Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
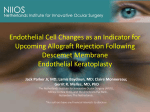
ARCH SOC ESP OFTALMOL 2009; 84: 237-244 ORIGINAL ARTICLE DESCEMET MEMBRANE ENDOTHELIAL KERATOPLASTY (DMEK): TWO-YEAR RESULTS QUERATOPLASTIA ENDOTELIAL DE MEMBRANA DE DESCEMET (DMEK): RESULTADOS A DOS AÑOS DAPENA I1, HAM L2, LIE J3, VAN-DER-WEES J3, MELLES GRJ4 ABSTRACT RESUMEN Purpose: To report the two-year results of Descemet membrane endothelial keratoplasty (DMEK) for managing corneal endothelial disorders. Methods: Non-randomized prospective clinical trial. A DMEK was performed in ten patients with Fuchs’ endothelial dystrophy or bullous keratopathy. A 3.5 mm clear corneal incision was made and «under air» DM was stripped off from the posterior stroma. A 9.0 mm diameter, organ cultured donor DM roll was inserted into a recipient anterior chamber, positioned into the posterior stroma and secured by completely filling the anterior chamber with air for 30 minutes. Results: Three eyes showed complete detachment of the tissue; this was managed by a secondary Descemet stripping endothelial keratoplasty procedure. The remaining seven eyes had a best corrected visual acuity of ≥ 0.7 in three eyes (43%) at one month, in five eyes (71%) at six months, and in six eyes (86%) at one and two years. At six months, the endothelial cell density averaged 2039 (±373) Objetivo: Describir los resultados, dos años después de realizar una queratoplastia endotelial de membrana de Descemet (DMEK: Descemet membrane endothelial keratoplasty), para el tratamiento de alteraciones del endotelio corneal. Métodos: Estudio clínico prospectivo no randomizado. En 10 pacientes con distrofia endotelial de Fuchs o queratopatía bullosa, se practicó una DMEK. A través de una incisión de 3,5 mm en córnea clara, la membrana de Descemet (MD) del receptor fue desprendida del estroma posterior en presencia de aire. Un disco de 9 mm de diámetro enrollado de MD donante preservada, fue insertado en la cámara anterior del receptor, posicionado en contacto con el estroma posterior corneal y asegurado en su posición mediante el llenado completo de la cámara anterior con aire durante 30 minutos. Resultados: Tres ojos mostraron un desprendimiento completo del tejido donante, por lo que fueron sometidos posteriormente a una queratoplastia endotelial con «pelado» de la MD (DSEK: Desce- Received: 15/10/08. Accepted: 24/4/09. Netherlands Institute for Innovative Ocular Surgery. Rotterdam. The Netherlands. 1 Graduate in Medicine. Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Holland. Melles Cornea Clinic Rotterdam, Rotterdam, Holland. 2 Graduate in Health Sciences. Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Holland. Melles Cornea Clinic Rotterdam, Rotterdam, Holland. 3 Graduate in Health Sciences. Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Holland. Amnitrans EyeBank Rotterdam, Rotterdam, Holland. 4 Graduate in Medicine. Ph.D. in Medicine. Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Holland. Melles Cornea Clinic Rotterdam, Rotterdam, Holland. Amnitrans EyeBank Rotterdam, Rotterdam, Holland. Correspondence: Gerrit R.J. Melles, MD, PhD Netherlands Institute for Innovative Ocular Surgery Laan Op Zuid, 88 3071 AA Rotterdam The Netherlands E-mail: [email protected] / [email protected] DAPENA I, et al. cells/mm2 (n=7), at one year 1925 (±267) cells/mm2 (n=7) and at two years 1730 (±400) cells/mm2 (n=6). Conclusions: DMEK may provide quick and nearly complete visual rehabilitation. Since the donor tissue can be stripped from donor corneoscleral rims, the procedure may be readily accessible to most corneal surgeons (Arch Soc Esp Oftalmol 2009; 84: 237-244). Key words: Descemet membrane endothelial keratoplasty (DMEK), posterior lamellar keratoplasty, corneal transplantation, Descemet membrane, endothelium, surgical technique. met stripping endothelial keratoplasty). En los siete ojos restantes, se observó una agudeza visual mejor corregida (AVMC) ≥ a 0,7 en 3 ojos (43%) en el primer mes, en 5 ojos (71%) a los seis meses, y en seis ojos (86%) al primer y segundo años. A los seis meses, la densidad celular endotelial media fue de 2039 (DS: 373) cél/mm2 (n=7), al año de 1925 (DS: 267 cél/mm2 (n=7) y a los 2 años de 1730 (DS: 400) cél/mm2 (n=6). Conclusión: DMEK podría proporcionar una recuperación rápida y casi completa de la visión. Debido a que el tejido donante puede ser obtenido a partir de anillos córneo-esclerales donantes, el procedimiento podría ser fácilmente accesible para la mayoría de los cirujanos corneales. Palabras clave: Queratoplastia endotelial de membrana de Descemet (DMEK), queratoplastia lamelar posterior, transplante corneal, membrana de Descemet, endotelio, técnica quirúrgica. INTRODUCTION In recent years we have described several posterior lamellar keratoplasty procedures which allowed the substitution of the corneal endothelium without incisions or sutures in the corneal surface for managing Fuchs’ endothelial dystrophy and aphakic or pseudophakic bullous keratopathy. In 1998 we described a technique in which a 7.5 mm diameter posterior lamellar disc without sutures could be transplanted through a 9.0 mm scleral incision with posterior suture (1-3). Since 2001, this technique became known in the United States as Deep Lamellar Endothelial Keratoplasty (DLEK) (4). In 2000 we described a variant of the previous technique that does not require sutures, in which a disc-shaped posterior transplant with a diameter of 9.0-9.5 mm was inserted through a 5.0 mm self-sealable tunnelized scleral incision and deployed in the anterior chamber (5). Since 2005, this technique has become known in the United States as «small incision DLEK» (6). In 2003, we described the insertion of a donor posterior disc folded in combination with a «descemetorrhesis» for removing the endothelial layer and its Descemet Membrane (DM) from the receptor (7,8). At present, this technique is known as Descemet’s stripping endothelial keratoplasty: DSEK) (9,10). 238 Even though the above techniques, designed and developed by our institute, demonstrated their feasibility for transplanting a donor posterior corneal disc without sutures, it could be expected that the selective DM and endothelium transplant would provide the best possible recovery of visual capacity in a corner with endothelial alteration (11-15). This study describes the clinical results after two years of an isolated DM transplant through a 3.5 mm self-sealing incision in a clear cornea, which could be termed «Descemet Membrane Endothelial Keratoplasty» (DMEK) (13-15). SUBJECTS, MATERIAL AND METHODS The DMEK was performed in four males and five females from 45 to 87 years of age with Fuchs’ endothelial dystrophy and/or bullous keratopathy (table I). All the patients signed an informed consent approved by the Institutional Review Board (IRB). Donor tissue In 10 donor ocular globes having less than 36 hours post mortem the corneal-scleral rings were ARCH SOC ESP OFTALMOL 2009; 84: 237-244 Transplante de membrana de Descemet Table I. Descemet Membrane Endothelial Keratoplasty (DMEK): 2-year results Patient Pre-surgery # Age Sex RE/ (years) LE 1 64 M LE 2 61 F 3 87 Surgery indication Concomitant disease BCVA Donor Surgery ECD (cel/) mm2 Complications Post-surgery BCVA BMC 1 m 6 m 12 m 24 m DCE Observations (cel/mm2) 6 m 12 m 24 m 0.3 2960 No 1.0 1.25 1.0 1.0 Adhered RE FED None (pseudophakic) PPBK None 1750 1678 1608 None FC 2630 Complicated graft insertion n.r. n.r. n.r. n.r. n.r. F LE PPBK 0.1 2460 No 0.25 0.4 0.4 n.d. Adhered 4 86 F RE Pupil fixed and RPE changes after complicated phako FED Superficial (pseudophakic) stromal scar 0.3 2640 Vitreous pressure n.r. n.r. n.r. n.r. n.r. 5 72 M RE FED Sub-epitelial central (pseudophakic) corneal scar 0.1 2660 Excentric donor pressure 0.5 0.6 0.7 0.7 6 60 M LE None 0.3 2470 No 1.0 1.0 1.0 1.0 7 76 F LE None 0.3 2520 No 0.6 0.8 1.0 0.9 Adhered 2180 2369 2289 None 8 59 9 74 M F RE LE None None 0.8 0.3 2480 2640 No No 1.0 1.0 0.6 0.7 1.0 0.8 1.0 1.0 Adhered Adhered 1790 1743 1476 None 2730 2098 2034 None 10 45 F RE FED (pseudophakic) FED (pseudophakic) BK eci (phakic) FED (pseudophakic) FED (phakic) Adhered; small paracentral DM roll Adhered 2270 2100 1800 None SEL 0.5 2640 Incomplete donor division n.r. n.r. n.r. n.r. n.r. n.r. n.r. n.r. 1760 1675 n.d. n.r. DSEK without complications 3 weeks after initial DMEK 1790 1812 1171 None n.r. n.r. DSEK without complications 2 weeks after initial DMEK None n.r. n.r. n.r. DSEK without complications 3 weeks after initial DMEK ARMD = Age-Related Macular Degeneration; DSEK = Descemet stripping endothelial keratoplasty; FC = Finger Counting; n.r. = Not relevant; BCVA = Best Corrected Visual Acuity (Snellen); ECD = Endothelial Cell Density; PPBK= Pseudo-Phakic Bullous Keratopathy; SEL = Systemic Erythematous Lupus; MD = Descemet Membrane; FED = Fuchs Endothelial Dystrophy; RPE = Retinal Pigmentary Epithelium; BMC = Biomicroscopy; BK eci = Bullous Keratopathy of unknown origin; m = Months; n.a. = Not available. extracted and stored in a minimally modified essential medium (MMEM) at 31ºC for organ culture. The mean age of donors was 71.3 years (SD: 6.1) and the mean cellular endothelial count of the tissue was 2614 (SD: 186) cel/mm 2 (Table). After two weeks in culture medium without dextrane and with antibiotics at 31 ºC the morphology and feasibility of the endothelial cells was assessed by means of inverted microscopy (Axiovert 40. Zeiss, Göttingen, Germany). Subsequently the corneal-scleral rings were assembled with the endothelial surface upwards upon a custom-designed vacuum holding instrument and the DM was detached from the posterior stroma using thin tweezers to obtain a 9.0 mm diameter endothelial single layer of DM. Due to the elastic properties of Descemet’s membrane it rolled up spontaneously to form what is known as a «Descemetroll», with the endothelium facing outwards. Each «Descemet-roll» was subsequently stored in a dextra- ne-free organ culture medium with antibiotics for a maximum period of one week awaiting transplant. Surgery An epithelial mark having a diameter of 9.0 mm was made in the recipient eyes to circumscribe the DM excision area. A 3.5 mm tunnelized incision was made in the limbus, penetrating the anterior chamber exactly at the limit of said mark. Utilizing a custom-made scraper (Melles scraper, D. O. R. C. International, Zuidland, The Netherlands) a circular portion of DM was removed from the posterior stroma in the presence of air, carrying out a «descemetorrhexis» of 9.0 mm diameter and removing from the eye the central portion thereof (7,8). The donor «Descemet-roll» was dyed with a 0.06% tryphan blue solution (VisionBlue™, D. O. ARCH SOC ESP OFTALMOL 2009; 84: 237-244 239 DAPENA I, et al. R. C. International) and inserted in a custom-made injector (Hippocratech, Rotterdam, The Netherlands) (11,12). Utilizing the injector, the donor «Descemet-roll» was inserted in the anterior chamber and carefully extended over the surface of the iris by indirect manipulation of the tissue with air and a balanced saline solution. Subsequently, an air bubble was injected under the donor DM to position it and maintain the tissue in contact with the recipient posterior stroma (11,12). The anterior chamber was completely filled with air for 30 minutes followed by an air-liquid replacement for pressurizing the eye. (SD: 373) cell/mm2 (n=7) and at the first and second year of 1925 (SD: 267) cell/mm2 (n=7) and 1730 (SD: 400) cell/mm2 respectively (fig. 1, Table I). Initially, it was difficult to visualize the transplant in the receiving eye. The confirmation that the transplant was in the right position was obtained observing its contour which showed a reflecting brilliance on the donor DM and by means of mirror microscopy which identified the paracentral endothelial donor cells. Some eyes exhibited small peripheral DM «tags», indicating the presence of DM micro-detachments or folds in the external limit of the transplant. With time, these peripheral tags stabilized and did not increase in size. Endothelial assessment DISCUSSION The cellular feasibility of the donor endothelial was assessed by means of inverted light microscopy (Axiovert 40. Zeiss, Göttingen, Germany), taking digital photographs (PixeLINK LP-A662, Zeiss, Göttingen, Germany) after administering 1.8% sucrose and dyeing with 0.04% blue tryphan (15-17). The endothelium of the patients was photographed and assessed utilizing a non-contact autofocus Topcon SP3000p mirror microscope (Topcon Corp, Tokyo, Japan). The images of the central cornea were manually analyzed and corrected, averaging three measurements of the endothelial cellular density (15-17,19,20). RESULTS The first day post-op all the donor DMs exhibited full adhesion to the posterior stroma of the receptor. One week after the operation, the Descemet transplant retained its position in seven of the eyes, but the three remaining eyes (cases 2, 4 and 10) exhibited a complete detachment of the donor membrane, with the graft appearing rolled up and floating in the anterior chamber. In these eyes a DSEK was performed without complications two or three weeks after the initial DMEK surgery. In the seven eyes that exhibited complete adhesion of the graft we observed a best corrected visual acuity (BCVA) ? to 0.7 in three eyes (43%) one month after surgery, in five eyes (71%) six months after surgery and in six eyes (86%) within the first and second year (table I). At six months after surgery, the mean endothelial cell density was of 2039 240 In 1998 we described that the DM transplant was technically possible in a cadaver human eye model (11,12). At the time, obtaining a DM from a donor corneal-scleral ring was seen as a challenge without the support of an eye bank. As on some occasions the peeling of the DM could be a challenge due to the inadvertent tearing of the membrane, the donor DM should preferably be prepared in the eye bank prior to surgery instead of during the operation itself. When the Amnitrans Eye Bank was established in Rotterdam (Amnitrans Eyebank Rotterdam) in January 2004, all its facilities and logistics were available for routine preparation of Descemet’s membrane transplants, and the assessment of its endothelial cell layer and the microbiological study of the tissue to ensure its sterility. Since then, extensive lab studies were made to simplify the procedure (14-18). In addition, a number of technical modifications were designed for the surgical implantation of the donor DM layer, its manipulation in the anterior chamber and its full adherence to the receiving posterior stroma. (Melles CRJ, unpublished data, 2005) (14,15). Recently, the possibility of transplanting an isolated DM was also demonstrated by Tappin and Pavel utilizing different approaches. Tappin designed an instrument for inserting a 7.5 mm diameter donor DM in the anterior chamber through a sutured 8.0 mm incision (21). Pavel described the DM donor tissue transplant linked to a stromal peripheral ring to facilitate its handling (P. Studeny. Descemet’s membrane with stromal hem transplantation. Winter ESCRS 2007). In this study, we transplanted ARCH SOC ESP OFTALMOL 2009; 84: 237-244 Transplante de membrana de Descemet Fig. 1: Slit lamp photograph of a transplanted cornea one year after performing DMEK (Case 6). A) notice the transparency of the transplanted cornea and the invisible anatomic interphase between the donor and host tissue. B) Notice the periphery of Descemet’s membrane signaled by the yellow arrow. DM with endothelium through a small tunnelized incision as previously described (11,12). Taking into account the terms utilized for differentiating different posterior lamellar keratoplasty procedures, the instant procedure, i.e. the isolated donor DM transplant carrying a feasible endothelial cell layer, was initially termed DMEK. The challenge in designing any posterior lamellar keratoplasty procedure is to provide a sufficiently high endothelial cellular density to obtain a longterm survival of the graft. In this study, both objective and subjective measures indicated that DMEK could be potentially able to achieve cellular densities approaching 2000 cells /mm 2 in the mid-term, comparable to those obtained after DLEK and DSEK (6-19). In comparison with the posterior lamellar keratoplasty techniques we designed in the past such as DLEK and DSEK (14), DMEK could have five main advantages: Firstly, this study suggests that the visual recovery after DMEK could be much faster than after DLEK or DSEK because six out of seven eyes with DMEK achieved a BCVA ≥ 0.5 one month after surgery (table I). In addition, in the first series described of 50 patients submitted to DMEK due to Fuchs’ endothelial dystrophy, 95% exhibited a BCVA ≥ 0.50.5, and more importantly 75% achieved a BCVA ≥ at 0.8 six months after surgery (22). These numbers are in contrast with DLEK or DSEK procedures which have demonstrated a mean BCVA ≥ 0.5 in an average time of six or more months (6,9,23). The difference in the visual acuity recovery might suggest that the presence of donor posterior stroma in DLEK and DSEK is what primarily determines the degree of visual recovery instead of secondary changes or edema in the receiving corneal stroma, because in DMEK there is no transplanted donor posterior stroma. However, in order to perform a DMEK it is necessary to have an adequate visualization of the anterior chamber due to the greater surgical complexity of the procedure. Therefore, in severely unbalanced corneas, in the presence of training devices for glaucoma, narrow anterior chamber or low potential for visual rehabilitation, it would be recommendable to perform a DSEK which is technically less challenging. In second place, as DMEK could provide a nearperfect restoration of the corneal anatomy and a better quality of the cornea, with this technique we could expect a greater recovery of the visual capacity (11,12). Accordingly, in DMEK the end visual ARCH SOC ESP OFTALMOL 2009; 84: 237-244 241 DAPENA I, et al. result might be limited only by the quality of the anterior portion of the receiving cornea prior to surgery. In Fuchs’ endothelial dystrophy it is not rare for visual acuity to be unrelated to the visual symptoms of the patient, and therefore in these cases VA would not be a good indicator for surgery. An example is case number 8 that exhibited a BCVA of 0.8 but a significantly decompensated cornea with sub-epithelial secondary changes and a significant alteration of sensitivity to contrast and color perception. In the third place, in DMEK the diameter of the graft can be of 9.0 up to 11.0 mm, which means that a greater endothelial cell surface is transplanted compared to DLEK (7.5 to 8.0 mm) or DSEK (8.5 to 9.5 mm). In our experience, even though the correlation between the diameter of the graft and its survival has not been demonstrated, we could expect that a larger graft in DMEK will benefit the long-term survival of the transplant. Fourth, DMEK could demonstrate a better fulfillment of current requirements for anterior segment of modern surgery because the donor DM can be transplanted through a tunnelized incision in a clear cornea, which is widely utilized in phacoemulsification surgery and is known to induce a minimum post-op astigmatism (17,24,25). Even though several instruments have been described for inserting a donor DM (21,26,27), its utilization could Limit the end diameter of the graft (6.0 to 7.5 mm), in addition to requiring a relatively large entry incision. Fifth, in contrast with DLEK and DSEK, where the majority of surgeons would require a microkeratome or femtosecond laser, in DMEK the donor DM films can be «peeled» directly from a cornealscleral ring. With our technique for preparing 9.0 mm DM films from concave donor corneal-scleral rings, the magnitude of the cellular lesion expressed in the «percentage of damaged mean endothelial surface area» is of 3.4% (11,12,18). Similar results were found by Ignacio et al, who obtained Descemet transplants from convex rings (28), and Zhu et al, who preserved rectangular films from concave rings (29). It is important to emphasize that all of the studies were made in preserved tissue, either in cold storage or in organ culture medium. Accordingly, if it is possible to routinely obtain viable grafts from preserve tissue, DMEK could be much more accessible for the majority of corneal surgeons than DLEK or DSEK. 242 As with DSEK/DSAEK, the graft detachment was the most frequent complication in DMEK. In the first described series of 50 patients submitted to DMEK due to Fuchs’ endothelial dystrophy, the rate of detachment was 25%. However, when analyzing the last 25 patients who were intervened with this procedure, the detachment rate went down to 12%. This reduction was related to the learning curve, changes in the surgical technique and in the techniques utilized in the eye bank as well as to the extension of the time for filling the anterior chamber with air in 45-60 minutes (22). In our experience, the most important factor for obtaining a complete adhesion of the donor tissue is to avoid the use of hyaluronic acid throughout the procedure (14). As with DSEK, all viscoelastics should be avoided in DMEK because the detachment of the donor tissue is strongly correlated with their utilization (14). In vitro experiments have proved that filling the anterior chamber with air for at least 30 minutes is essential to obtain a complete adhesion of the donor tissue in DMEK whereas an air filling of only 15 minutes would be sufficient in DLEK and DSEK (8,14). Our experience with DMEK suggests that the transplant of isolated donor DM carrying feasible endothelium for treating alterations of the corneal endothelium provides a near-perfect anatomic restoration and a high degree of visual rehabilitation. As in DLEK and DSEK, the main drawback of the procedure is the risk of detachment of the graft in the early post-op (16). When the percentage of detachments in DMEK can be reduced due to improvements in the eye bank logistics and also in the surgical technique, the project of posterior lamellar keratoplasty should finally be completed. REFERENCES 1. Melles GR, Eggink FA, Lander F, Pels E, Rietveld FJ, Beekhuis WH, et al. A surgical technique for posterior lamellar keratoplasty. Cornea 1998; 17: 618-626. 2. Melles GR, Lander F, Beekhuis WH, Remeijer L, Binder PS. Posterior lamellar keratoplasty for a case of pseudophakic bullous keratopathy. Am J Ophthalmol 1999; 127: 340-341. 3. Melles GR, Lander F, van Dooren BT, Pels E, Beekhuis WH. Preliminary clinical results of posterior lamellar keratoplasty through a sclerocorneal pocket incision. Ophthalmology 2000; 107: 1850-1857. 4. Terry MA, Ousley PJ. Deep lamellar endothelial keratoplasty in the first United States patients: early clinical results. Cornea 2001; 20: 239-243. ARCH SOC ESP OFTALMOL 2009; 84: 237-244 Transplante de membrana de Descemet 5. Melles GR, Lander F, Nieuwendaal C. Sutureless, posterior lamellar keratoplasty. Cornea 2002; 21: 325-327. 6. Terry MA, Ousley PJ. Small-incision deep lamellar endothelial keratoplasty (DLEK): six-month results in the first prospective clinical study. Cornea 2005; 24: 59-65. 7. Melles GR, Wijdh RH, Nieuwendaal CP: A technique to excise the descemet membrane from a recipient cornea (descemetorhexis). Cornea 2004; 23: 286-288. 8. Melles GR, Kamminga N. Tecniques for posterior lamellar keratoplasty through a scleral incision. Ophthalmologe 2003; 100: 689-695. 9. Price FW Jr, Price MO. Descemet’s stripping with endothelial keratoplasty in 200 eyes: Early challenges and techniques to enhance donor adherence. J Cataract Refract Surg 2006; 32: 411-418. 10. Dapena I, Ham L, Melles GRJ. Endothelial keratoplasty. DSEK/DSAEK or DMEK: The thinner the better? Curr Opin Ophthalmol, in press. 11. Melles GRJ, Rietveld FJR, Pels E, Beekhuis WH, Binder PS. Transplantation of Descemet’s membrane carrying viable endothelium through a small scleral incision. Invest Ophthalmol Vis Sci 1998; 39: S76. 12. Melles GR, Lander F, Rietveld FJ. Transplantation of Descemet’s membrane carrying viable endothelium through a small scleral incision. Cornea 2002; 21: 415-418. 13. Melles GR, Ong TS, Ververs B, van der Wees J. Descemet membrane endothelial keratoplasty (DMEK). Cornea 2006; 25: 987-990. 14. Melles GR. Posterior lamellar keratoplasty: DLEK to DSEK to DMEK. Cornea 2006; 25: 879-881. 15. Melles GR, Ong TS, Ververs B, van der Wees J. Preliminary clinical results of Descemet membrane endothelial keratoplasty. Am J Ophthalmol 2008; 145: 222-227. 16. Ham L, van der Wees J, Melles GR. Causes of primary donor failure in Descemet membrane endothelial keratoplasty. Am J Ophthalmol 2008; 145: 639-644. 17. Nieuwendaal CP, Lapid-Gortzak R, van der Meulen IJ, Melles GJ. Posterior lamellar keratoplasty using descemetorhexis and organ-cultured donor corneal tissue (Melles technique). Cornea 2006; 25: 933-936. 18. Lie JT, Birbal R, Ham L, van der Wees J, Melles GR. Donor tissue preparation for Descemet membrane endo- 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. thelial keratoplasty. J Cataract Refract Surg 2008; 34: 1578-1583. van Dooren BT, Mulder PG, Nieuwendal CP, Beekhuis WH, Melles GR. Endothelial cell density after deep posterior lamellar keratoplasty (Melles techniques): 3 years follow-up. Am J Ophthalmol 2004; 138: 211-217. van Dooren BT, Mulder PG, Nieuwendal CP, Beekhuis WH, Melles GR. Endothelial cell density after deep anterior lamellar keratoplasty (Melles technique). Am J Ophthalmol 2004; 137: 397-400. Tappin M. A method for true endothelial cell (Tencell) transplantation using a custom-made cannula for the treatment of endothelial cell failure. Eye 2007; 21: 775-779. Ham L, Dapena I, van Luijk C, van der Wees J, Melles GR. Descemet membrane endothelial keratoplasty (DMEK) for Fuchs endothelial dystrophy: review of the first 50 consecutive cases. Eye. 2009. [Epub ahead of print] Gorovoy MS. Descemet-stripping automated endothelial keratoplasty. Cornea 2006; 25: 886-889. Holweger RR, Marefat B. Corneal changes after cataract surgery with 5.0 mm sutured and 3.5 mm sutureless clear corneal incisions. J Cataract Refract Surg 1997; 23: 342-346. Olsen T, Dam-Johansen M, Bek T, Hjortdal JO. Corneal versus scleral tunnel incision in cataract surgery: a randomized study. J Cataract Refract Surg 1997; 23: 337-341. Lange TM, Wood TM, McLaughlin BJ. Corneal endothelial cell transplantation using Descemet’s membrane as a carrier. J Cataract Refract Surg 1993; 19: 232-235. Shimmura S, Miyashita H, Knomi K, Shinozaki N, Taguchi T, Kobayashi H, et al. Transplantation of corneal endothelium with Descemet’s membrane using a hyroxyethyl methacrylate polymer as a carrier. Br J Ophthalmol 2005; 89: 134-137. Ignacio TS, Nguyen TT, Sarayba MA, Sweet PM, Piovanetti O, Chuck RS, et al. A technique to harvest Descemet’s membrane with viable endothelial cells for selective transplantation. Am J Ophthalmol 2005; 139: 325330. Zhu Z, Rife L, Yiu S, Trousdale MD, Wasilewski D, Siqueira A, et al. A technique for preparation of the corneal endothelium-Descemet’s membrane complex for transplantation. Cornea 2006; 25: 705-708. ARCH SOC ESP OFTALMOL 2009; 84: 237-244 243