Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
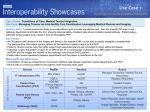
Clinical health information technology (HIT) is being more widely adopted and can support better care delivery in a complex environment. The vendor market is equally complex, with many (often expensive) choices and no consistent way of evaluating what different systems can do. This fact sheet provides a simple framework to help identify the key differentiators between some of the most commonly used tools in the ambulatory setting: electronic health record (EHR) systems and chronic disease management systems (CDMS), also known as disease registries. Of all the HIT tools, these two are especially important in terms of potential to improve the clinical care of patients with chronic conditions. Table 1 compares the key features of EHR and CDMS tools. Commentary The most important question that an organization needs to answer in choosing its IT system is: “What problem(s) are we trying to solve?” After requirements development and selection, implementation must be addressed. All too often, organizations implementing EHRs or CDMSs fail to take advantage of the full capability of whichever system they select. The optimal use of either type of technology requires a change in how clinical care is practiced—in paper-based systems, workflows are designed to deal with paper “tools” while electronic tools require new workflows and training. Use of CDMSs to improve population care (often for chronic disease management) can be thought of as a “stepping stone” toward more comprehensive computerization of data (including EHR and electronic documentation). CDMS systems often provide the opportunity to create and support new team working relationships but do not require all those “touching” the system to use the computer as part of their daily interactions with patients. Provider teams become accustomed to pulling up appropriate information to support planned visits for patients, relying on a computer (or computer printout) for key prompts and reminders, and using reports to support patient follow-up and outreach. These systems are well suited to organizations focusing on quality improvement and that might not have significant resources to finance an EHR purchase and implementation or have a large support staff to maintain it. EHR implementation requires a bigger investment (in terms of time, funds, and staff ) and more significant re-engineering of clinical workflow. Team members would use keyboards or touch screens instead of paper; hardware and software requirements are more extensive (and expensive); and interactions with patients must be altered to avoid provider-computer (as opposed to providerpatient) interactions. The information available for an individual patient is much more robust if C A L I FOR N I A H EALTH C ARE F OU NDATION fact sheet Electronic Health Records versus Chronic Disease Management Systems: A Quick Comparison M arch 2008 Table 1. Comparison of Key Features in EHRs and CDMSs Key Features Electronic Health Records Chronic Disease Management Systems Definition An electronic record of patient health information, including patient demographics, conditions, medications, vital signs, medical history, immunizations, notes, laboratory data, and radiology reports that can generate a complete record of a clinical patient encounter. An electronic system used to capture, manage, and provide information on specific conditions to support organized care management for patients. Approach Individual patient based. Population based. When fully implemented, can represent a legal patient record (and eliminate the need for a paper chart). Does not represent a legal patient record (requires a supporting paper chart or EHR). Not optimized for population management or populationbased reporting; would require customization. Optimized to manage specific conditions across patients including support of population-based reporting. Electronic documentation of patient visits (including non-office visits) with tools and templates for large amounts of clinical data. Requires planned data migration from paper charts. Limited documentation of patient interactions, data usually focused on identified medical conditions (such as diabetes, immunizations, etc.). Documentation and Reporting Variable amounts of structured or coded data that supports search, analysis, and reporting. Limited flexibility in recording miscellaneous and patient-reported information. Support of Team Care Supports team care (including messaging between team members). Variably “task-driven” outlining steps and follow-up actions required by staff for individual patients. Supports team care (through common documentation that can be seen simultaneously). Level of Integration Can be integrated with practice management systems. Ability to assign evaluation and management codes, and more generally support billing processes. May have one-way interface with practice management systems. Less tuned to support billing. E-Prescribing Support Can support e-prescribing as a separate module or integrated with the EHR; can support electronic lab ordering and results reporting. Generally does not support e-prescribing. Level of Sophistication and Support More sophisticated technology, requiring more robust implementation and support services. Simpler technology; typically limited implementation and support services required. Implementation and Maintenance Longer implementation timelines; more difficult and expensive to maintain. Shorter implementation timelines; easier to maintain; and less expensive. Can be implemented incrementally; for example, starting with front office staff. Training Requires significantly more training for both physicians and staff and greater computer literacy. Requires some training, but less intensive than for EHR. Impact on Workflow Processes Significantly greater impact (requiring more change) to workflow processes; generally requires intensive provider use of computers. Less significant impact to workflow; might not require provider use of computers. Attributes Common to Both Systems Able to incorporate guidelines and standards and remind providers about appropriate or required care. Relies on a separate charting process (paper or electronic). Prompts and relevant data easily retrievable at time of patient visit. Standard and ad-hoc reporting functions support patient outreach tools (such as reminder letters or call-back lists). Human intervention needed to confirm appropriate diagnoses and enter data. Management support for multiple co-morbid conditions generally not available (relative prioritization of recommendations). Patient education and instruction tools usually limited to English. Interoperability with other vendors not optimal and not built-in. Source: Laura Jantos and Michelle Holmes, IT Tools for Chronic Disease Management: How Do They Measure Up?, California HealthCare Foundation, July 2006 (www.chcf.org/topics/chronicdisease/index.cfm?itemID=123057). | California HealthCare Foundation the investment is made to put that information into the system (that is, by manual entry, scanning, and electronic interfaces with labs, e-prescribing systems, etc.). Factors in Choosing an Approach: “Stepping Stones” or “A Cold Plunge”? n Level of leadership’s commitment to change; n Readiness and ability to change workflow practices; n Computer skills across care team; n Capital for hardware, software, and connectivity; and n Priority: population management vs. individual care. f o r m o r e i n f o r m at i o n Robert H. Miller and Christopher E. West, “The Value of Electronic Health Records in Community Health Centers: Policy Implications,” Health Affairs, Vol. 26 No. 1, January/February 2007, pp. 2006-14. n Alexandra E. Shields et al, “Adoption of Health Information Technology in Community Health Centers: Results of a National Survey,” Health Affairs, Vol. 26 No. 5, September/October 2007, pp. 13731383. n Most off-the-shelf EHR systems, however, do not support population management systems well. Even the most sophisticated implementations, such as Kaiser Permanente’s Health Connect and the Computerized Patient Record System (CPRS) used by the Veterans Health Administration, rely on separate population management systems used in parallel with their EHR. However, some EHR purchasers (including clinic networks) have worked closely with EHR vendors to customize their systems to offer some of the needed functionality. However, this customization work is very time intensive and requires significant expertise. There is no single right solution—there are only tools to help improve clinical care. The most sophisticated systems in use today include both EHR and CDMS functions. The more successful implementations of both systems require change management techniques and the inclusion of all members of the care team (including administrative staff ) to help smooth the way. Some people prefer to use stepping stones to cross a river, others prefer to jump in and swim. Either way, they are more likely to successfully get to the other side by working together as a team and having a plan for how to get there. California HealthCare Foundation | 1438 Webster Street, Suite 400, Oakland, CA 94612 | tel: 510.238.1040 | fax: 510.238.1388 | www.chcf.org