Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
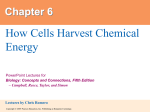
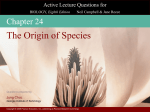
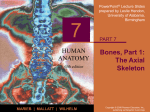
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Angular Movement Increase or decrease the angle between 2 bones. Include: Flexion — bending movement along the sagittal plane that decreases the angle of the joint and brings the articular bones closer together Extension — (reverse of flexion) bending movement along the sagittal plane that increases the angle of the joint and brings the articular bones further apart Hyperextension – bending beyond upright (or normal) extension Dorsiflexion (toes up) and plantar flexion (pointing toes) of foot Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Angular Movement Abduction — (moving away) movement of limb away from the midline / or median plane of body along the frontal plane Adduction — (moving toward) movement of a limb toward the body midline Circumduction — moving a limb so that it describes a cone in space Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Angular Movement Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 8.5b Angular Movement Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 8.5c, d Angular Movement Dorsi and Plantar Flexion Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 8.5e, f Now, somebody describe walking in the proper anatomically language of angular movement, e.g. “ Walking involves the…” Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Rotation Turning a bone along its own long axis E.g. 1st two cervical vertebrae E.g. hip and shoulder joints Medial rotation: toward median plane Lateral rotation: away from median plane Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Rotation The turning of a bone around its own long axis Examples Between first two vertebrae Hip and shoulder joints Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 8.5g Special Movements Supination and pronation: Supination: (turning backwards) e.g. palm up or forward (or palm superiorly or anteriorly Pronation: (turning forwards) e.g. palm down or back (or palm inferior or posterior) Eg. For supination/pronation is the radius and ulna Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Special Movements Inversion and eversion: e.g. the foot Inversion: the sole of the foot moves medially Eversion: the sole of the foot moves laterally Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Special Movements Protraction and retraction: e.g. the jaw Nonangular anterior (protraction) and posterior (retraction) movements in a transverse plane Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Special Movements Elevation and depression: Elevation: lifting a body part superiorly E.g. scapulae are “elevated” when you shrug your shoulders Depression: lifting a body part inferiorly E.g. chewing: mandible alternates between elevation and depression Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Special Movements Opposition: e.g. oppostion of the thumb and fingers Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Types of Synovial Joints Six major categories: Plane Hinge Pivot Condyloid Saddle Ball & socket Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Plane Joint Articular surfaces are essentially flat Allow only slipping or gliding movements Only examples of nonaxial joints E.g. intercarpal/intertarsal joints E.g. vertebral articular processes Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Types of Synovial Joints Hinge joints Cylindrical projections of one bone fits into a trough-shaped surface on another Motion is along a single plane (like a mechanical hinge) Uniaxial joints permit flexion and extension only Examples: elbow and interphalangeal joints Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Pivot Joints Rounded end of one bone protrudes into a “sleeve,” or ring, composed of bone (and possibly ligaments) of another uniaxial rotation of one bone around its own long axis Examples: “No” motion of the head via joint between the atlas and axis, and the proximal radioulnar joint (radius rotates within ring-like ligament secured to the ulna Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Condyloid or Ellipsoidal Joints Oval articular surface of one bone fits into a complementary depression in another Both articular surfaces are oval Biaxial joints permit all angular motions Examples: radiocarpal (wrist) joints, and metacarpophalangeal (knuckle) joints Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Saddle Joints Similar to condyloid joints but allow greater movement Each articular surface has both a concave and a convex surface Example: carpometacarpal joint of the thumb Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Ball-and-Socket Joints A spherical or hemispherical head of one bone articulates with a cuplike socket of another Multiaxial joints permit the most freely moving synovial joints Examples: shoulder and hip joints Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Selected Synovial Joints We’ll look at five selected synovial joints: Knee Shoulder Hip Elbow Temporomandibular (jaw) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Knee Largest and most complex joint of the body Allows flexion, extension, but very little rotation Three joints in one surrounded by a single joint cavity Intermediate: Femoropatellar joint. Between the patella and distal end of the femur Lateral and medial tibiofemoral joints: between the femoral condyles above and c-shaped menisci (semilunar cartilage) of the tibia below (lateral & medial joints) Acts as a hinge. Permits flexing and extension Bicondylar joint Some rotation when the knee is flexed The joint cavity is only partially enclosed by a capsule Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Knee Ligaments and Tendons – Anterior View Anteriorly, 3 ligaments run from the patella to the tibia: Patellar ligament Medial patellar retinaculum Lateral patellar retinaculum All 3 are continuous with the quadriceps muscle tendon There are many bursae associated with the knee The ligaments of the knee: Capsular & extracapsular ligaments act to prevent hyperextension of the knee and are stretched tight when the knee is extended Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 8.8c Synovial Joints: Knee Ligaments and Tendons – Anterior View Tendon of the quadriceps (rectus) femoris muscle Fibular and tibial collateral ligaments (extracapsular): Run from the medial epicondyle of the femur to the medial condyle of the tibia and fuse to the medial meniscus Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Knee – Other Supporting Structures Intracapsular ligaments: Prevent anterior/posterior displacement of the articular surfaces & secure bones when standing Anterior cruciate ligament: Attaches to the anterior intercondylar area of the tibia, passes posteriorly, laterally, and superiorly to attach to the femur on the medial side of its lateral condyle Prevents forward sliding of the tibia on the femur Checks hyperextension of the knee Is tight when the knee is extended Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Knee – Other Supporting Structures Posterior cruciate ligament: Attached to the posterior intercondylar area of the tibia and passes anteriorly, ,medially, and superiorly to attach to the lateral side of the medial femural condyle Functions in preventing backward displacement of the tibia or forward sliding of the femur Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Knee – Other Supporting Structures Medial meniscus & lateral meniscus (semilunar cartilage) The menisci are two pads of cartilagenous tissue which serve to disperse friction in the knee joint between the lower leg (tibia) and the thigh (femur). They are shaped concave on the top and flat on the bottom, articulating the tibia. They are attached to the fossae between the condyles of the tibia (intercondyloid fossa), and towards the center they are unattached and their shape narrows to a thin shelf Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Knee – Locking the knee The lateral femural condyle stops rolling before the medial condyle causing the femur to rotate medially on the tibia until all the major ligaments of the knee are tight and the menisci are compressed The popliteus muscle rotates the femur and “unlocks” the knee Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Elbow Hinge joint that allows flexion and extension only Hinge joint formed by the trochlea of the humerus being “gripped” by the ulna’s trochlear notch The articular capsule is thin and allows freedom to flex and extend Side to side movements are restricted by: Ulnar collateral ligament (medially) Radial collateral ligament (laterally) The biceps and triceps provide some stability Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Shoulder (Glenohumeral) Ball-and-socket joint in which stability is sacrificed to obtain most freely moving joint of the body Head of humerus articulates with the glenoid cavity of the scapula The glenoid cavity contributes little to joint stability Glenoid labrum: the rim of fibrocartilage that helps support the joint Ligaments are located on the anterior aspect The coracohumeral ligament: Superiorly located & provides only a strong thickening of the capsule Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Shoulder Stability Weak stability is maintained by: Thin, loose joint capsule Muscle tendons that cross the shoulder joint contribute most to this joint’s stability Four ligaments – coracohumeral, and three glenohumeral Tendon of the long head of biceps, which travels through the intertubercular groove and secures the humerus to the glenoid cavity Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Rotator Cuff Rotator cuff (four tendons and associated muscles) that encircles the shoulder joint and blends with the articular capsule The muscles are: Subscapularis Supraspinatus Infraspinatus Teres minor Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Hip (Coxal) Joint Ball-and-socket joint Formed by the articulation of the spherical head of the femur with the acetabulum of the coxal Acetabulum labrum: Fibrocartilage that enhances the depth of the acetabulum Ligaments that reinforce the capsule of the hip joint: Iliofemoral ligament (anteriorly) Pubofemoral ligament (inferiorly) Ischiofemural ligament (posteriorly) Ligamentum teres: the ligament of the head of the femur Intracapsular Contains artery to the head of the femur Thus, the socket and ligaments contribute most to the stability of the hip joint but limit its range of motion Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Synovial Joints: Hip Stability Acetabular labrum Iliofemoral ligament Pubofemoral ligament Ischiofemoral ligament Ligamentum teres Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 8.12a Synovial Joints: Hip Stability Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 8.12c, d Temporomandibular Joint (TMJ) Lies just anterior to the ear Mandibular condyle articulate with the inferior surface of the temporal bone Articular surface of the temporal bone: Posteriorly: concave mandibular fossa Anteriorly: convex articular tubercle The lateral aspects of the joint are strengthened by a lateral ligament Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Temporomandibular Joint (TMJ) Three types of movement Hinge – depression and elevation of mandible Side to side – (lateral excursion) grinding of teeth Anterior movement of the superior disc and superior mandibular condyle (when mouth is wide open…like during a yawn…but please don’t yawn now…you did didn’t you) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Sprains The ligaments reinforcing a joint are stretched or torn These injuries are slow to heal due to poor vascularization Completely torn ligaments require prompt surgical repair. Inflammation in the joint will break down neighboring tissues If damaged beyond repair, substitute or grafted ligaments are used Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Cartilage Injuries Mostly tearing of the knee’s menisci Avascular: can not repair itself Loose bodies (cartilage fragments) can interfere with joint function by binding or locking the joint Removal of part of the meniscus makes the joint less stable… BUT, prevents more tearing as I have drawn and demonstrated on the board (reminder for me to draw something on the board) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Dislocations Occur when bones are forced out of alignment Usually accompanied by sprains, inflammation, and joint immobilization Caused by serious falls and are common sports injuries Subluxation – partial dislocation of a joint Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Inflammatory and Degenerative Conditions Bursitis An inflammation of a bursa, usually caused by a blow or friction Symptoms are pain and swelling Treated with anti-inflammatory drugs; excessive fluid may be aspirated Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Inflammatory and Degenerative Conditions Tendonitis Inflammation of tendon sheaths typically caused by overuse Symptoms and treatment are similar to bursitis Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Arthritis More than 100 different types of inflammatory or degenerative diseases that damage the joints Most widespread crippling disease in the U.S. Symptoms – pain, stiffness, and swelling of a joint Acute forms are caused by bacteria and are treated with antibiotics Chronic forms include osteoarthritis, rheumatoid arthritis, and gouty arthritis Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Osteoarthritis (OA) Most common chronic arthritis; often called “wear-and-tear” arthritis Affects women more than men 85% of all Americans develop OA More prevalent in the aged, and is probably related to the normal aging process Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Osteoarthritis: Course of disease OA reflects the years of abrasion and compression causing increased production of metalloproteinase enzymes that break down cartilage As one ages, cartilage is destroyed more quickly than it is replaced The exposed bone ends thicken, enlarge, form bone spurs, and restrict movement Joints most affected are the cervical and lumbar spine, fingers, knuckles, knees, and hips Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Osteoarthritis: Treatments OA is slow and irreversible Treatments include: Mild pain relievers, along with moderate activity Magnetic therapy Glucosamine sulfate decreases pain and inflammation Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Rheumatoid Arthritis (RA) Chronic, inflammatory, autoimmune disease of unknown cause, with an insidious onset Usually arises between the ages of 40 to 50, but may occur at any age Signs and symptoms include joint tenderness, anemia, osteoporosis, muscle atrophy, and cardiovascular problems The course of RA is marked with exacerbations and remissions Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Rheumatoid Arthritis: Course RA begins with synovitis of the affected joint Inflammatory chemicals are inappropriately released Inflammatory blood cells migrate to the joint, causing swelling Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Rheumatoid Arthritis: Course Inflamed synovial membrane thickens into a pannus Pannus erodes cartilage, scar tissue forms, articulating bone ends connect The end result, ankylosis, produces bent, deformed fingers Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Rheumatoid Arthritis: Treatment Conservative therapy – aspirin, long-term use of antibiotics, and physical therapy Progressive treatment – anti-inflammatory drugs or immunosuppressants The drug Enbrel, a biological response modifier, neutralizes the harmful properties of inflammatory chemicals Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Gouty Arthritis Deposition of uric acid crystals in joints and soft tissues, followed by an inflammation response Typically, gouty arthritis affects the joint at the base of the great toe In untreated gouty arthritis, the bone ends fuse and immobilize the joint Treatment – colchicine, nonsteroidal antiinflammatory drugs, and glucocorticoids Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Developmental Aspects of Joints By embryonic week 8, synovial joints resemble adult joints Few problems occur until late middle age Advancing years take their toll on joints: Ligaments and tendons weaken Intervertebral discs become more likely to herniate Most people in their 70s have some degree of OA Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Developmental Aspects of Joints Prudent exercise (especially swimming) that coaxes joints through their full range of motion is key to postponing joint problems Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings