Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
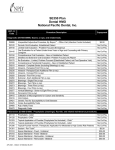
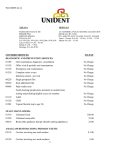
SE450 Plan Dental HMO National Pacific Dental, Inc. CDT-11 Procedure Description Code Diagnostic (D0100-D0999): Exams; x-rays; and related tests. 2 D9999 Unspecified Adjunctive Procedure, By Report - Office Visit (Infection Control Included) D0120 Periodic Oral Evaluation -Established Patient D0140 Limited Oral Evaluation - Problem Focused (Emergency) Oral Evaluation for a Patient Under three Years of Age and Counseling with Primary D0145 Caregiver D0150 Comprehensive Oral Evaluation - New or Established Patient D0160 Detailed and Extensive Oral Evaluation -Problem Focused, By Report D0170 Re-Evaluation - Limited, Problem Focused (Established Patient; not Post-Operative Visit) D0180 Comprehensive Periodontal Evaluation - New or Established Patient D0210 Intraoral - Complete Series (Including Bitewings) (x-ray) D0220 Intraoral - Periapical First Film (x-ray) D0230 Intraoral - Periapical Each Additional Film (x-ray) D0240 Intraoral - Occlusal Film (x-ray) D0250 Extraoral - First Film (x-ray) D0260 Extraoral - Each Additional Film (x-ray) D0270 Bitewings - Single Film (x-ray) D0272 Bitewings - Two Films (x-ray) D0273 Bitewings - Three Films (x-ray) D0274 Bitewings - Four Films (x-ray) D0277 Vertical Bitewings - Seven to Eight Films (x-ray) D0330 Panoramic Film (x-ray) D0415 Collection of Microorganisms for Culture and Sensitivity D0416 Viral Culture D0421 Genetic Test for Susceptibility to Oral Diseases D0425 Caries Susceptibility Tests D0460 Pulp Vitality Tests D0470 Diagnostic Casts Preventive (D1000-D1999): Prophylaxis (cleanings); fluoride; and related maintenance procedures. D1110 Prophylaxis - Adult 1 D1120 Prophylaxis -Child 1 D1203 Topical Application of Fluoride (Prophylaxis Not Included) - Child D1204 Topical Application of Fluoride (Prophylaxis Not Included) - Adult Topical Fluoride Varnish; Therapeutic Application for Moderate to High Caries Risk D1206 Patients 1 D1351 Sealant - Per Tooth D1510 Space Maintainer - Fixed - Unilateral D1515 Space Maintainer - Fixed - Bilateral D1520 Space Maintainer - Removable - Unilateral D1525 Space Maintainer - Removable - Bilateral 275-5354 - D0420 / D1000430 10-2011 Copayment $5.00 No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay No Co-Pay $5.00 $45.00 $45.00 $45.00 $45.00 1 CDT-11 Procedure Description Copayment Code D1550 Re-cementation of Space Maintainer $11.00 D1555 Removal of Fixed Space Maintainer $11.00 Restorative (D2000-D2999): Amalgams, resins, pins, and single crowns: includes polishing; bases; pulp caps; liners; and preparation, temporization and cementation of cast restorations; and cast crowns. D2140 Amalgam - One Surface, Primary or Permanent $10.00 D2150 Amalgam - Two Surfaces, Primary or Permanent $12.00 D2160 Amalgam - Three Surfaces, Primary or Permanent $15.00 D2161 Amalgam - Four or More Surfaces, Primary or Permanent $15.00 D2330 Resin-Based Composite - One Surface, Anterior $10.00 D2331 Resin-Based Composite - Two Surfaces, Anterior $12.00 D2332 Resin-Based Composite - Three Surfaces, Anterior $15.00 D2335 Resin-Based Composite -Four or More Surfaces, or Involving Incisal Angle (Anterior) $60.00 D2390 Resin-Based Composite Crown, Anterior $25.00 D2391 Resin-Based Composite - One Surface, Posterior $40.00 D2392 Resin-Based Composite - Two Surfaces, Posterior $60.00 D2393 Resin-Based Composite - Three Surfaces, Posterior $80.00 D2394 Resin-Based Composite - Four or More Surfaces, Posterior $80.00 3 D2750 Crown - Porcelain Fused to High Noble Metal $230.00 D2751 Crown - Porcelain Fused to Predominantly Base Metal $230.00 3 D2752 Crown - Porcelain Fused to Noble Metal $230.00 3 D2780 Crown - 3/4 Cast High Noble Metal $230.00 D2781 Crown - 3/4 Cast Predominantly Base Metal $230.00 3 D2782 Crown - 3/4 Cast Noble Metal $230.00 3 D2790 Crown - Full Cast High Noble Metal $230.00 D2791 Crown - Full Cast Predominantly Base Metal $230.00 3 D2792 Crown - Full Cast Noble Metal $230.00 3 D2794 Crown - Titanium $230.00 D2910 Re-Cement Inlay, Onlay, or Partial Coverage Restoration $12.00 D2915 Re-Cement Cast or Prefabricated Post and Core $12.00 D2920 Re-Cement Crown $12.00 1 D2930 Prefabricated Stainless Steel Crown - Primary Tooth $48.00 1 D2931 Prefabricated Stainless Steel Crown - Permanent Tooth $48.00 1 D2934 Prefabricated Esthetic Coated Stainless Steel Crown -Primary Tooth $48.00 D2940 Protective Restoration $5.00 D2950 Core Build-Up, Including Any Pins $30.00 D2951 Pin Retention - Per Tooth, in Addition to Restoration $30.00 D2952 Cast Post and Core In Addition to Crown -Indirectly Fabricated $50.00 D2953 Each Additional Indirectly Fabricated Post - Same Tooth $15.00 D2954 Prefabricated Post and Core in Addition to Crown $50.00 D2955 Post Removal (Not in Conjunction with Endodontic Therapy) $15.00 D2957 Each Additional Prefabricated Post - Same Tooth $12.00 D2970 Temporary Crown (Fractured Tooth) $54.00 Endodontics (D3000-D3999): Pulp caps; root canals; apical surgery; retrogrades; hemisections and related procedures. D3110 Pulp Cap - Direct (Excluding Final Restoration) $12.00 D3120 Pulp Cap - Indirect (Excluding Final Restoration) No Co-Pay Therapeutic Pulpotomy (Excluding Final Restoration) -Removal of Pulp Coronal to the D3220 $20.00 Dentinocemental Junction and Application of Medicament D3221 No Co-Pay Pulpal Debridment, Primary and Permanent Tooth 275-5354 - D0420 / D1000430 10-2011 2 CDT-11 Code Procedure Description Copayment D3222 D3230 Partial Pulpotomy (w/ inc. root development) $20.00 $20.00 Pulpal Therapy (Resorbable Filling) - Anterior, Primary Tooth (Excluding Final Restoration) Pulpal Therapy (Resorbable Filling) - Posterior, Primary Tooth (Excluding Final D3240 $20.00 Restoration) D3310 Root Canal Therapy - Anterior (Excluding Final Restoration) $95.00 D3320 Root Canal Therapy - Bicuspid (Excluding Final Restoration) $118.00 D3330 Root Canal Therapy - Molar (Excluding Final Restoration) $162.00 D3410 Apicoectomy/Periradicular Surgery - Anterior $80.00 D3421 Apicoectomy/Periradicular Surgery - Bicuspid (First Root) $80.00 D3425 Apicoectomy/Periradicular Surgery - Molar (First Root) $80.00 D3426 Apicoectomy/Periradicular Surgery (Each Additional Root) $80.00 D3430 Retrograde Filling - Per Root $20.00 Periodontics (D4000-D4999): Includes root planing/curettage; gingival and osseous surgery; and related procedures; includes pre-op and post-op evaluations and local anesthetic; charting must be performed in conjunction with these procedures. Gingivectomy or Gingivoplasty - Four or More Contiguous Teeth or Bounded Teeth D4210 $95.00 Spaces, Per Quadrant Gingivectomy or Gingivolplasty - One to Three Contiguous Teeth or Bounded Teeth D4211 $64.00 Spaces, Per Quadrant Gingival Flap Procedure, Including Root Planing - Four or More Contiguous Teeth or $150.00 Bounded Teeth Spaces, Per Quadrant Gingival Flap Procedure, Including Root Planing - One to Three Contiguous Teeth or D4241 $100.00 Bounded Teeth Spaces, Per Quadrant Osseous Surgery (Including Flap Entry and Closure) - Four or More Contiguous Teeth or D4260 $195.00 Bounded Teeth Spaces, Per Quadrant Osseous Surgery (Including Flap Entry and Closure) - One to Three Contiguous Teeth or D4261 $130.00 Bounded Teeth Spaces, Per Quadrant D4341 Periodontal Scaling and Root Planing -Four or More Teeth, Per Quadrant $35.00 D4342 Periodontal Scaling and Root Planing, One to Three Teeth, Per Quadrant $24.00 D4355 Full Mouth Debridement to Enable Comprehensive Evaluation and Diagnosis $30.00 D4910 Periodontal Maintenance $24.00 Prosthodontics, Removable (D5000-D5899): Full and partial dentures; includes fabrication and/or repair of prosthesis and routine post-delivery care. D5110 Complete Denture - Maxillary $260.00 D5120 Complete Denture - Mandibular $260.00 D5130 Immediate Denture - Maxillary $300.00 D5140 Immediate Denture - Mandibular $300.00 Maxillary Partial Denture - Resin Base (Including Any Conventional Clasps, Rests, and D5211 $275.00 Teeth) Mandibular Partial Denture - Resin Base (Including Any Conventional Clasps, Rests, and D5212 $275.00 Teeth) Maxillary Partial Denture - Cast Metal Framework with Resin Base (Including Any D5213 $300.00 Conventional Clasps, Rests, and Teeth) Mandibular Partial Denture - Cast Metal Framework with Resin Base (Including Any D5214 $300.00 Conventional Clasps, Rests, and Teeth) D5410 Adjust Complete Denture - Maxillary $10.00 D5411 Adjust Complete Denture - Mandibular $10.00 D5421 Adjust Partial Denture - Maxillary $10.00 D5422 Adjust Partial Denture - Mandibular $10.00 D5510 Repair Broken Complete Denture Base $25.00 D4240 275-5354 - D0420 / D1000430 10-2011 3 CDT-11 Procedure Description Code D5520 Replace Missing or Broken Teeth - Complete Denture (Each Tooth) D5610 Repair Resin (Partial) Denture Base D5620 Repair Cast (Partial Denture) Framework D5630 Repair or Replace Broken Clasp (Partial Denture) D5640 Replace Broken Teeth (Partial Denture) - Per Tooth D5650 Add Tooth to Existing Partial Denture D5660 Add Clasp to Existing Partial Denture D5670 Replace All Teeth and Acrylic on Cast Metal (Partial) Framework (Maxillary) D5671 Replace All Teeth and Acrylic on Cast Metal (Partial) Framework (Mandibular) D5710 Rebase Complete Maxillary Denture D5711 Rebase Complete Mandibular Denture D5720 Rebase Maxillary Partial Denture D5721 Rebase Mandibular Partial Denture D5730 Reline Complete Maxillary Denture (Chairside) D5731 Reline Complete Mandibular Denture (Chairside) D5740 Reline Maxillary Partial Denture (Chairside) D5741 Reline Mandibular Partial Denture (Chairside) D5750 Reline Complete Maxillary Denture (Laboratory) D5751 Reline Complete Mandibular Denture (Laboratory) D5760 Reline Maxillary Partial Denture (Laboratory) D5761 Reline Mandibular Partial Denture (Laboratory) D5820 Interim Partial Denture (Maxillary) D5821 Interim Partial Denture (Mandibular) D5850 Tissue Conditioning (Maxillary) D5851 Tissue Conditioning (Mandibular) Prosthodontics, Fixed (D6200-D6999): Abutments; pontics and related procedures. Includes diagnosis/models; preparation, temporization, fabrication and cementation of final restoration. 3 D6210 Pontic - Cast High Noble Metal D6211 Pontic - Cast Predominantly Base Metal 3 D6212 Pontic - Cast Noble Metal 3 D6214 Pontic - Titanium 3 D6240 Pontic - Porcelain Fused to High Noble Metal D6241 Pontic - Porcelain Fused to Predominantly Base Metal 3 D6242 Pontic - Porcelain Fused to Noble Metal 3 D6250 Pontic - Resin with High Noble Metal D6251 Pontic - Resin with Predominantly Base Metal 3 D6252 Pontic - Resin with Noble Metal 3 D6720 Crown - Resin with High Noble Metal D6721 Crown - Resin with Predominantly Base Metal 3 D6722 Crown - Resin with Noble Metal 3 D6750 Crown - Porcelain Fused to High Noble Metal D6751 Crown - Porcelain Fused to Predominantly Base Metal 3 D6752 Crown - Porcelain Fused to Noble Metal 3 D6780 Crown - 3/4 Cast High Noble Metal D6781 Crown - 3/4 Cast Predominantly Base Metal 3 D6782 Crown - 3/4 Cast Noble Metal 3 D6790 Crown - Full Cast High Noble Metal D6791 Crown - Full Cast Predominantly Base Metal 275-5354 - D0420 / D1000430 10-2011 Copayment $19.00 $25.00 $25.00 $25.00 $19.00 $25.00 $35.00 $248.00 $248.00 $65.00 $65.00 $65.00 $65.00 $25.00 $25.00 $25.00 $25.00 $65.00 $65.00 $65.00 $65.00 $45.00 $45.00 $25.00 $25.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 $230.00 4 CDT-11 Code Procedure Description Copayment 3 D6792 Crown - Full Cast Noble Metal $230.00 3 D6794 Crown - Titanium $230.00 D6930 Re-Cement Fixed Partial Denture No Co-Pay D6940 Stress Breaker $35.00 D6970 Post and Core in Addition to Fixed Partial Denture Retainer - Indirectly Fabricated $35.00 D6972 Prefabricated Post and Core in Addition to Fixed Partial Denture Retainer $35.00 D6973 Core Build-Up for Retainer, Including any Pins $30.00 D6980 Fixed Partial Denture Repair, By Report $45.00 Oral Surgery (D7000-D7999): Nonsurgical and surgical extractions (including sutures, if necessary) and related procedures; includes pre-op and post-op evaluations and treatment under local anesthetic. D7111 Extraction, Coronal Remnants, Deciduous Tooth $10.00 D7140 Extraction, Erupted Tooth or Exposed Root (Elevation and/or Forceps Removal) $10.00 Surgical Removal of Erupted Tooth Requiring Elevation of Mucoperiosteal Flap and D7210 $20.00 Removal of Bone and/or Section of Tooth D7220 Removal of Impacted Tooth - Soft Tissue $30.00 D7230 Removal of Impacted Tooth - Partially Bony $50.00 D7240 Removal of Impacted Tooth - Completely Bony $75.00 D7241 Removal of Impacted Tooth - Completely Bony, with Unusual Surgical Complications $75.00 D7250 Surgical Removal of Residual Tooth Roots (Cutting Procedure) $30.00 D7270 Tooth Reimplantation and/or Stabilization Of Accidentally Evulsed or Displaced Tooth $50.00 D7280 Surgical Access of an Unerupted Tooth $50.00 Alveoloplasty in Conjunction with Extractions - Four or More Teeth or Tooth Spaces, Per D7310 $36.00 Quadrant Alveoloplasty in Conjunction with Extractions - One to Three Teeth or Tooth Spaces, Per D7311 $24.00 Quadrant Alveoloplasty Not in Conjunction with Extractions - Four or More Teeth or Tooth Spaces, D7320 $36.00 Per Quadrant Alveoloplasty Not in Conjunction with Extractions - One to Three Teeth or Tooth Spaces, D7321 $24.00 Per Quadrant D7510 Incision and Drainage of Abscess - Intraoral Soft Tissue $26.00 D7520 Incision and Drainage of Abscess - Extraoral Soft Tissue $26.00 D7910 Suture of Recent Small Wounds up to 5 cm No Co-Pay Frenulectomy – Also Knowna as Frenectomy or Frenotomy – Separate Procedure not D7960 $60.00 Incidental to Another Procedure Orthodontics (D8000-D8999): Orthodontic treatment; related procedures to improve a patient's craniofacial dysfunction and/or dentofacial deformity. D8050 Interceptive Orthodontic Treatment of the Primary Dentition (Phase 1) 4 $1,200.00 D8060 Interceptive Orthodontic Treatment (Primary/Transitional Dentition) (Phase 1) 4 $1,200.00 D8070 Comprehensive Orthodontic Treatment of the Transitional Dentition (24 Month Case) $2,100.00 D8080 Comprehensive Orthodontic Treatment of the Adolescent Dentition (24 Month Case) $2,100.00 D8090 Comprehensive Orthodontic Treatment of the Adult Dentition (24 Month Case) $2,200.00 D8210 Removable Appliance Therapy $560.00 D8220 Fixed Appliance Therapy $560.00 D8660 Pre-Orthodontic Treatment Visit (Orthodontic Consultation) $120.00 Periodic Orthodontic Treatment (In Conjunction With Comprehensive Orthodontic D8670 No Co-Pay Treatment) Orthodontic Retention - Per Arch (Removal of Appliances, Construction and Placement of D8680 $95.00 Retainers (s) D8999 2 Unspecified Orthodontic Procedure, By Report Diagnostic Workup 275-5354 - D0420 / D1000430 10-2011 $250.00 5 CDT-11 Code Procedure Description Premium Transparent Brackets (Per Arch) Adjunctive General Services (D9110-D9999): D9110 Palliative (Emergency) Treatment of Dental Pain - Minor Procedure D9120 Fixed Partial Denture Sectioning D9211 Regional Block Anesthesia D9212 Trigeminal Division Block Anesthesia D9215 Local Anesthesia D9230 Analgesia, Anxiolysis, Inhalation of Nitrous Oxide Consultation (Diagnostic Service Provided by Dentist or Physician Other than Requesting Dentist or Physician Office Visit-Observation (During office hours) Office Visit - After Regularly Scheduled Hours Case Presentation, Detailed and Extensive Treatment Planning D9310 D9430 D9440 D9450 1 2 3 Copayment $200.00 No Co-Pay $45.00 No Co-Pay No Co-Pay No Co-Pay $10.00 No Co-Pay No Co-Pay $35.00 No Co-Pay For children age 14 and under only Other than those procedures listed, no other unspecified procedures are covered Does not include the cost of noble metal, high noble metal, or titanium To be covered, all services and procedures must be considered dentally necessary by your Primary Care Dentist. Your Selected General Dentist may encounter situations that require the services of a dentist who limits his/her practice to specialty care. Your Selected General Dentist will provide you with a Specialty Referral Form outlining what procedures need to be performed or evaluated by a Specialist. Specialty care requires prior authorization by us. Please Call 800-232-0990 For All Specialty Care Referrals The above procedures are performed as needed and deemed necessary by your attending Panel Dentist - subject to applicable Limitations, Exclusions and Governing Administrative Policies of the Program. Please refer to these sections for further clarification of benefits. (See Limitations and Exclusions) 275-5354 - D0420 / D1000430 10-2011 6 Limitations and Exclusions Below are the limitations that are applicable to this Plan: 1. Crowns, bridges and dentures (including immediate dentures) are not to be replaced within a five- year period from initial placement and only if it is unsatisfactory and cannot be made satisfactory by reline or repair; 2. Partial dentures are not to be replaced within any five-year period from initial placement, unless necessary due to natural tooth loss where the addition or replacement of teeth to the existing partial is not feasible; 3. Denture relines are limited to one per denture during any 12 consecutive months; 4. Treatment is generally limited to conventional techniques and does not include hemisection, implants, over-dentures and grafting; 5. The plan allows a treatment plan up to five units of crown or bridgework per arch. Upon the sixth unit, the Plan considers the treatment to be full-mouth reconstruction. The patient is responsible for fees incurred for anything beyond the fifth unit at usual and customary fees; 6. Periodontal treatments (root planing/subgingival curettage) are limited to four quadrants during any 12 consecutive months; 7. A full mouth x-ray is defined as a minimum of 6 periapical films plus bitewing x-rays or panorex plus bitewing x-rays on the same date of service; 8. Sealants: Plan benefit applies to primary and permanent molar teeth, within four (4) years of eruption, unless medically necessary;; 9. Single unit cast metal and/or ceramic restorations and crowns are covered only when the tooth cannot be adequately restored with other restorative materials. Crown build-ups including pins are only allowable as a separate procedure in the exceptional instance where extensive tooth structure is lost and the need for a substructure can be demonstrated by written report and x-rays; 10. Cosmetic dental care is limited to composite restorations on posterior teeth, if a listed benefit, when a Plan dentist determines treatment to be appropriate dental care. All other cosmetic procedures are excluded from coverage. The following dental procedures and services are not included in the Plan: 1. Hospital or ambulatory facility administered dental services; general anesthesia; intravenous and inhalation sedation; services of a special anesthesiologist; prescription drugs or other related hospital or ambulatory facility fees; 2. Dental conditions arising out of and due to enrollee’s employment or for which Worker’s Compensation is payable. Services that are provided to the enrollee by state government or agency thereof, or are provided without cost to the enrollee by any municipality, county or other subdivision; 3. Treatment required by reason of war; 4. Treatment of fractures and dislocations; 5. Loss or theft of fixed and removable prosthetics (crowns, bridges, full or partial dentures); 6. Dental expenses incurred in connection with any dental procedures started after termination of eligibility for coverage; 7. Any service that is not specifically listed as a covered expense; 8. Procedures, appliances or restorations to replace developmentally missing teeth or other developmental conditions; developmental malformations (including but not limited to cleft palate, enamel hypoplasia, fluorosis, jaw malformations, anodontia) and the removal/replacement of supernumerary teeth; 9. Treatment/removal of malignancies, cysts over 1.25 centimeters, tumors or neoplasms; 10. Dispensing of drugs/medications in a dental office; 11. Treatment as a result of accidental injury. Accidental injury is defined as damage to the hard and soft tissues of the oral cavity resulting from external forces to the mouth; 12. Cases which in the professional opinion of two (2) of our attending dentists, or our Dental Director, determine that a satisfactory result cannot be obtained or where the prognosis is poor or guarded. Such decision is an adverse determination, which can be appealed. See your EOC for your appeal options; 13. Dental services received from any dental office other than our contracted dental office, unless expressly authorized in writing by us or as cited under “Emergency Dental Services”’ 14. Elective procedures, including but not limited to the removal of impacted asymptomatic teeth, extractions for orthodontic purposes, surgical orthodontic procedures and crown exposure; 15. Implant placement or removal, appliances placed on or services associated with implants, including but not limited to prophylaxis and periodontal treatment; 16. Crown lengthening procedures; 17. Replacement of long standing missing tooth or teeth (usually 5 years or more) in an otherwise stable dentition; 18. Dental Services and treatments for restoring tooth structure loss from wear, bruxism, attrition and/or erosion; changing or restoring vertical dimension; and full-mouth reconstruction to enhance occlusion; diagnosis and/or treatment of the temporomandibular joint (TMJ); 275-5354 - D0420 / D1000430 10-2011 7 19. Dental services not performed in our general practice dental office because of physical, medical or behavioral limitations of eligible dependents/members over the age of eight years. This exclusion shall not apply to an enrollee who is unable to undergo dental treatment in a office setting or undergo local anesthesia due to a documented physical, mental, or medical reason as determined by the enrollee’s physician or the dentist providing dental care. Orthodontic Exclusions and Limitations (if a covered benefit under your plan) I. Orthodontic treatment must be provided by one of our contracting dentists II. Plan benefits shall cover 24 months of usual and customary orthodontic treatment and an additional 24 months of retention. Treatment extending beyond such time periods will be subject to a per-office-visit charge. III. The following are not included as orthodontic benefits: 1. repair or replacement of lost or broken appliances 2. re-treatment of orthodontic cases 3. changes in treatment necessitated by an accident 4. treatment involving: a. maxillo-facial surgery, myofunctional therapy, cleft palate, micrognathia, macroglossia b. surgically exposing impact teeth (i.e. maxillary cuspids) c. hormonal imbalances or other factors affecting growth or developmental disturbances d. treatment related to temporomandibular joint disorders e. lingually placed direct bonded appliances and arch wires (“invisible braces”) f. functional appliances that are used in conjunction with fixed appliances IV. The retention phase of treatment shall include the construction, placement, and adjustment of retainers. Complete plan information may be found in the Evidence of Coverage form # TX-EOC 09 2009 (PL) or contract # TX-GC2008 (PL) 275-5354 - D0420 / D1000430 10-2011 8