Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
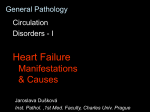
Hypoperfusion and Shock Hypoperfusion Common problem Extent makes resuscitation difficult Shock due to hypoperfusion Start fluid resuscitation as soon as possible © 2009 NAEMT Overview Describe differences between compensated and uncompensated shock Review differences of distributive, non-distributive and obstructive shock Explore pathophysiology for different etiologies of shock Discuss interventions for early and late shock © 2009 NAEMT Physiology BP = Cardiac Output x Systemic Resistance Cardiac Output = Stroke Volume x Heart Rate After-load = Resistance to blood being ejected Pre-load = Blood returned to heart Starling’s Law = Amount of cardiac muscle stretch LifeART NHTSA © 2009 NAEMT Shock Compensation Children vs. Adults Children Increased heart rate Vasoconstriction Prolonged compensation Rapid decompensation Adults Increased stroke volume Vasoconstriction Tachycardia Slow, but sustained compensation EPS411.com © 2009 NAEMT Categories of Shock Non-Distributive Hypovolemic Hemorrhagic Metabolic © 2009 NAEMT Categories of Shock Distributive Anaphylaxis Septic Neurogenic © 2009 NAEMT Categories of Shock Obstructive Pulmonary embolus Tension pneumothorax Cardiac tamponade © 2009 NAEMT Etiologies of Hypoperfusion (Common) Emesis and diarrhea Osmotic diuresis from diabetes Internal or external blood loss Plasma loss from sepsis or anaphylaxis © 2009 NAEMT Etiologies of Hypoperfusion (Uncommon) Spinal cord injury Cardiac failure Medications required to restore perfusion © 2009 NAEMT Severity of Hypoperfusion Compensated Volume Compensated Decompensated Signs are due to inadequate tissue perfusion Compensated shock is reversible with fluids Time © 2009 NAEMT Severity of Hypoperfusion Compensated Shock Signs Compensated Decompensated Volume Pulse Breathing Blood Pressure AVPU Altered Mental Status Time © 2009 NAEMT Severity of Hypoperfusion Compensated Shock Signs Compensated Decompensated Weak or absent peripheral pulses, weak central pulses Volume Weak peripheral pulses, strong central pulses EPS411.com Time © 2009 NAEMT Severity of Hypoperfusion Dehydration Testing Hypovolemic patient’s skin will “tent” © 2009 NAEMT Severity of Hypoperfusion Decompensated Shock Compensated Decompensated Volume Inadequate tissue perfusion to all organs Body is unable to continue compensation Time © 2009 NAEMT Severity of Hypoperfusion Decompensated Shock Signs Compensated Decompensated Volume Pulse Breathing Blood Pressure AVPU V Altered Mental Status P U Weak or absent peripheral pulses, weak central pulses Time © 2009 NAEMT Severity of Hypoperfusion Decompensated Shock Signs © 2009 NAEMT Assessment © 2009 NAEMT Scene Survey Hazards to you, your partner, the patient and bystanders © 2009 NAEMT First Impression Pediatric Assessment Triangle Compensated or decompensated EPS411.com © 2009 NAEMT First Impression General Appearance Observe interactions Not sick - attentive to environment, focus on familiar people and objects, alert for threats Good brain function requires adequate oxygenation, ventilation, cerebral perfusion Sick - does not care you are present or recognize parents © 2009 NAEMT First Impression General Appearance Muscle tone Spontaneous movements Skin color Other signs of distress KyleDavidBates.com © 2009 NAEMT First Impression Work of Breathing © 2009 NAEMT First Impression Circulation to the Skin Skin color, capillary refill, distal vs. central pulses © 2009 NAEMT First Impression Sick Rapid Initial Assessment Not Sick Yes Significant MOI? No Appropriate Interventions Relationship Transport Priority Involve Family Transport Method Detailed History Transport Destination Focused Physical Exam © 2009 NAEMT Initial Assessment Airway Loss of airway may occur in decompensated shock Identify and treat life threats © 2009 NAEMT Initial Assessment Breathing Assess for chest trauma Abnormal sounds Rate effort and volume Administer O2 and treat cause © 2009 NAEMT Initial Assessment Circulation Compensated Weak peripheral pulses, strong central pulses Decompensated Weak or absent peripheral pulses, weak central pulses EPS411.com EPS411.com © 2009 NAEMT Initial Assessment Circulation Management – Intravenous Fluid bolus if any signs of shock Early recognition of hypoperfusion and fluid resuscitation are key Select a large bore catheter Location close to central circulation Two IVs may be needed © 2009 NAEMT Initial Assessment Circulation Management – Intraosseous Can be used on any age child © 2009 NAEMT Intraosseous Space Blood Flow © 2009 NAEMT Anatomy Neonate Leg Cross Section Skin Intraosseous Catheter Tibia Lateral Compartment Fibula Subcutaneous Fat Anterior Compartment Posterior Compartment © 2009 NAEMT Other Issues IO Insertion Depth based on patient size and weight Gently insert catheter Advance catheter slowly Feel needle drop into medullary space Frequently monitor insertion site and extremity Need hands-on training © 2009 NAEMT IO Insertion Anatomical Landmarks Patella Tibial Tuberosity Medial Tibia © 2009 NAEMT IO Insertion Unable to Palpate Tibial Tuberosity Finger Width Finger Width Often difficult or impossible to palpate © 2009 NAEMT IO Insertion Able to Palpate Tibial Tuberoisty Finger Width © 2009 NAEMT Anatomy Neonate Leg Cross Section Traditional IO Catheter Tibia Fibula Left Leg © 2009 NAEMT Anatomy 11 y.o. Tibia Cross Section Tibia Fibula Left Leg © 2009 NAEMT Pain Somatic and Visceral © 2009 NAEMT Initial Assessment Circulation Management – Crystalloids 20 mL/kg, < 20 minutes Reassess patient after each fluid bolus © 2009 NAEMT Initial Assessment Never Administer D5W D5W can lead to hyperglycemia © 2009 NAEMT Initial Assessment Circulation Management – Medications Sepsis Pressers and antibiotics Cardiogenic Shock Pressers, furosemide, morphine and antiarrhythmics Anaphylaxis Epinephrine, diphenhydramine, Solu-Medrol EPS411.com © 2009 NAEMT Initial Assessment Circulation Management – Medications Use medications after fluid boluses EPS411.com © 2009 NAEMT Transport Decision Rapid transport for pediatric shock patients © 2009 NAEMT Focused History Questions to Determine Type of Shock Bleeding Vomiting Diarrhea Fluid intake / urine output Fever Anaphylaxis signs FEMA Photo Library / Andrea Boomer © 2009 NAEMT Head to Toe Physical Exam Done En Route © 2009 NAEMT Ongoing Assessment Done Frequently © 2009 NAEMT Summary Recognition and rapid intervention are keys to treatment Pulse quality and level of consciousness are key indicators Obtain IV or IO access if shock treatment is needed Deliver crystalloid fluids at 20 mL/kg © 2009 NAEMT