Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
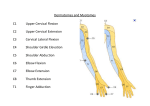
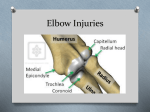
10- Exam of Elbow, Radius, Ulna Most are overuse injuries: all treatments conservative Uniaxial hinge Joint: Multifaceted articulation Capitellum and trochlea of the distal end of the humerus combine with: ◦ Radial head and olecranon of the proximal radius and ulna Annular ligament holds the radius and ulna together Humeroulnar joint is the true elbow joint Capsule reinforced and thickened (Lateral: radial and medial: ulnar= most important) Stabilize in flexion and extension Median Nerve ◦ Crosses the elbow medially ◦ Passes through the two heads of the pronator teres Ulnar Nerve ◦ Passes along the medial arm and posterior to the medial epicondyle ◦ Through the cubital tunnel Radial Nerve ◦ Descends the arm laterally, dividing into the superficial (sensory) branch and the deep (motor or posterior interosseous) branch ◦ The deep branch passes through the Arcade of Frohse, where it is most susceptible to injury History and PE: History, Inspection, Palpation, ROM, Muscle/Neuro testing, Specific tests History: age, occupation, type injury, pain, alleviate/relieve, previous injury, OLD CARTS/PQRSTA Provocative or Palliative-What causes the symptom? What makes it better or worse? What have you done to get relief? Quality or Quantity-What is the character of the symptom, i.e., pain: is it crushing, piercing, dull, sharp? Region or Radiation-Where is the symptom? Does it spread? Severity-How does the symptom rate on a severity scale of 1-10 with 10 being the most intense pain the patient (subjective) has ever had. Timing-When did the symptom begin? How long does it last? How often does it occur? Is it sudden or gradual? Associated signs and symptoms of the chief complaint. Examine Joint above and Joint below Inspection: expose, compare bilaterally, joint alignment, previous injury, muscle imbalances, functional Carrying angle: Normally 10-15 degrees (female>male) Cubitus valgus: >15 (forearm deviating outwards) Cubitus varus: <10 (forearm deviating towards midline) 10- Exam of Elbow, Radius, Ulna Palpation: TART ROM: flexion, extension, pronation, supination Muscle Strength 0/5 No muscle movement 1/5 Visible movement but not at the joint 2/5 Movement at the joint but not against gravity 3/5 Movement against gravity but not against added resistance 4/5 Movement against resistance but less than normal 5/5 Normal strength Neuro: C5=Biceps; C6=Brachioradialis; C7=Triceps Tinel’s test: tapping over a nerve to elicit pain along nerves Elbow Extension Test: inability to extend suggests need for Xray Milking Maneuver: elbow flexed to >55, hand supinated, patient/DO may pull down own thumb Pain=positive test Moving Valgus Test: patient experiences reproduction of symptoms in an arc as the elbow goes from 120 degrees flexion to 70 degrees extension 10- Exam of Elbow, Radius, Ulna Injuries Anterior: Biceps Tendon Rupture: weakness of supination and flexion; tender to palpation Deformity as muscle belly contracts (avulsion fragment from radial tuberosity) Risk: male, >30, steroids Posterior: Triceps Tendonitis: tenderness around insertion of the triceps (posterior elbow) Pain with resisted extension of the elbow Olecranon bursitis (miners/students elbow): Relatively painless posterior swelling (no erythema/temp change) Septic bursitis: infection (aspirate/culture); protection Medial: Epicondylitis: Golfers elbow (overuse of wrist flexors) Microtears to the tendon at medial epicondyle Increased pain with resisted wrist flexion and forearm pronation Epicondylitis: Rest, Ice, Anti-inflammatories, steroids Ulnar Collateral Sprain (MCL): pitchers= tenderness over humeroulnar joint; repetitive valgus stress (20-130 degrees) May have ulnar nerve irritation Pain increases by manual valgus stress; milking maneuver Medial Apophysitis: Any tension stress may partially or completely tear off the medial epicondyle Either fast or gradual onset of pain, with swelling/bruising Pitchers: treat via education, biomechanics, limiting pitches, rest, NSAIDs, Rehab Cubital Tunnel Syndrome: 2nd most common compression neuropathy behind CTS(carpal) Mechanical compromise of ulnar nerve: Direct insult, excessive traction/compression Positive Tinel’s test: weakness of intrinsic hand muscles Flexor-Pronator Mass Syndrome: purely sensory syndrome (median n. becomes trapped) Resisted flexion of FDS rtendon of index/middle finger Anterior Interosseous Syndrome: mostly motor syndrome: minimal or no sensory loss Weakness or loss of flexion of DIP joint of thumb index finger Lateral: Nursemaids elbow: pull childs arm, axial traction on extended/pronated arm Pulls radius distally (supinate and pronate and it pops back into place) Epicondylitis: tennis elbow (overuse of wrist extensors) Microtears of the tendon at lateral epicondyle More common than medial Ache over lateral epicondyle (difficulty with wrist extension: ie pick up cup) General treatment for all: Rest, Ice, OMM, splint, rehab, steroid, Surgery last resort SP Always write: OMM, meds, labs, xrays, followup, patient voices understanding and agrees with the above treatment