Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
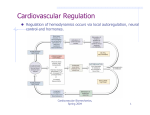
Cell Bio 19- Integrated Control of the CV System • • • • • • • • The cardiovascular system can be explained in terms of individual mechanisms of control – Powerful systemic mechanisms operate over both long and short-terms to regulate cardiac output and mean arterial pressure – Local mechanisms control blood flow in the microcirculation Together these mechanisms regulate the function of the cardiovascular system In attempting to understand the integrated response of the cardiovascular system to a stress, we must include in our analysis not only cardiovascular subsystems, but also pertinent control systems outside the circulation Integrated control of the cardiovascular system is best understood by considering three important circulatory “stresses” – Standing up (orthostasis), exercise, and hemorrhage Short-Term Regulation of Arterial Pressure Blood pressure is one of four vital signs that are considered key to assessing a patient’s well-being Access to blood flow—which any organ may need at a moment’s notice—is crucially tied to maintenance of a constant pressure head • A constant pressure head is achieved through tight control of mean arterial blood pressure (MAP) The short-term regulation of arterial pressure—on a scale of seconds to minutes—occurs through neural pathways and targets the heart, vessels, and adrenal medulla • The long-term regulation of arterial pressure—on a scale of hours to days—occurs through pathways that target blood vessels, but also the kidneys Moreover, the regulation of arterial pressure is also achieved by regulation of cardiac output Neural Reflexes • The neural reflex systems that regulate MAP operate as a series of negative feedback loops consisting of five main elements (Reflex arc) – A detector – Afferent neurons – Integration center – Efferent neurons – Effectors • A dual system of sensors and neural reflexes controls MAP (in the short-term) – The primary sensors are baroreceptors – The secondary sensors are chemoreceptors • These are primarily involved in ventilation Cell Bio 19- Integrated Control of the CV System Baroreceptors • Baroreceptors are mechanoreceptors that detect distension (stretch) of the vessel walls • There are two general types of baroreceptors – High pressure – Low pressure • Will discuss with regulation of cardiac output • High-pressure baroreceptors are located in two strategic, high pressure areas – The carotid sinus – The aortic arch • The receptors are coiled terminals of sensory fibers intermeshed in the elastic fibers of the vessel walls • The negative feedback loop established by the high-pressure baroreceptor reflex arc addresses two situations – Increased MAP causes vasodilation and bradycardia – Decreased MAP causes vasoconstriction and tachycardia Note that decreased MAP causes vasoconstriction and tachycardia • • The firing rate of the afferent baroreceptor nerves is proportionate to the amount of stretch detected in the vessel wall Baroreceptors have both a dynamic and static response – Baroreceptors are very sensitive to the rate of change of arterial blood pressure • The baroreceptors adapt to pressure signals – Hypertension? • The carotid receptors are generally much more sensitive than the aortic receptors Afferent Pathways • The pathway for carotid sinus baroreceptors is through the glossopharyngeal nerve (CN IX) via the carotid sinus nerve • The pathway for aortic sinus baroreceptors is through the depressor branch of the vagus nerve (CN X) Cell Bio 19- Integrated Control of the CV System • The entire complex of medullary nuclei involved in cardiovascular regulation is called the medullary cardiovascular center • Within this center, broad subdivisions can be distinguished – Cardioinhibitor and vasomotor areas • The cardiovascular center receives all important information from the baroreceptors and is the coordinating center for cardiovascular homeostasis • Most afferent fibers of the high-pressure baroreceptors (aortic or carotid) project to the bilateral nuclei of the solitary tract (part of the cardiovascular center) where they synapse onto two main types of interneurons – Inhibitory interneurons – Excitatory interneurons Efferent Pathways • A set of interneurons originating in the vasomotor area traverse the spinal cord and synapse on preganglionic sympathetic neurons in the thoracic spinal cord • By default these interneurons produce tonic output resulting in sympathetic activity, which promotes vasoconstriction – As well, sympathetic activity increases heart rate and contractility, and release of epinephrine from the adrenal medulla • Inhibitory interneurons project from the NTS onto the vasomotor area • Excitation of inhibitory interneurons—due to increased pressure detected by the baroreceptors— reduces sympathetic activity of the bulbospinal interneurons • The principal effect is thus vasodilation • This pathway largely accounts for the vascular component of the baroreceptor reflex • • Excitatory interneurons project from the NTS onto a cardioinhibitory area – Excitation of excitatory interneurons originating in the cardioinhibitory area increases parasympathetic activity to the heart—which is already strong—slowing heart rate This pathway accounts for the cardiac component of the baroreceptor reflex (bradycardia) Cell Bio 19- Integrated Control of the CV System • • The scenarios just discussed pertained to an increase in MAP In the case of a decrease in MAP (as in hemorrhage), decreased firing of the baroreceptor fibers leads to decreased activation of the interneurons – Sympathetic activity is increased – Parasympathetic activity is decreased Chemoreceptors • Chemoreceptors detect changes in blood PO2, PCO2, and pH—information used primarily to regulate ventilation, and secondarily to regulate blood pressure • There are two types of chemoreceptors – Peripheral chemoreceptors are located in bodies—clusters of highly-vascularized epithelial cells—along the arch of the aorta and at the bifurcation of the common carotid arteries – Central chemoreceptors are located in the medulla • The peripheral chemoreceptors are mainly sensitive to decreases in the partial pressure of oxygen (PO2) – This results in increased sympathetic outflow, causing vasoconstriction – Increased parasympathetic outflow also occurs, resulting in transient bradycardia • However, these chemoreceptors rapidly increase ventilation, which results in an increased heart rate • Central chemoreceptors of the medulla mainly sense low brain pH, which is usually a reflection of high arterial PCO2 • Activation of the central chemoreceptors, results in increased sympathetic output, and vasoconstriction – Increased blood pressure Cell Bio 19- Integrated Control of the CV System Regulation of Cardiac Output Recall that cardiac output is the product of heart rate and stroke volume Regulation of both of these factors occurs along two main lines – Mechanisms intrinsic to the heart – Mechanisms extrinsic to the heart • Other things being unchanged, an increased cardiac output raises MAP – The heart is an important effector organ in feedback loops regulating MAP Intrinsic Mechanisms • Heart rate is intrinsically determined by the nature of the action potential at the SA node, which itself is governed by ionic concentrations across cell membranes • Stroke volume is largely correlated with the force of ventricular contraction Extrinsic Mechanisms • Low-pressure baroreceptors are located in strategic, low pressure areas throughout the heart and most great vessels • Distension of these receptors depends mainly on venous return – They detect blood volume, and as such they help regulate cardiac output, and indirectly, MAP • • • There are two types of low-pressure atrial receptors, both joining the vagus nerve – A fibers monitor heart rate – B fibers monitor rising atrial volume Direct Effects • The afferent fibers of the low-pressure baroreceptors travel to various nuclei of the cardiovascular center – The overall response of effector organs is to reduce blood volume (and thus decrease pressure) • This is accomplished directly by an increase in heart rate, accompanied by vasodilation only in the kidneys, which increases dieresis Indirect Effects • There are also indirect effects resulting from the stretch of low-pressure baroreceptors – Stimulation of hypothalamus to inhibit secretion of antidiuretic hormone (ADH), which reduces water retention in the kidneys – Stretch of atrial myocytes causes secretion of atrial natriuretic peptide (ANP)—a vasodilator—which also enhances excretion of sodium in the kidneys Cell Bio 19- Integrated Control of the CV System • Examples of Integrated Control The following examples of integrated control—orthostasis, exercise, and hemorrhage—all involve a similar scenario – The cardiovascular system experiences a sudden challenge, and at minimum, an increase in blood pressure is required • The increase in blood pressure is mainly mediated by the heart and by the vasculature, with contributions from other organ systems Orthostasis • When one moves from a recumbent position to an erect posture, gravity, and high compliance of the veins rapidly lead to pooling of blood in the lower extremities – This pooling reduces venous return, which reduces cardiac output, and thus decreases mean arterial pressure • In the absence of properly functioning compensatory mechanisms, MAP can quickly fall low enough to compromise perfusion to the brain, and syncope can result – Orthostatic hypotension • The primary cardiovascular compensatory response to a sudden decrease in MAP is the baroreceptor reflex – Sympathetic outflow is increased – Parasympathetic outflow is decreased • The net effect is to raise MAP by rapidly targeting both the heart and blood vessels • Both inhibitory and excitatory interneurons are inhibited • • • • Under increased sympathetic outflow, widespread vasoconstriction occurs on both the arterial and venous sides – Arteriolar vasoconstriction results in increased total peripheral resistance, which increases MAP – Venoconstriction forces more blood back to the heart (increased venous return) and thus more blood to the arterial side, increasing MAP Heart rate and contractility increase immediately, which increases cardiac output, and thus mean arterial pressure – However, increased heart function must be accompanied by increased availability of blood—increased venous return—which results from venoconstriction An important compensation for blood pooling during orthostasis comes from skeletal muscle contraction Upon standing, muscles of the legs and abdomen tighten forcing blood upward to the heart – As with venoconstriction, this effect is dependent on one-way valves preventing the backflow of blood Cell Bio 19- Integrated Control of the CV System Exercise • The main goal in exercise is to increase blood flow to working muscles • Adaptation to exercise probably places the greatest demands on the circulation • Cardiac output may increase fivefold or more • Increased heart rate is about 2X as important as increased stroke volume in mediating the increase in CO • The cardiovascular response to exercise involves both a central command—from the CNS—and local responses in muscle Central Command • The anticipation of exercise initiates a central command originating in the cerebral cortex, and producing a twofold result – Increased sympathetic outflow to the heart and blood vessels – Decreased parasympathetic outflow to the heart Increased CO • Increased cardiac output results mainly from increased HR and contractility, which are mediated by increased sympathetic activity and decreased parasympathetic activity – Note that the increase in CO is essential as simply redirecting blood flow would be insufficient • An increase in cardiac output necessitates an increase in venous return, which occurs by essentially “squeezing” blood back to the heart – As in orthostasis, this is accomplished by venoconstriction and contraction of working muscles • Selective constriction in arteriolar beds redistributes flow to working muscle – Increased resistance in the skin, gut, kidneys, and inactive muscle causes reduction in blood flow • As body temperature increases, the skin experiences selective vasodilation – Vasoconstriction does not occur in coronary or cerebral circulations • Sympathetic vasoconstricting effects to working muscle are overridden by local effects • The increased activity of the working muscle produces metabolites—lactate, potassium, and adenosine—which promote vasodilation and hyperemia – This local vasodilation also decreases total peripheral resistance Cell Bio 19- Integrated Control of the CV System Hemorrhage • The initiating event in hemorrhage is blood loss • With a decreased blood volume, venous return to the heart is almost immediately decreased • According to the Frank-Starling mechanism, the decrease in venous return results in decreased cardiac output • Assuming that total peripheral resistance is initially unchanged, decreased cardiac output results in decreased MAP Compensatory Responses • Within a few hours following hemorrhage arterial pressure gradually rises back toward normal – Result of compensatory responses • In certain persons the compensatory responses fail, and arterial pressure falls • • RAAS • ADH • As in orthostasis, the baroreceptor reflex plays an important initial role in attempting to restore MAP Over a slightly longer term, arteriolar vasoconstriction resulting from the baroreceptor reflexes reduces blood flow into capillary beds, thus lowering CHP – Reabsorption is favored, and blood volume increases Decreased blood pressure resulting from hemorrhage causes activation of RAAS, and release of angiotensin II, which has two main effects – It causes arteriolar vasoconstriction, reinforcing the increase in total peripheral resistance – It stimulates secretion of aldosterone, which causes Na+ reabsorption in the kidneys, thus indirectly raising blood volume The low-pressure atrial baroreceptors mediate the release of anti-diuretic hormone, which has two effects – It promotes water reabsorption in the kidneys, helping to restore blood volume – It causes arteriolar vasoconstriction