Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
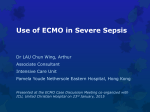
Complessità nell’infarto evolvente complicato da disfunzione ventricolare sinistra Angelo Sante Bongo Aritmiche Ischemiche Meccaniche Complicanze dell’IMA Aritmiche Ischemiche Meccaniche Complicanze dell’IMA Diagnosi anatomo coronarica precoce Rivascolarizzazione , se indicata Supporto a ventricolo Ruolo dell’emodinamista “Defibrillation was attempted again but remained unsuccessful. CPR continued. We suspected that the patient’s heart was too distended to permit termination of ventricular fibrillation … a decision was made to consult cardiac surgery about the initiation of extracorporeal membrane oxygenation (ECMO) for full hemodynamic support and to decompress the heart and facilitate termination of ventricular fibrillation.” n engl j med 369;11 nejm.org september 12, 2013 Aritmiche Ischemiche Meccaniche Complicanze dell’IMA Shock cardiogeno Trombosi coronarica no reflow Complicanze ischemiche e Shock cardiogeno Trombosi coronarica no reflow Complicanze ischemiche e Shock cardiogeno Trombosi coronarica no reflow Complicanze ischemiche e •L’attuale terapia di rivascolarizzazione ha ridotto la mortalità per IMA a meno del 5% •La più frequente causa di mortalità post-IMA, lo shock cardiogeno, complica 8-12% nello STEMI e 5% nel NSTEMI •Mortalità attuale 40-50 % Shock cardiogeno post IMA Trends in the incidence rates of cardiogenic shock in patients with acute myocardial infarcts. Goldberg et al. Thirty-year trends (1975 to 2005) in the magnitude of,management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction Circulation 2009;119:1211 1 in 20 Trends in hospital case fatality rates in patients with acute myocardial infarct according to the presence of cardiogenic shock. 40% Trattamento del Tronco comune Trattamento di tutte le lesioni coronariche Contropulsatore aortico Assistenza ventricolare Disfunzione Ventricolare sinistra: il ruolo dell’Emodinamista 01/03/17 25 SHORT TERM Sostegno al flusso SI gonfia durante la Diastole Contropulsatore Aortico Datascope/Arrow CONTROPULSATORE 01/03/17 28 Si sgonfia durante Systole IABP in MI without shock Recent data for IABP Intra-aortic balloon pump: indications, efficacy, guidelines and future directions. Curr.Opin Cardiol. 2014 Jul;29(4):285-92. IABP in cardiogenic shock IABP-SHOCK II : the largest randomized control trial ever performed in cardiogenic shock - randomised 600 patients enrolled in 37 centres in Germany from June 2009 to March 2012 Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 2012; 367:1287-1296. IABP-SHOCK II STUDY Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 2012; 367:1287-1296. IABP-SHOCK II STUDY Primary Study Endpoint: 30-DAY Morality Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 2012; 367:1287-1296. IABP-SHOCK II STUDY Conclusions: Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 2012; 367:1287-1296. . Lancet.2013 Nov 16;382(9905):1638-45 IABP in cardiogenic shock 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction:Circulation 2013; 127:e362–e425. 2014 ESC/EACTS guidelines on myocardial revascularization:European Heart J (2014)35;2541-2619 Femoral cannulation for veno-arterial (VA) ECMO … RA/IVC drainage from CFV access (23/25F) …venous return limits flow Arterial inflow (17F) … “downsize” Distal arterial inflow (6F) … “downsize” …“open” versus “percutaneous” access ? *no complications *exit strategy VAda ECMO VenoArterial (distal artery) ECMO Non physiologic and inherently unstable Efficacy proportional to LVEF Retrograde arterial flow … LVEF and cerebral perfusion, LVEDP ! Distal malperfusion … The patient … sedate and non-ambulatory Blood path and directional flow … Family of MACS INTERMACS® – A North American registry established in 2005 for patients who are receiving mechanical circulatory support device therapy to treat advanced heart failure. PediMACS – The pediatric portion of INTERMACS. While INTERMACS has always included durable devices implanted in pediatric patients, pediMACS has been developed to focus on capturing data elements unique to pediatric patients. MedaMACS – The Medical Arm of Mechanically Assisted Circulatory Support (MedaMACS Registry), a prospective study of medically managed advanced heart failure patients, will report the nature of optimal contemporary medical therapy for heart failure and provide information on medical outcomes in terms of timed endpoints of mechanical support, transplant, or death through two years of follow-up. IMACS – The International Society for Heart and Lung Transplantation Registry for Mechanically Assisted Circulatory Support (IMACS) is an international registry intended to enroll and follow patients who receive durable mechanically assisted circulatory support devices (MCSD) in all countries and hospitals that wish to participate. 50 la macchina (VAD) • La disfunzione ventricolare sinistra post IMA evolvente in SHOCK cardiogeno è una complicanza gravata ancora oggi da elevata mortalità. • La terapia medica massimale nei casi più gravi non consente un adeguato recupero • Il contropulsatore aortico non garantisce alcun miglioramento di sopravvivenza ma va considerato come “bridge” per una assistenza ventricolare più avanzata • L’ECMO rappresenta un mezzo di supporto circolatorio più utile per consentire un recupero finalizzato ad una terapia di supporto con VAD ed eventuale successivo trapianto • L’impianto di VAD in fase acuta , nonostante la maggior gravità di esordio offre nei pazienti con IMA, gli stessi vantaggi dell’impianto nei pazienti senza IMA . Il suo impiego andrà validato con studi prospettici Conclusioni • Lo sviluppo di tecniche di assistenza avanzate in grado di supportare il ventricolo sin nella fase acuta dello IMA impone una riorganizzazione in rete che, analogamente a quanto si è verificato per la riperfusione coronarica, consenta a tutti i pazienti in shock cardiogeno post IMA (e non IMA) di raggiungere i centri qualificati prima che si verifichi un deterioramento irreversibile del danno miocardico Conclusioni Conclusions Transcatheter closure of PIVSRs can be performed with high technical success and relatively low procedural complication rates; however, in the acute setting it is associated with very high in-hospital mortality rates. Device closure appears well suited to treatment of patch leaks post surgical repair in particular, thus a hybrid strategy of early surgical repair with transcatheter closure of patch leaks as needed is preferable for primary PIVSRs regardless of haemodynamic status. T Transcatheter closure can also be considered in patients who are not surgical candidates, generally have haemodynamically tolerable defects, and survive a period of watchful waiting. Long-term outcomes appear good in patients with or without prior surgery who are treated subacutely and survive to hospital discharge. Conclusioni Il ruolo ell’emodinamista è cruciale nella gestione dell complicanze IMA I casi più complessi debbono essere affrontati in centri con heart team Il contropulsatore non è più indicato nello shock cardiogeno ma si deve utilizzare l’assistenza ventricolare La rottura del setto post IMA può essere affrontato con chiusura percutanea in casi selezionati in laboratori che praticano trattamento delle cardiopatie strutturali Il trattamento con assistenza ventricolare del post arresto ed il trattamento della rottura del papillare necessitano di ulteriori validazioni Among 98 patients … cardiogenic shock (34), ventricular fibrillation or pulseless ventricular tachycardia (23), or asystole /pulseless electrical activity (41) 96% underwent emergency revascularization (2 received CABG) with successful angioplasty achieved in 71% (TIMI 3 flow) 55% were weaned from ECLS … ECLS-related complications occurred in 36%... cannulation site bleeding All-cause in-hospital mortality rate was 67.3%, and the survival rate to hospital discharge was 32.7% Aritmiche Ischemiche Meccaniche Complicanze dell’IMA Complicanze meccaniche dell’ IMA PRECOCI ROTTURA SETTO INTERVENTRICOLARE ROTTURA DI PARETE LIBERA PAPILLARE ISCHEMICO (insuff. Mitralica) TARDIVE ANEURISMA DEL VENTRICOLO SX PSEUDOANEURISMA ISCHEMIA PAPILLARE CRONICA