Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
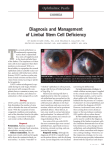
Taiwan Journal of Ophthalmology 4 (2014) 97e99 Contents lists available at ScienceDirect Taiwan Journal of Ophthalmology journal homepage: www.e-tjo.com Case report Post-chemotherapy bilateral limbal stem cell deficiency Yen-Wen Hsieh a, Jiunn-Liang Chen a, b, c, *, Shwu-Jiuan Sheu a, c, Jyh-Seng Wang d a Department of Ophthalmology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan Chung Hwa University of Medical Technology, Tainan, Taiwan c National Yang-Ming University School of Medicine, Taipei, Taiwan d Department of Pathology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan b a r t i c l e i n f o a b s t r a c t Article history: Received 9 July 2013 Received in revised form 14 August 2013 Accepted 29 August 2013 Available online 25 October 2013 We report an extremely rare case of bilateral total limbal stem cell deficiency (LSCD) induced by longterm systemic chemotherapy for squamous cell carcinoma of the lung, and the outcomes of bilateral keratolimbal allograft transplantation (KLAT) in such a case. A 34-year-old male patient had underlying disease of squamous cell carcinoma in the right upper lung with extensive mediastinum and lymph node metastasis and received a series of systemic chemotherapy, including a combination of vinorelbine and cisplatin and a combination of gemcitabine, cisplatin, and docetaxel. According to clinical manifestations of ocular surface disorder, pathology findings, and immunostaining of cytokeratin 13 (CK13), LSCD secondary to systemic chemotherapy was diagnosed. KLAT was performed in both eyes. Although graft rejection developed in the right eye, complete re-epithelialization with favorable visual acuity occurred in the left eye 3 years after limbal transplantation. Copyright Ó 2013, The Ophthalmologic Society of Taiwan. Published by Elsevier Taiwan LLC. All rights reserved. Keywords: keratolimbal allograft transplantation limbal stem cell deficiency systemic chemotherapy 1. Introduction Corneal limbus is well known as an area containing stem cells that are important as a regenerative source of corneal epithelial cells. In addition, the limbus acts as a barrier between the cornea and the conjunctival epithelium. Limbal stem cell deficiency (LSCD) may lead to failure in the maintenance of the regenerative capacity of corneal epithelial cells and lead to replacement of corneal epithelial cells by the invading conjunctival epithelium. The clinical features of corneal diseases with LSCD include conjunctivalization of cornea, poor corneal epithelialization, persistent epithelial defects, corneal scarring, chronic inflammation, corneal vascularization, and fibrous ingrowth.1e3 LSCD may occur in two major clinical settings. It may be caused by destruction of the limbal stem cell population [chemical or thermal injuries, ocular cicatricial pemphigoid (OCP), StevenJohnson syndrome, contact lens-related trauma, severe microbial infection, and iatrogenic causes such as repeated surgeries or cryotherapies]; or dysfunction of the stromal microenvironment of limbal stem cells (aniridia, ectodermal dysfunction, chronic Conflicts of interest: The authors have no conflicts of interest relevant to this article. * Corresponding author. Department of Ophthalmology, Kaohsiung Veterans General Hospital, 386, Ta-Chung First Road, Kaohsiung 813, Taiwan, ROC. E-mail address: [email protected] (J.-L. Chen). limbitis, peripheral ulcerative keratitis, and idiopathic keratopathy). Topical cytotoxic agents such as 5-fluorouracil and mitomycin C have been reported to delay corneal epithelialization and induce LSCD when applied locally.4,5 Yet LSCD secondary to systemic chemotherapy has seldom been reported. To date, two cases of LSCD related to hydroxycarbamide6,7 have been reported in the literature. However, LSCD arising from combination systemic chemotherapy has never been reported. Herein we report such an extremely rare case. 2. Case report A 34-year-old man visited our hospital in May 2009 due to progressive blurred vision in both eyes for 1 year. The patient was a victim of right upper lung squamous cell carcinoma with extensive mediastinum and lymph node metastasis. He had received a series of chemotherapy regimens of cisplatin combined with vinorelbine, cisplatin combined with gemcitabine and docetaxel from November 2007 to October 2008. He denied any history of ocular trauma or surgery. Six months after chemotherapy, he complained of decreased visual acuity with pain, severe photophobia, itching, and redness in both eyes. He received treatment from his local general practitioner, but in vain. At the initial visit, his best corrected visual acuity was 6/15 in the right eye and 6/60 in the left eye. Slit lamp biomicroscopy revealed bilateral multiple irregular whitish-gray opacifications on the corneal surface, and the lesions 2211-5056/$ e see front matter Copyright Ó 2013, The Ophthalmologic Society of Taiwan. Published by Elsevier Taiwan LLC. All rights reserved. http://dx.doi.org/10.1016/j.tjo.2013.08.003 98 Y.-W. Hsieh et al. / Taiwan Journal of Ophthalmology 4 (2014) 97e99 Fig. 1. Preoperative pictures showed an advanced ocular surface disorder in the chronic inflammation phase with raised whitish-gray opacifications (arrows) above the corneal surface, marked 360-degree corneal vascularization (arrowheads) with vessel extending 4e5 mm from the limbus into the center of the cornea in the right eye (A) and 1e2 mm in the left eye (B). were localized between subepithelial and anterior stroma. In spite of topical lubricants and anti-inflammatory medications, increasing central corneal opacity with surrounding engorged hyperemic vessels and 360-degree superficial and deep corneal vascularization towards the corneal center developed in both eyes 2 years later (Fig. 1). He also experienced secondary glaucoma and recurrent central corneal ulceration. His visual acuity had deteriorated to counting fingers in the right eye and to 3/60 in the left eye. Under the impression of LSCD, limbal stem cell transplantation was done to restore the ocular surface before lamellar corneal transplantation. The procedure included keratolimbal allograft transplantation (KLAT) from a cadaver donor following superficial keratectomy and fine needle cauterization of stromal neo-vascularization in both eyes (the left eye in June 2011 and the right eye in November 2011). Systemic cyclosporine A (IVAX, Opava, Czech) and Prednisolone VPP (Taiwan Veterans Pharmaceutical, Taoyuan County, Taiwan) were given for immunosuppression after the surgeries. The final visual acuity was 6/20 with complete corneal re-epithelialization in the left eye but poor corneal re-epithelialization in the right eye due to severe rejection. Corneal pathology disclosed marked thinning of the corneal epithelium, focal absence of Bowman’s layer, moderate B-cell and T-cell lymphocytes, and neutrophil infiltration in the left eye (Fig. 2A). The pathologic picture of the limbus revealed few goblet cells, T-lymphocyte infiltration with CD3 immunostaining (Fig. 2C), B-lymphocyte infiltration with CD20 immunostaining (Fig. 2D), fibrosis, and neovascularization in the subepithelial tissue of the left eye (Fig. 2B). In addition, the presence of positive cytokeratin 13 (CK13) squamous epithelium overlying the corneal stroma of the right eye supported the diagnosis of LSCD (Fig. 2E). OCP was less favored because conjunctiva pathology revealed rare CD117positive mast cells (Fig. 3A), few CD68-positive macrophages (Fig. 3B), and the negative finding of linear deposition of immunoglobulin G (IgG) along the epithelial basement membrane zone by direct immunofluorescence (DIF) (Fig. 3C). 3. Discussion The diagnosis of LSCD has long relied on clinical features such as replacement of the corneal epithelium with conjunctiva, chronic inflammation, poor corneal epithelial healing, and stromal corneal Fig. 2. (A) The sections of the specimen showed a picture of corneal tissue with marked thinning epithelium and focal absence of Bowman’s layer (arrow) and aggregation of lymphocytes composed of both B-cells and T-cells and neutrophils in the subepithelial tissue (arrowheads). (B) The sections of the limbal tissue specimen exhibited the presence of moderate lymphocyte infiltration (arrow) composed of both T-cells and B-cells with CD3 immunostaining [in (C), arrow] and CD20 immunostaining [in (D), arrow], fibrosis, and neovascularization (arrowhead) in the subepithelial tissue. (E) The immunohistochemistry stain of cornea reveals the presence of CK13-positive squamous epithelium (arrow) overlying corneal stroma. (A: H&E 200; B: H&E 100; E: 100). CK13 ¼ cytokeratin 13; H&E ¼ hematoxylin and eosin. Y.-W. Hsieh et al. / Taiwan Journal of Ophthalmology 4 (2014) 97e99 99 Fig. 3. (A) A rare CD117-positive mast cell (400). (B) A few CD68-positive macrophages (400). (C) The negative finding of linear deposition of IgG (arrows) along the epithelial basement membrane zone by DIF (400). DIF ¼ direct immunofluorescence; IgG ¼ immunoglobulin G. scarring. The invasion of goblet cells in the cornea under impression cytology could also confirm the diagnosis.8 Identification of surface marker would facilitate the diagnosis of LSCD. Poli et al developed a validated and reliable technique by immunocytochemical detection of highly specific conjunctival and corneal cytokeratins for diagnosis of LSCD,9 in which it was shown that CK12 is specific for corneal differentiation whereas CK13 is specific for conjunctival differentiation. In our case, the presence of positive CK13 squamous epithelium overlying corneal stroma confirmed the diagnosis of LSCD. OCP was ruled out by conjunctival biopsy plus a DIF test of IgG. Based on the history and clinical findings, we speculated that chemotherapy is the cause of LSCD in our case. In Ellies’ report, LSCD might be reversible after cessation of hydroxycarbamide.6 However, our case could not change the regimen of chemotherapy as the combination was the only responding one for him. Although limbal graft failure occurred in his right eye, the worse eye, a favorable outcome was obtained in his left eye. Compared to the previous two case reports of LSCD following single chemotherapy, our case had been exposed to multiple chemotherapy including vinorelbine, cisplatin, gemcitabine, and docetaxel. Chemotherapy drugs can affect only dividing cells (cell cyclespecific) or cells at rest (cell cycle-nonspecific). Vinorelbine and docetaxel inhibit the microtubule structures and ultimately result in cell death. Gemcitabine is known as the family of drugs called antimetabolites, which are very similar to normal substances and are incorporated into cellular metabolism to make the cell cycle cease. Cisplatin is classified as an alkylating agent, which is most active in the resting phase. These cytotoxic agents with the essential propensity of targeting rapidly dividing cells may contribute to the induction of stem cell damage, including that of the cornea. Even so, surgical treatment is still possible to offer benefit. The management of ocular surface disorders, particularly complete LSCD, has always been a challenging condition for ophthalmologists. Generally, the treatment depends on the extent of LSCD whether it is partial, total, unilateral, or bilateral. In partial LSCD with the visual axis involved and decreased vision, the conjunctivalized epithelium covering the cornea is removed to allow the remaining intact limbal epithelium to reconstruct the corneal surface. In total LSCD, limbal stem cell transplantation is the only available treatment of LSCD, for instance autograft (from the contralateral eye)10 in unilateral cases or allograft11 (from a living related donor or a cadaver donor) transplantation can harvest healthy limbal stem cells to the damaged eye. In allograft transplantation, systemic immunosuppression is required to diminish the risk of graft rejection and maintain the survival of the limbal transplant. Recently, with the increased knowledge on stem cell biology, cultured limbal stem cells represent another source of cells for subsequent transplantation to repair the LSCD disorder.12 Our case demonstrated a linkage between systemic chemotherapy and bilateral progressive LSCD, which was rarely reported. The pathogenesis might be due to stem cell failure due to chemical injury or a deficit in the stem cell niche.13 Chemotherapy can induce systemic and local side effects, such as hematopoietic stem cell impairment. Lucas et al demonstrated that cisplatin-induced neuropathy in the bone marrow may prevent hematopoietic regeneration in an animal study.14 However, the underlying mechanisms of chemotherapy-induced stem cell suppression remain unresolved. Clinically, we monitor blood cell count to evaluate the severity of the hematopoietic stem cell impairment. After systemic administration of chemotherapy, we monitor the drug toxicity levels in the aqueous and tear films, which reflect the LSCD. However, this ocular drug level is hard to detect based on the current technique. In our case, clinical manifestation and pathologic evidence (including positive CK13) support the diagnosis of LSCD. With the increasing number of people receiving systemic chemotherapy for a variety of diseases, we recommend detailed history investigation in all cases of idiopathic corneal epitheliopathy characterized by progressive LSCD. Once drug toxicity is suspected, cessation or modification of the toxic agent should be considered. References 1. Dua HS, Azuara-Blanco A. Limbal stem cells of the corneal epithelium. Surv Ophthalmol. 2000;44:415e425. 2. Dua HS, Joseph A, Shanmuganathan VA, Jones RE. Stem cell differentiation and the effects of deficiency. Eye (Lond). 2003;17:877e885. 3. Dua HS, Saini JS, Azuara-Blanco A, Gupta P. Limbal stem cell deficiency: concept, aetiology, clinical presentation, diagnosis and management. Indian J Ophthalmol. 2000;48:83e92. 4. Pires RT, Chokshi A, Tseng SC. Amniotic membrane transplantation or conjunctival limbal autograft for limbal stem cell deficiency induced by 5fluorouracil in glaucoma surgeries. Cornea. 2000;19:284e287. 5. Dudney BW, Malecha MA. Limbal stem cell deficiency following topical mitomycin C treatment of conjunctival-corneal intraepithelial neoplasia. Am J Ophthalmol. 2004;137:950e951. 6. Ellies P, Anderson DF, Topuhami A, Tseng SC. Limbal stem cell deficiency arising from systemic chemotherapy. Br J Ophthalmol. 2001;85:373e374. 7. Ding X, Bishop RJ, Herzlich AA, Patel M, Chan CC. Limbal stem cell deficiency from systemic chemotherapy with hydroxycarbamide. Cornea. 2009;28:221e223. 8. Puangsricharern V, Tseng SC. Cytologic evidence of corneal diseases with limbal stem cell deficiency. Ophthalmology. 1995;102:1476e1485. 9. Poli M, Janin H, Justin V, Auxenfans C, Burillon C, Damour O. Keratin 13 immunostaining in corneal impression cytology for the diagnosis of limbal stem cell deficiency. Invest Ophthalmol Vis Sci. 2011;52:9411e9415. 10. Dua HS, Azuara-Blanco A. Autologous limbal transplantation in patients with unilateral corneal stem cell deficiency. Br J Ophthalmol. 2000;84:273e278. 11. Dua HS, Azuara-Blanco A. Allo-limbal transplantation in patients with limbal stem cell deficiency. Br J Ophthalmol. 1999;83:414e419. 12. Rama P, Matuska S, Paganoni G, Spinelli A, De Luca M, Pellegrini G. Limbal stem-cell therapy and long-term corneal regeneration. N Engl J Med. 2010;363: 147e155. 13. Ramaesh K, Ramaesh T, Dutton GN, Dhillon B. Evolving concepts on the pathogenic mechanisms of aniridia related keratopathy. Int J Biochem Cell Biol. 2005;37:547e557. 14. Lucas D, Scheiermann C, Chow A, Kunisaki Y, Bruns I, Barrick C, et al. Nat Med. 2013;19:695e703.