Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Maternal health wikipedia , lookup
Patient safety wikipedia , lookup
Public health genomics wikipedia , lookup
Social determinants of health wikipedia , lookup
Race and health wikipedia , lookup
Health system wikipedia , lookup
Health equity wikipedia , lookup
Reproductive health wikipedia , lookup
Electronic prescribing wikipedia , lookup
Rhetoric of health and medicine wikipedia , lookup
International Association of National Public Health Institutes wikipedia , lookup
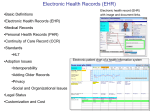
Public Health Data Standards Consortium http://www.phdsc.org The Consortium is a unique entity made up of federal, state and local agencies, professional associations, academia, health IT vendors and individuals that collectively represent the interests of public health in the health IT standardization. PHDSC Ad Hoc Task Force on Electronic Health Record-Public Health (EHR-PH) http://www.phdsc.org/health_info/ehr-task-force.asp 2004 PHDSC EHR-PH Task Force Goal: To provide a public health perspective to the evaluation of the HL7 EHR-S Functional Model Objectives: ■ Bring the state and local public health agencies and public health research community’s perspectives into the on-going efforts to develop the HL7 Functional Model for the EHR-S ■ Demonstrate the benefits of an organized interaction between the public health and clinical health care 2004 PHDSC EHR-PH Task Force WHITE PAPER “Electronic Health Record: Public Health Perspectives” http://www.phdsc.org/health_info/pdfs/PHDSC_EHRPH_WhitePaper2004.pdf Purpose: ■ To communicate to the public health community a need for broader involvement in the national effort to standardize clinical and public health data and information systems ■ To describe public health perspectives on the EHR 2010 PHDSC EHR-PH Task Force Re-evaluation of HL7 EHR-S FM V1.1 from Public Health Perspectives Supported by the National Center for Health Statistics (NCHS) Centers for Disease Control and Prevention (CDC) Grant No. 5U38HM000455-02 2010 PHDSC EHR-PH Task Force Project Objective: Conduct re-evaluation of HL7 EHR-S FM Release 1.1 to identify necessary functionality for public health reporting and information sharing across clinical EHR-S and public health information systems Re-evaluation of HL7 EHR-S FM from PH Perspectives Why Now? ■ HL7 EHR-S FM has undergone a series of enhancements ■ Public Health better positioned itself at HL7 by Participation in Public Health and Emergency Response Work Group (PHER WG) Participation in HL7/ONC/EHR Biosurveillance Use Case Alignment Project ■ Public Health has been involved in the national HIT standardization efforts at HITSP, IHE and other initiatives ■“Meaningful use of EHR-S” warrants meaningful use of public health information systems ■ CDC/NCHS contract with PHDSC 2010 PHDSC EHR-PH Task Force Participants: 93 members joined the Task Force 50% increase in comparison with 2004 EHR-S FM evaluation with 63 members Limitations: All public health domains are not represented 2010 PHDSC EHR-PH Task Force Participants Affiliation* Stakeholders Number of Participants Local Public Health 12 State Public Health 25 Federal Agencies Professional Associations 25 (CDC=22, VA=1, NIST=1, FDA=1) 4 (PHDSC, NAPHIT, AHIMA) Academia 4 Payor 2 Clinicians 1 IT vendors 19 (EHR=4, PH=15) Total 92 *We were unable to specify stakeholder category for 1 participant. 2010 PHDSC EHR-PH Task Force Public Health Participant Jurisdictions: Public health participants range from local and state health departments in 17 states as follows: AK CA CO DE IL KY MA MI MN NC NE NY OH OR SD TN TX 2010 PHDSC EHR-PH Task Force Domain/Stakeholder Representation*,** Domain Number of Participants Communicable Diseases 13 Chronic Diseases (including Cancer) 11 Immunization 9 Vital Records 9 Environmental Health 1 Public Health Informatics 24 IT, HIT Standards, HIM, EMR, EHR 38 Law (including HIPAA) 2 Primary Care 3 Behavioral & Occupational Health 2 Birth Defects 1 *Participants may have expertise in several domains. **Several participants did not specify their area of expertise. 2010 PHDSC EHR-PH Task Force Participants have sufficient expertise for evaluating domains included in the Meaningful Use of Health IT Electronic Reporting from EHR-S to Public Health on: Communicable diseases (N=13) Immunizations (N=9) Biosurveillance (N= 24) Communicable and chronic disease surveillance based on ASTHO definition Plus expertise in: Chronic diseases (11) Vital records (9) Information Technology (38) Public Health Informatics (24) 2010 PHDSC EHR-PH Task Force Timeline Methodology 12/20091/2009 Recruit participants for the HL7 EHR FM Re-evaluation 1/14/10 Re-launch the PHDSC Ad Hoc Task Force on EHR-PH 3/30/10 Solicit feedback on the Model from Task Force Participants 5/14/10 Build an agreement among participants on proposed revisions/additions 5/22/10 Present proposed revisions/additions to the HL7 EHR SWAT team for inclusion in the ballot 5/31/10 Generate Recommendation Report document 9/2009 1/2010 5/2010 Present project updates at the HL7 Working Group Meetings 5/26/10 Deliver a webinar for a public health community 2010 PHDSC EHR-PH Task Force Participation Process Reviewed sections of the EHR-S FM Submitted revisions to the Project Team via e-mail using Excel spreadsheet Received spreadsheet with proposed revisions prior calls Review revision resolution outcomes Participated in the revisions resolution with the HL7 EHR SWAT Team Reviewed proposed revisions during the calls Work with the HL7 EHR WG to incorporate proposed revisions in the HL7 EHR-S FM R2 ballot 2010 PHDSC EHR-PH Task Force Comments HL7 EHR-S Functional Model Care Management DC.2 Clinical Decision Support DC.3 Operations Management and Communication Supportive S.1 Clinical Support S.2 Measurement, Analysis, Research and Reports S.3 Administrative and Financial IN.1 Security IN.2 Health Record Information and Management IN.3 Registry and Directory Services IN.4 Standard Terminologies & Terminology Services IN.5 Standards-based Interoperability IN.6 Business Rules Management IN.7 Workflow Management Information Infrastructure Direct Care DC.1 Source: HL7 EHR-S FM Overview CDC PHDSC HL7 EHR-S FM Evaluation 17 HL7 EHR-S Functional Model ID Layout of the FM: Functional Identification Function Type Functional Name Functional Statement Functional Description “See also” column Conformance Criteria Type Name Statement (Normative) (Normative) Number Description See Also Conformance Criteria HL7 EHR-S Functional Model ID Type Name Statement Description DC.1.5 F Manage problem list Create and maintain patient-specific problem list A problem list may include, but is not limited to: Chronic conditions, diagnoses, or symptoms, functional limitations, visit or stay-specific conditions, diagnoses, or symptoms. Problem lists are managed over time, whether over the course of a visit or stay… See Also Conformance Criteria IN.2.5.1 IN.2.5.2 1. The system SHALL display all active problems associated with a patient. 2. The system SHALL create a history of all problems associated with a patient. 3. The system SHALL retrieve a history of all problems associated with a patient. 4. The system SHALL provide a user interface to deactivate a problem. 5. The system MAY provide the ability to re-activate a previously deactivated problem. 6. … Source: HL7 EHR-S FM Direct Care Chapter CDC PHDSC HL7 EHR-S FM Evaluation 19 2010 PHDSC EHR-PH Task Force Evaluation Outcomes: HL7 EHR-S FM Functions Categories Total Comments Received Newly Proposed Conformance Criteria Comments Resolution Outcomes (Accepted / Rejected) Direct Care 259 15 155 / 0 Supportive 13 1 13 / 0 Infrastructure 12 0 12 / 0 TOTAL 284 16 284 2010 PHDSC EHR-PH Task Force Comments Examples Direct Care Comments Section New- Facility Demographics DC.1 Care Management Recommendation comments Add Country, province, address elements 4 Capture mode of transport (e.g. airplane birth) Capture information surrounding incident (e.g. trauma, foodborne illness, communicable disease) Care communications to/from public health (e.g. alerts) 1 MAY…SHALL Existing infrastructure support 3 1 2 Direct Care Comments Section Recommendation # DC.1.1 MAY…SHOULD provide ability to store/reference imaged documents Record -data SHOULD be captured using standardized code sets or nomenclature management -provide the ability to store/reference imaged documents 3 MAY…SHALL provide the ability to receive, store and present text-based externally-sourced documents and reports -ability to receive/store/present text-based externally-sourced docs/reports 2 SHOULD…SHALL provide the ability to request correction of the administrative or financial data 1 Defer elevate in domain-specific profiles; covered in the externally sourced information; To be covered by Data Profiles; not universal need 9 NEW: Lab Orders SHOULD contain complete demographic info -SHALL prevent patient-sourced data from overriding provider-sourced -SHALL provide the patient the ability to annotate provider-sourced data -Add to supportive functions S.2.2.2 as another example, there may be standard reports for public health -SHALL provide ability to Capture and Maintain multiple patient names -shall provide the ability to capture and maintain historical demographic data -Ability to combine demographic and clinical data for PH submission 7 Direct Care Comments Section DC.1.2 Manage Patient History DC.1.3 Preferences, Directives, Consents and Authorizations Recommendation comments MAY…SHOULD provide the ability to capture the relationship between patient and others. 1 SHOULD…SHALL conform to function IN.1.4 (Patient Access Management) 1 Not in most systems at this time; cover under Data Profiles 5 cover under Data Profiles 2 MAY…SHOULD provide the ability to generate printable consent and authorization forms. -display the authorizations associated with a specific clinical activity 2 NEW: the system SHOULD provide the ability to manage electronic signature of the patient for consents and authorizations 1 Direct Care Comments Section DC.1.4 Summary Lists Recommendation comments Update Add to 2.6.2 description … of a health risk (e.g. notifiable and reportable conditions such as communicable disease, adverse drug event or patient safety reports) within the cared for population..... 1 SHOULD…SHALL provide the ability to capture a report of No Known Drug Allergies 1 Description addition: Medication lists are not limited to medication orders recorded by providers, but may include, for example, pharmacy dispense/supply records, patient-reported medications and additional information such as age specific dosage. Medication provided by public health during a mass prophylaxis (e.g. H1N1 vaccinations) would also be included. 5 Include in Data Profiles; already covered in supportive 2 Description addition: Medication provided by public health during a mass prophylaxis (e.g. H1N1 vaccinations) would also be included. 1 MAY…SHOULD provide the ability to capture information regarding the filling of prescriptions 1 Direct Care Comments Section Recommendation comments DC.1.4 Summary Lists Description Addition: For example, Behavioral risk factors such as tobacco/alcohol use, social history, significant trends (lab results, weight); Description Addition: problem list Description Addition: for clinical, administrative, public health, financial decision-making 3 MAY…SHOULD provide the ability to re-activate a previously deactivated problem -provide the ability to associate encounters, orders, medications, notes with one or more problems 2 NEW: SHOULD prepare a report of a patient ‘s immunization history upon request of the patient, personal representative or for appropriate authorities such as schools or day-care centers 1 Direct Care Comments Section Recommendation DC.1.5 Manage Assessm ents Added Social history examples to 2.1.3 1 cover under Data Profiles 1 MAY…SHOULD provide the ability to link data from external sources, laboratory results, and radiographic results to the standard assessment. 1 Description addition: Guidelines and protocols presented for planning care may be site specific, community, industry-wide standards or as specified by public health. Description addition: Provide administrative tools for healthcare organizations and public health authorities 2 Not in most systems at this time; 1 MAY…SHOULD provide the ability to use information from DC.2.1.4 (Support for Patient and Family Preferences) to improve the effectiveness of care and treatment plans. 1 DC.1.6 Care Plans, Treatment Plans, Guideline s, and Protocols comments Direct Care Comments Section DC.1.7 Orders and Referrals Management Recommendation # Description addition: Different medication orders, including discontinue, refill, and renew, and disposal require -Orders should be communicated to the correct service provider for completion and . -Order status will be monitored and alerts sent for uncompleted orders. 3 cover under Data Profiles; covered in supportive/infrastructure functions; Not universal need; 8 MAY…SHALL make common content available for prescription details to be selected by the ordering clinician - conform to function S.3.3.2 2 MAY…SHOULD provide the ability for the ordering clinician to create prescription detail - make available common patient med instruction content to be selected by tordering clinician. - provide the ability to include prescriptions in order sets -provide the ability to re-prescribe medication by allowing a prior prescription to be reordered --provide order sets for referral preparation - provide guidelines to the provider about the appropriateness of a referral -Update DC.2.4.1 to SHOULD -provide the ability for a provider to choose from among the order sets pertinent to a certain disease or other criteria 7 NEW: the system SHOULD provide the ability to communicate order activity to public health authorities as required by jurisdictional law. - The system should report medication orders, where appropriate, to public health authorities (e.g. oncology related medi.orders should be communicated or transmitted to cancer registry). 2 Direct Care Comments Section Recommendation # DC.1.8 Document ation of Care, Measure ments and Results Description addition: The system should report medication administration, where appropriate, to public health authorities (e.g. oncology …). - Results of tests presented in easily accessible manner to appropriate providers and to PH agencies where public health is a care provider (e.g. newborn screening results) - route results to other care providers, e.g. nursing home, consulting physicians, PH provider… 3 cover under Data Profiles; covered in supportive/infrastructure functions; Not universal need; 2 MAY…SHOULD notify the clinician when specific doses are due -conform to function DC.2.3.1.1/2 (Support for Drug Interaction Checking/Patient Specific Dosing /Warnings), and check/report allergies, drug-drug interactions, and other -- provide the ability for providers to annotate a result. --display a link to an image associated with results. 4 SHOULD…SHALL provide ability to recommend required immunizations per pt. risk factors; provide the ability to capture other clinical data pertinent to the immunization administration; SHALL transmit/receive required immunization info to PH immunization registry either directly or via an intermediary, indicate normal and abnormal results; notify relevant providers (ordering, copy to) that new results have been received 4 NEW: If a public health immunization registry is available, the system SHALL provide the ability to extract the required information to submit to a public health immunization registry. - New Subsection 2.6.1.2 ( patient level surveillance) The system SHALL transmit appropriate patient-level clinical information (e.g. results) to public health notifiable condition programs - system SHALL provide ability to present numerical/non-numerical current/historical test results to appropriate provider and to public health entities meeting disease reporting criteria. 3 Direct Care Comments - pending Section DC.1.8 Documentation of Care, Measurements and Results DC.1.9 Generate /Record PatientSpecific Instructions Recommendation # MAY…SHOULD 4 SHOULD…SHALL 1 NEW:- When available, a clinical decision support system MAY provide target values indicated by public health (e.g., Health People 2010 goal mean total blood cholesterol) -Add: system functionality Should track and report when decision support alerts have been disabled. The system may be configured to notify the user of the status of alerts --Add: the system SHOULD be able to provide the patient with this information electronic as well as in paper form 1 Recommendation for future policy modeling work for Public Health 1 Add: The instructions shall not only be available to the patient through screen prints/paper form -- but also electronically. 1 Direct Care Comments - pending Section DC.2 Clinical Decision Support DC.3.1 Clinical Workflow Tasking Recommendation # Description:-append Including failure to report a reportable condition to public health -add geographic proximity (e.g., zipcodes) to the list of potentially shared items of interest -extend resource examples to include information on local disease incidence rates and open public health investigations. -add (e.g. public health education materials) 4 MAY…SHOULD 28 SHOULD…SHALL 15 NEW: The system SHOULD provide the ability to configure rules defining abnormal trends and public health reportable conditions -The system SHALL have the capacity to identify, track and provide alerts, notifications and reports about variances from standard care plans, guidelines and protocols. -The system SHOULD make data available for aggregation. -A system MAY provide the patient pop. health measures specific to their condition /location -The EHR system MAY accept question sets supporting outbreak investigation (eg., exposure questionnaires, contact tracing) from public health authorities to facilitate information gathering from the patient. 5 Description: Include PH authorities in the 1st sentence to emphasize the importance of including PH 1 MAY…SHOULD 10 SHOULD…SHALL 4 Recommendation for future policy modeling work for Public Health 6 Supportive/Infrastructure Functions Comments Section Recommendation # S.1 Clinical Support MAY…SHOULD 3 S.2 Measurement, Analysis, Research and Reports MAY…SHOULD 1 S.3 Administrative and Financial Description: Add: The system SHALL provide the ability to report to public health 1 MAY…SHOULD 5 IN.1.1 Entity Authentication Description: Replace "disaster" with "emergency" 1 IN.2.4 Extraction of Health Record Information SHOULD…SHALL 5 IN.3 Registry and Directory Services MAY…SHOULD 6 2010 PHDSC EHR-PH Task Force Recommendations 2010 PHDSC EHR-PH Task Force Our Recommendations: Incorporate revisions identified by the Task Force members into the HL7 EHR FM release 2 ballot Add 16 new conformance criteria as extensions to the EHR-S FM Consider the development of a Public Health Functional Profile as a basic approach for identifying certification criteria for standards-based HIT products 2010 PHDSC EHR-PH Task Force Our Recommendations (continued): Work with HL7 EHR WG on defining a new specification entitled “Data Profile” as a supporting document to the Functional Profile that will define standardized data set(s) for information exchanges Additional work is needed to better define the need for an independent HL7 Public Health Functional Model that will define functions for non-clinical data sources, e.g., environmental and socio-economic data 2010 PHDSC EHR-PH Task Force Next Steps: --Current Project- Continue working with HL7 EHR Working Group on the comment reconciliation for the EHR-S FM Release 2 ballot during 2010 2010 PHDSC EHR-PH Task Force Next Steps: -- New Project - Conduct a pilot project in 2010-2011in collaboration with HL7 EHR WG and PHER WG to develop a methodology for using Functional Profiles and Data Profiles to establish certification criteria for standards-based HIT products Work with Early Hearing Detection and Intervention program on defining an approach for setting certification criteria with support from CDC 2010 PHDSC EHR-PH Task Force More Information about Our Project: PHDSC web-site http://www.phdsc.org/health_info/ehr-task-force.asp PHDSC project wiki http://wiki.phdsc.org/index.php/EHR-PH_Project 2010 PHDSC EHR-PH Task Force Why is This Work Important for Public Health? 2010 PHDSC EHR-PH Task Force Potential Impacts to Public Heath Influence of ARRA and HIE on Health IT Standards Public Health Infrastructure Public Health Policy and Legislation Practice of Public Health 2010 PHDSC EHR-PH Task Force Influence of ARRA and HIE These initiatives explicitly mention cooperation/collaboration with “public health” Many jurisdictions will focus on “low hanging fruit” and high priority areas: Immunization registries Disease surveillance ANY standardization will help public health sift through the data that will be sent to public health departments 2010 PHDSC EHR-PH Task Force Public Health Infrastructure Public Health will need to be able to accept the information that will soon be collected at the Point of Care via EHR-S Substantially MORE information is expected to flow into public health departments as the collection of data moves from a paper-based collection/reporting approach to an electronic collection/reporting approach Advanced knowledge of the structure/nature of the data will help when adapting, modifying or creating systems to capture this information. 2010 PHDSC EHR-PH Task Force Public Health Policy and Legislation HIE and ARRA will likely cause evaluations of public health policy, legislation and administrative rules governing public health Understanding the EHR-S Functional Model from public health perspectives can help shape the discussion of the dialogue on policy changes 2010 PHDSC EHR-PH Task Force Practice of Public Health Better understanding of current health of the community through more accurate and timely reporting of data Evidence-based data also results in greater potential for quantifiable measurements and predictions Data-driven model will help manage the collection AND subsequent evaluation of the public health interventions Get Involved! Anna Orlova, PhD, Executive Director 624 N. Broadway Room 325 Baltimore MD 21205 Phone: 410-614-3463 Fax: 410-614-3097 E-mail: [email protected] 2010 PHDSC EHR-PH Task Force Questions? Comments?