal No seizures ↓ acid ceramidase ceramide with anterior horn cell storage • May have cherry-red spots POMPE DISEASE (glycogen storage type II disease; acid maltase deficiency) • Onset at several weeks to several months of age • Involves brain and muscle • Presents with profound hypotonia & weakness, little spontaneous movement (resembles SMA) • Later develop dementia POMPE DISEASE • Massive cardiomegaly • Liver firm but usually not enlarged unless CHF • Usually die by 1-2 years of age • Acid maltase deficiency glycogen storage POMPE DISEASE • Treatment with alglucosidase alfa approved by FDA in 2006 • Early treatment (compared to an untreated historical control group) – Reduced the risk of death by 99% – Reduced the risk of death or any type of ventilation by 88% – Significantly improved motor and cognitive development • Basis of movie Extraordinary Measures • Cost: $60-400,000 per year LEIGH SYNDROME (subacute necrotizing encephalomyelopathy) • Onset in early infancy (60% in 1st year) or childhood; rarely in adulthood • Neonatal form – Acidosis – Severe retardation – Usually early death • Other types with variable clinical picture: – Steadily progressive, saltatory, or episodic – May progress with intercurrent infections – Typically associated with lactic acidosis LEIGH – Symptoms and signs • • • • • • • Retarded motor and intellectual development Respiratory disturbances Ophthalmoplegia Dysphagia and weight loss Vomiting Hypotonia & weakness Ataxia LEIGH – Symptoms and signs • • • • • • Seizures Visual loss Nystagmus Dystonia Peripheral neuropathy (often subclinical) Fevers LEIGH - Pathology • Brainstem and basal ganglia lesions common • Necrosis around 4th ventricle and aqueduct. • Distribution resembles Wernicke's without mammilary bodies and without hemorrhage Figure 1. Sequential FLAIR (fluid-attenuated inversion recovery) MR images of the brain Goldenberg, P. C. et al. Neurology 2003;60:865-868 LEIGH - Multiple specific causes • Generally defects in energy metabolism • Lactate elevated in most patients in some phase of illness, CSF > blood LEIGH - Genetics • Usually due to nuclear gene mutation (autosomal recessive) • Minority due to mitochondrial DNA abnormality (maternal) INFANTILE NEUROAXONAL DYSTROPHY (INAD) • Onset age 6 months-3 years (classic form) • Slowly progressive • Combination of lower, then upper motoneuron signs: – Falling, clumsiness – Hypotonia, hyporeflexia with normal NCV's – Later, spasticity INFANTILE NEUROAXONAL DYSTROPHY • Also later – Optic atrophy, blindness – Involuntary movements, dystonia, decerebrate rigidity – Dementia – Seizures occur in a minority of pts • NCV's normal; EMG's suggest denervation • Autosomal recessive INFANTILE NEUROAXONAL DYSTROPHY • Iron in globus pallidus in 40-50% • Cerebellar atrophy INFANTILE NEUROAXONAL DYSTROPHY • Pathology – Axonal spheroids in medulla (cuneate, gracilis), pons, thalamus, and peripheral nerve INFANTILE NEUROAXONAL DYSTROPHY • Optic atrophy and MRI are helpful in suspecting diagnosis • Resembles PKAN (pantothenate kinase-associated neurodegeneration; Hallervorden-Spatz) but no “eye of the tiger” sign • Diagnosis in the past: skin or conjunctival biopsy; spheroids in nerves • PLA2G6 mutations found in 95% of patients (gene found 2006) – Calcium-independent phospholipase A2, catalyzing the hydrolysis of glycerophospholipids, probably causing membrane pathology "CEREBRAL" GM1 GANGLIOSIDOSIS (TYPE II) • • • • • Normal until 6-14 months, then regress Hyperacusis, ataxia, dysarthria, strabismus Then mental regression, spasticity, and seizures No organomegaly or macular degeneration ß-galactosidase deficiency INFANTILE NEURONAL CEROID LIPOFUSCINOSIS (Santavuori-Haltia) • • • • • • Onset 2nd year of life; occasionally by 8 months Rapid deterioration (weeks to months) Myoclonus Visual loss; retinal degeneration; blind by age 2-3 Dementia Loss of motor skills INFANTILE NEURONAL CEROID LIPOFUSCINOSIS • • • • Acquired microcephaly and severe cerebral atrophy Vegetative state, with death usually by 5-10 years Seizures occur, but not prominent Leukocytes, skin, conjunctiva, rectum: granular inclusions CASE INFANTILE, WITH VISCERAL STORAGE • • • • • • Generalized GM1 gangliosidosis Gaucher's (infantile) Niemann Pick, type A Sandhoff Wolman's Glycolipid and glycoprotein disorders (fucosidosis, mannosidosis, sialidosis, I-cell disease) GENERALIZED GM1 GANGLIOSIDOSIS (TYPE I) • Feeding difficulty plus failure to thrive noted soon after birth • Poorly responsive • Hypoactive • Hypotonic • Hyperacusis • Cherry-red spot in about half GENERALIZED GM1 GANGLIOSIDOSIS (TYPE I) • Edema of face and extremities • Bone changes – Long bones wide in center, tapered at end – Vertebral hypoplasia and beaking • Hepatosplenomegaly • Corneas clear • Store ganglioside in brain and mucopolysaccharide in viscera and bone • ß-galactosidase deficiency • Usually die in first 1-2 years GAUCHER DISEASE (TYPE II; Acute Neuronopathic) • • • • • Rapid (1-3 year) course Onset usually by 3-6 months Retrocollis EOM defects Bulbar signs – Sucking, swallowing dysfunction – Facial palsy GAUCHER DISEASE (TYPE II) • Irritability • Later signs and symptoms – Dementia – Spasticity – Ataxia – Rare seizures – Trismus and stridor • Normal fundi GAUCHER DISEASE (TYPE II) • • • • • Splenomegaly > hepatomegaly Bones thinned; pathologic fractures common Pulmonary infiltrates Do not have Hurler phenotype Glucocerebrosidase deficiency GAUCHER DISEASE (TYPE II) • Can diagnosed by Gaucher cells in bone marrow • Neuropathology: – Little lipid storage – Neuron loss, especially in brainstem GAUCHER DISEASE (Type I; Adult) • Most common • Nervous system not involved • Treatment with – Replacement enzyme – Miglustat (Zavesca) • Inhibitor of glucosylceramide synthase, needed for synthesis of most glycospingolipids • Prevents accumulation of glucosylceramide • Also used in other forms of Gaucher, NP-C, GM1, and Tay Sachs NIEMANN-PICK DISEASE, TYPE A (ACUTE NEUROPATHIC) • Like Gaucher's, plus cherry-red spot in ~25-50% • Onset 3-9 months of life • Hepatomegaly > splenomegaly (often initial presentation) • Progressive intellectual and motor deterioration • Feeding difficulty and failure to thrive • Seizures infrequent NIEMANN-PICK DISEASE, TYPE A (ACUTE NEUROPATHIC) • Pathology – Ballooned neurons – Vacuolated histiocytes and lymphocytes (NiemannPick cells) • Sphinomyelinase deficiency • Autosomal recessive • Frequently Jewish CASE • Visceromegaly • Hexosaminidase A & B deficiency LATE INFANTILE, WITHOUT VISCERAL STORAGE • • • • • Neuronal ceroid lipofuscinosis Juvenile Tay-Sachs Progressive myoclonus epilepsies Huntington's chorea Xeroderma pigmentosa NEURONAL CEROID LIPOFUSCINOSIS • Usually autosomal recessive • Numerous eponyms, mixed features • Enzyme and genetic testing has generally replaced biopsies • Defects in lysosomal function NEURONAL CEROID LIPOFUSCINOSIS Type Infantile: INCL, CLN1 Late-infantile: LINCL, CLN2 Juvenile: JNCL, CNL3 Adult: ANCL, CNL4, 5 Eponyms Santavuori-Haltia Jansky-Bielschowsky Spielmeyer-Sjögren; Spielmeyer-Vogt; Batten Kufs (AR) Parry (AD) Usual age of onset 6-24 months 2-4 years 4-10 years Variable; usually 2nd-3rd decade Course Rapid Rapid Slower Slow Age at death 5-10 years 8-12 years 15-25 years Variable Manifesting symptoms Myoclonus, visual loss Seizures, particularly myoclonic Visual loss, dementia Extrapyramidal signs, ataxia Other symptoms Dementia, seizures, ataxia, acquired microcephaly Ataxia, dementia, late visual loss Seizures (less prominent), dysarthria, extrapyramidal signs Myoclonus, dysarthria, seizures, personality changes, neuropathy Retina Nonpigmentary degeneration Pigmentary degeneration Pigmentary degeneration Normal* ERG Decreased Decreased Absent VER Decreased Increased Absent Membranous inclusions Granular Curvilinear or rectilinear Fingerprints; vacuolated lymphocytes Granular NEURONAL CEROID LIPOFUSCINOSIS Type Infantile: INCL, CLN1 Late-infantile: LINCL, CLN2 Juvenile: JNCL, CNL3 Adult: ANCL, CNL4, 5 Eponyms Santavuori-Haltia JanskyBielschowsky SpielmeyerSjögren; Spielmeyer-Vogt; Batten Kufs (AR) Parry (AD) Enzymatic defect Palmitoyl protein thioesterase (PPT) Pepstatininsensitive lysosomal peptidase— tripeptyidyl peptidase 1 (some pts) CLN3 protein; trans-membrane chaparone, involved in folding of other proteins ? Also PPT in one family Lysosomal accumulation Sapsosin A, B Subunit C of mitochondrial ATP Subunit C of mitochondrial ATP Subunit C of mitochondrial ATP Genetic defect CLN1/PPT1 1p32 CLN2/TPP1 11p15.5 CLN3 16p12.1 CLN4 Mixed findings From Genetests.org NEURONAL CEROID LIPOFUSCINOSIS Pathology • Atrophy of both gray and white matter – Cerebral > cerebellar – Cerebellar prominent in CLN2 – Almost complete loss of cortical neurons in CLN1 • Lipopigments in neurons, glia, endothelial cells, liver, skin, WBCs, etc. • Retinal necrosis; almost complete loss of photoreceptors NEURONAL CEROID LIPOFUSCINOSIS Pathology • Vacuolated lymphocytes in CLN3 Bovine model of NCL Retina atrophy Granular osmophilic deposits Curvilinear inclusions Fingerprint inclusions NEURONAL CEROID LIPOFUSCINOSIS Imaging • • • • Atrophy Hypointense thalami on T2 Progressive WM signal on T2 ↓ ↓ N-acetylaspartate on MRS Now 14 NCL variants JUVENILE TAY-SACHS (PARTIAL GM2 GANGLIOSIDOSIS) • Variant 1 – Typical "gray matter disease“ • Seizures and dementia • Cerebellar and basal ganglia dysfunction • No cherry-red spot • Onset 5-10+ years, with 5-10 year course • Variant 2 – More like spinocerebellar degeneration – Onset between age 2 and adulthood CASE • • • • 5 y.o. Visual loss Starts losing cognition Age 8: a few seizures LATE INFANTILE, WITH VISCERAL STORAGE • Gaucher Type III • Niemann Pick, type C • Mucopolysaccharidoses – Hurler's – Hunter's – Sanfilippo's GAUCHER DISEASE (Type III; Chronic Neuronopathic) • Slower course – Onset early childhood to adult – Mild to severe mental retardation – Seizures and myoclonus (progressive myoclonus epilepsy) – Spasticity – Cranial nerve dysfunction – Eye movment abnormalities (e.g., oculomotor apraxia with failure of saccadic initiation, supranuclear gaze palsy) – Splenomegaly NIEMANN-PICK, TYPE C (CHRONIC NEUROPATHIC) • Similar to type A but onset later (> 2 years) and slower progression • Can have hepatic disease due to cholestasis even in neonatal period • Mild splenomegaly • Dementia • Marked spasticity • Apraxia of vertical gaze NIEMANN-PICK, TYPE C • • • • • • Ataxia Cataplexy Generalized tonic-clonic and myoclonic seizures Some with cherry-red spot Most die before age 10-15 Sphinomyelinase deficiency 1. Cherry red spots can be seen in all but which of the following disorders? A. B. C. D. E. Tay Sachs Generalized GM1 Gangliosidosis Infantile Neuroaxonal Dystrophy Niemann Pick type A Farber lipogranulomatosis 2. A 3-month-old boy comes in with seizures, subdural hemorrhages, and rib fractures. What metabolic disorder should be suspected? A. B. C. D. Leigh Niemann-Pick type A Alper Menke 3. Match the disorder with other organ involvement: Alper Retina Pompe Heart Neuronal ceroid lipofuscinosis Blood vessels Gaucher Liver Farber lipogranulomatosis Joints Menke Spleen 4. Which symptom is not common in girls with Rett syndrome? A. B. C. D. E. Perseverative speech Hand wringing Bruxism Hyperventilation Aerophagia 5. Match the disease and the gene or enzyme: Rett Hexosamindase A Alper PLA2G6 Tay Sachs Acid maltase Niemann Pick Mitochondrial DNA polymerase gamma (POLG) MeCP2 Pompe Infantile neuroaxonal dystrophy Sphingomyelinase 6. Which of the following is considered a mitochondrial disorder? A. B. C. D. E. Pompe Leigh Tay Sachs Gaucher Neuronal ceroid lipofuscinosis 7. For each of the neuronal ceroid lipofuscinoses, check off the most prominent initial symptoms. Seizures Infantile Late infantile Juvenile Adult Visual loss Myoclonus Dementia Extrapyramidal sx’s, ataxia 7. For each of the neuronal ceroid lipofuscinoses, check off the most prominent initial symptoms. Seizures Infantile Late infantile Juvenile Adult Visual loss Myoclonus Dementia Extrapyramidal sx’s, ataxia 7. For each of the neuronal ceroid lipofuscinoses, check off the most prominent initial symptoms. Seizures Infantile Late infantile Juvenile Adult Visual loss Myoclonus Dementia Extrapyramidal sx’s, ataxia 7. For each of the neuronal ceroid lipofuscinoses, check off the most prominent initial symptoms. Seizures Infantile Late infantile Juvenile Adult Visual loss Myoclonus Dementia Extrapyramidal sx’s, ataxia 7. For each of the neuronal ceroid lipofuscinoses, check off the most prominent initial symptoms. Seizures Infantile Late infantile Juvenile Adult Visual loss Myoclonus Dementia Extrapyramidal sx’s, ataxia 8. Name the metal associated with the disease: A. Menke: Copper B. Infantile Neuroaxonal Dystrophy: Iron 9. Match the disease and pathological finding: Infantile neuroaxonal dystrophy Glycogen storage Alper Pili torti Tay Sachs Ballooned cells with “torpedoed” axons Neuronal ceroid lipofuscinosis Spheroids Pompe Curvilinear, fingerprint, and granular osmophilic inclusions Menke Laminar cortical degeneration Case #1: girl with slow regression • Normal motor and cognitive development until age 2 • Then gradually lost ability to verbalize, with slower loss of comprehension • Progressive ataxia and weakness. Using walker by age 3. Stopped crawling by age 4. • Exam: No HSM. Followed a few commands. Nonverbal. Hypotonic but with spastic catch. Weak. Hyporeflexic. Ataxic. • Later, visual loss, seizures, hypertonicity, hyperreflexia • MRI: cerebellar and brainstem atrophy • EMG and nerve bx: mild axonopathy • Died age 10 • Dx: infantile neuroaxonal dystrophy INFANTILE NEUROAXONAL DYSTROPHY (INAD) • Onset age 6 months-3 years (classic form) • Slowly progressive • Combination of lower, then upper motoneuron signs: – Falling, clumsiness – Hypotonia, hyporeflexia with normal NCV's – Later, spasticity INFANTILE NEUROAXONAL DYSTROPHY • Also later – Optic atrophy, blindness – Involuntary movements, dystonia, decerebrate rigidity – Dementia – Seizures occur in a minority of pts • NCV's normal; EMG's suggest denervation • Autosomal recessive INFANTILE NEUROAXONAL DYSTROPHY • Iron in globus pallidus in 40-50% • Cerebellar atrophy Case #2: girl with slow regression • History of 32-week prematurity and neonatal hepatitis, HSM that resolved. • Started walking at 17 months, always a toe-walker. Delayed but could ride a bike at age 5. • Seizures starting at 18 months. • Age 6 began to have spells of becoming limp and falling when she was excited. • When she presented to us at age 5, she was microcephalic, and had oculomotor apraxia, truncal hypotonia but tight heel cords, dysmetria and ataxia. • Progressive ataxia, dysphagia, loss of speech, and loss of ability to voluntarily look up, then down (but could be “dolled”). • Died age 10 • Dx: Niemann-Pick, type C NIEMANN-PICK, TYPE C (CHRONIC NEUROPATHIC) • Similar to type A but onset later (> 2 years) and slower progression • Can have hepatic disease due to cholestasis even in neonatal period • Mild splenomegaly • Dementia • Marked spasticity • Apraxia of vertical gaze NIEMANN-PICK, TYPE C • • • • • • Ataxia Cataplexy Generalized tonic-clonic and myoclonic seizures Some with cherry-red spot Most die before age 10-15 Sphinomyelinase deficiency Case #3 – boy with rapid regression • Normal until 7 months • Then low grade fever without source, fussy, and regressed • Stopped rolling, scooting; lost head control. Weaker on left. • Initially very floppy but progressively hypertonic. • Regressed episodically. Frequent fevers. • Progressive dysphagia, and stopped feeding. Hyperventilation. • Infantile spasms • Brother with same problem but slower progression • No known consanguinity but from “very stable community” • Exam: truncal hypotonia, limb hypertonia, brisk DTRs • Lactate 29 (up to 2.2); pyruvate 1.2 • MRI: high T2 signal in basal ganglia • Brother had similar MRI • Died age 2-1/2 • Brother died age 14 years • Dx: Leigh syndrome LEIGH SYNDROME (subacute necrotizing encephalomyelopathy) • Onset in early infancy (60% in 1st year) or childhood; rarely in adulthood • Neonatal form – Acidosis – Severe retardation – Usually early death • Other types with variable clinical picture: – Steadily progressive, saltatory, or episodic – May progress with intercurrent infections – Typically associated with lactic acidosis LEIGH – Symptoms and signs • • • • • • • Retarded motor and intellectual development Respiratory disturbances Ophthalmoplegia Dysphagia and weight loss Vomiting Hypotonia & weakness Ataxia LEIGH – Symptoms and signs • • • • • • Seizures Visual loss Nystagmus Dystonia Peripheral neuropathy (often subclinical) Fevers LEIGH - Pathology • Brainstem and basal ganglia lesions common • Necrosis around 4th ventricle and aqueduct. • Distribution resembles Wernicke's without mammilary bodies and without hemorrhage Figure 1. Sequential FLAIR (fluid-attenuated inversion recovery) MR images of the brain Goldenberg, P. C. et al. Neurology 2003;60:865-868 Case #4 – a true unknown! How would you work him up? • 11 y.o. boy seen in clinic for developmental decline and myoclonus • PLD normal • Early development normal; “riding twowheeler at age 2” • Age 4: began to be rigid in his routines; sensitive to a variety of stimuli • KG: reading 10 words, c/w 20-word average; not counting as high Age 6: 1st seizure; clonic; focal EEG (posterior) Development plateaued Seizure-free on oxcarb until age 10 Then recurrent clonic seizures, affecting either or both sides of body • Frequent generalized myoclonic jerks • Starting at age 10, progressive ataxia, cognitive loss, dysarthria • • • • – Now crawls to ambulate – Comprehension ok and good sense of humor; difficulty thinking of words Work-up? • Whole exome analysis •News since the last talk! • Late infantile NCL Case #2 • GM1 37117055 Case #4 • Juvenile TS Tips for next talk • Add CDG? 33051487 – no; do as clinic 10:00 case. • Timing was fine. A little dry in the middle. Cases are good idea. • Perhaps add a brief case at the end of each of the 4 sections.