Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Normal and abnormal clavicle: image review
Poster No.:
P-0085
Congress:
ESSR 2015
Type:
Educational Poster
Authors:
A. O' Brien , A. levai , T. Simelane , N. Ramesh ; Dublin/IE,
1
2
1
2 1
2
PORTLAOISE/IE
Keywords:
Anatomy, Bones, Musculoskeletal bone, Conventional
radiography, CT, Education, Normal variants, Acute, Arthritides,
Metastases
DOI:
10.1594/essr2015/P-0085
Any information contained in this pdf file is automatically generated from digital material
submitted to EPOS by third parties in the form of scientific presentations. References
to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in
any way constitute or imply ECR's endorsement, sponsorship or recommendation of the
third party, information, product or service. ECR is not responsible for the content of
these pages and does not make any representations regarding the content or accuracy
of material in this file.
As per copyright regulations, any unauthorised use of the material or parts thereof as
well as commercial reproduction or multiple distribution by any traditional or electronically
based reproduction/publication method ist strictly prohibited.
You agree to defend, indemnify, and hold ECR harmless from and against any and all
claims, damages, costs, and expenses, including attorneys' fees, arising from or related
to your use of these pages.
Please note: Links to movies, ppt slideshows and any other multimedia files are not
available in the pdf version of presentations.
www.essr.org
Page 1 of 20
Learning objectives
The purpose of this poster is provide an illustrative guide to the changes seen in the
clavicle and the uniqueness of this long bone
Background
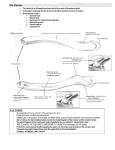
The clavicle {collar bone} is an 'S' shape bone, the medial aspect is convex, and the
lateral aspect concave. Divided into a sternal end, a shaft and an acromial end.
Sternal (medial) End
The sternal end articulates with the manubrium of the sternum at the sternoclavicular
joint - an articular disc with a large facet; it is marked by a rough oval depression for the
costoclavicular ligament
Shaft
The lateral one-third and medial two-third;
The lateral one third is more flattened and thinner consisting of two borders, the anterior
and posterior, two surfaces, the superior and inferior. The anterior border is concave
forwards and deltoid muscle originates at this end. The posterior border is convex
backwards and has the attachment of the trapezius muscle. The inferior border the
conoid tubercle and the trapezoid ridge which gives attachment to the medial part of the
coracoclavicular ligament{ the conoid ligament} and the lateral part of the coracoclavicular
ligament{ the trapezoid ligament}
The medial two thirds is circular and thicker consists of 4 surfaces. The anterior surface
is convex forwards and has the origin of the pectoralis major; the posterior surface is
concave backwards and has the origin of sternohyoid muscle; the superior surface; the
inferior surface has the subclavian groove with attachment of the subclavius muscle.
The shaft of the clavicle acts a point of origin and attachment for several muscles - deltoid,
trapezuis, subclavius, pectoralis major, sternocleidomastoid and sternohyoid
Acromial (lateral) End
Page 2 of 20
The acromial end has a small facet for articulation {incomplete articular disc} with the
acromion of the scapula at the acromioclaviclar joint, with attachment for two ligaments:
Conoid tubercle - attachment point of the conoid ligament, the medial part of the
coracoclavicular ligament
Trapezoid ridge - attachment point of the trapezoid ligament, the lateral part of the
coracoclavicular ligament.
UNUSUAL FEATURES OF CLAVICLE
1.
2.
3.
4.
5.
6.
7.
8.
9.
th
First bone to ossify in foetus{5-6 week}
Only long with 2 primary centres of ossification
Only bone that ossifies in membrane{ not cartilage}
Only long bone in the body that lies horizontally
Has no medullary cavity
Subcutaneous along its entire length
Commonest bone amongst the 206 bones in the human body to fracture
One of the only long bone that does not require routine two orthogonal views
One of the easiest bones that can be assessed clinically.
Imaging findings OR Procedure Details
RADIOGRAPHY: OF THE CLAVICLE
Radiograph of the clavicle it is desirable to perform a Postero- Anterio {PA},as the
clavicle is close to the image reader to give optimum skeletal detail. It also reduces the
radiation dose to the eyes and thyroid.
The entire length of the clavicle should be included on the image, the lateral end of the
clavicle clearly demonstrated with no foreshortening of the clavicle
Alternate radiography include Anterio-Posterior view { AP} if patient immobile;
Angulated {15-30 degrees} inferio-superior view may be useful in demonstrating certain
fractures.
Companion shadow is a term used to describe the appearance of a smooth,
homogenous, density{ skin and subcutaneous fat } with a well-defined stripe that runs
Page 3 of 20
parallel to the clavicle , not seen in every radiographs and can mimic periosteal reaction
or other pathology
Though non traumatic lesions are more common in lateral third of clavicle, some of the
lesions like Freidrich`s disease, condensing osteitis, sternocostoclavicular hyper ostosis
are quiet common at the medial end.
Table:
Congenital/developmental
Birth Fracture
Congenital Defects of Clavicle
Congenital Pseudoarthrosis of Clavicle
Cleidocranial dysplasia
Short Clavicle syndrome
Metabolic / Endocrine disorders
Hyper Parathyroidism
Hyper vitaminosis A, D
Inflammatory
Infantile Cortical Hyperostosis
Infective-Bacterial Osteomyelitis
Non suppurative Periostistis (CRMO, SAPHO, SCCH)
Spondyloarthropathy-Rheumatoid arthritis,
Recurrent Trauma / Overuse syndromes
Anterior Subluxation of sterno clavicular joint
Distal Osteolysis of the clavicle
Osteitis
Idiopathic
Friedrich`s Disease
Neoplastic: Primary: Ewing's tumour Secondary: Metastatic lesions: lung, breast,
thyroid
Fractures of the clavicle are common, up to 10% of all fractures. The mechanism
of injury is usually medium to high energy falling on an outstrecthed arm, in direct
impact sports. Fractures are commonest at the junction of the middle third and lateral
third, the weakest point of the clavicle. Traditionally, these fractures are management
conservatively. Occasionally, though internal fixation may be necessary { in malunion or
non union, reduced function }.Birth fractures account for 0.5-0.9% of normal deliveries,
Page 4 of 20
usually they are associated with difficult delivery, Some of the children may have brachial
plexus injuries. They heal without any residual problems.
Cleidocranial dysplasia, an autosomal dominant disorder,occurs in approximately 1
per million individuals worldwide. Individuals with cleidocranial dysplasia usually have
underdeveloped or absent clavicles, only the medial part of the bone is absent, in 10%
cases, they are totally absent.
Caffey's Disease: {infantile cortical hyperostosis} an autosomal dominant disorder
where in there is excessive new bone formation -hyperostosis is a bone disorder that
most often occurs in babies. Changes are noted in the clavicle, including other bonesmandible, scapulae, mandible, long bones. Occurring in approximately 3/1000 infants, it
is a self limiting disease, with changes not seen over the age of two months.
EROSIONS LATERAL END OF THE CLAVICLE
Bilateral: Hyperparathyroidism ; rheumatoid arthritis; scleroderma
Unilateral: Trauma, metastatic, myeloma, osteomyelitis
Images for this section:
Page 5 of 20
Fig. 1
Page 6 of 20
Fig. 2: TABLE 1
Page 7 of 20
Fig. 3
Page 8 of 20
Fig. 4
Page 9 of 20
Fig. 5
Page 10 of 20
Fig. 6
Page 11 of 20
Fig. 7
Page 12 of 20
Fig. 8
Page 13 of 20
Fig. 9
Page 14 of 20
Fig. 10
Page 15 of 20
Fig. 12
Page 16 of 20
Fig. 11
Page 17 of 20
Fig. 13
Page 18 of 20
Conclusion
A large number of pathologies involve the clavicles, often seen on Chest Radiographs.
Pathological changes seen are either infective, benign {erosions secondary to systemic
disorders} or primary or secondary malignant involvement. Some of these can often be
subtle and missed on Chest radiographs, or changes seen in the clavicle may point to
the underlying systemic disorders.
References
1. Gray, Henry. Anatomy of the Human Body; Philadelphia: Lea & Febiger, 1918;
Bartleby.com, 2000. www.bartleby.com/107/. [Date of Printout]
2. Clark's Positioning in Radiography 12Ed
A. Stewart Whitley, Charles Sloane, Graham Hoadley, Adrian D. Moore
CRC Press, 26 Aug 2005
3. E. Roos, M. Maas, S. J. M. Breugem, G. R. Schaap, and J. A. M. Bramer, "Nonbacterial
Osteitis of the Clavicle: Longitudinal Imaging Series from Initial Diagnosis to Clinical
Improvement," Case Reports in Rheumatology, vol. 2015, Article ID 182731, 4 pages,
2015. doi:10.1155/2015/182731
4. Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint
Surg Am. Feb 2009;91(2):447-60. [Medline].
Personal Information
AMY O BRIEN
ANDREA LEVAI
THABISILE SIMELANE
Page 19 of 20
NAGABATHULA RAMESH
MIDLAND REGIONAL HOSPITAL, PORTLAOISE, IRELAND
Page 20 of 20