Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
SYNOPSIS
Name of Sponsor/ Company
Chugai Pharmaceutical Co., Ltd.
Name of Finished Product
ACTEMRA
Name of Active Ingredient
tocilizumab
Title of Study
Investigators
Study centre(s)
Publication
(reference)
Clinical Pharmacology Study of MRA in Rheumatoid Arthritis
Patients with Renal Impairment
Yukio Yuzawa and Kiyoshi Takasugi
Nagoya University Hospital, Nephrology Department and Dohgo
Spa Hospital, Internal Medicine Department
None
Studied Period
(date of first enrolment)
13 January 2005 - 6 October 2005
(date of last complete)
Phase of development
Clinical pharmacology study
The objectives are to investigate the blood pharmacokinetics of
Objectives
MRA after single administration in rheumatoid arthritis patients
with renal impairment, and to evaluate safety as well.
The blood pharmacokinetics of MRA are investigated after single
Methodology
intravenous infusion of the drug at a dose of 8 mg/kg in
rheumatoid arthritis patients with renal impairment in an
open-label study, and safety is also evaluated.
Patients will be included using the creatinine clearance (CrCL)
values as defined below.
Renal
impairme
nt
classificat
Number of patients
(planned and analysed )
CrCL
(mL/min)
Target
sample
size
Moderate
Severe
(No renal
impairme
80 ≥ CrCL
> 50
50 ≥ CrCL
> 30
30 ≥ CrCL
> 10
CrCL > 80
d
patient
s
ion
Mil
Enrolle
Safety
evaluation set
Pharmacokineti
c analysis set
FAS
≥4
4
4
≥4
5
5
No limit
3
3
2
2
Exclude
d
as
nt)
subjects
Total
―
10
14
14
Main inclusion criteria
Patients with RA duration of 6 months or more
Patients whose ESR (Westergren method) is ≥30 mm/hr or CRP
is ≥1.0 mg/dL
Main exclusion criteria
Patients assessed as having Class IV Steinbrocker functional
Diagnosis and main criteria for
activity
inclusion
Patients who have been treated for the underlying disease with a
biological agent (infliximab or etanercept, etc.) or leflunomide
Patients who received the drugs and therapies that may affect
evaluation of drug efficacy
Other patients who are unsuitable for safety reason <0}{0>その
他、治験責任医師あるいは治験分担医師が不適当と判断した患者
<}0{>s
Investigational product,: MRA (Tocilizumab [recombinant])
Test product, dose and mode of
Dose
and
method
of administration: 8
administration, batch number
intravenously drip infused over 1 hour.
mg/kg MRA is
Lot No.: MR4C05A
Duration of treatment
35 days
Reference therapy, dose and
mode of administration, batch
A comparator is not used in this study.
number
Pharmacokinetics
Serum MRA concentration and pharmacokinetic parameters
Criteria for evaluation
after administration of MRA.
Efficacy
ACR20 response rate, Time course of DAS28 from baseline
Safety
Pharmacokinetics
The maximum serum drug concentration (Cmax), area under the
serum
Statistical method
drug
concentration-time
curve
(AUC),
apparent
elimination rate constant (kel), elimination half-life (t1/2), total
clearance
(CL),
volume
of
distribution
(Vd),
volume
of
distribution at steady state (Vss) and mean residence time
(MRT), etc., are determined for each patient from the serum
MRA concentrations.
The Cmax is determined from the actual measured values, the
AUC is determined using the trapezoidal rule (linear/log
trapezoidal rule) and the terminal elimination phase is
extrapolated using the linear least squares method. The profile of
the serum drug concentration for each patient is graphed and
summary statistics are calculated at each time by renal
impairment class.The pharmacokinetic parameters are plotted
according to the distribution, and the summary statistics are
calculated. In addition, an exploration is conducted into the
effects on pharmacokinetic parameters due to the deterioration
of renal function.
Efficacy
For both FAS and PPS, time courses of continuous scale
variables are plotted, and nominal and ordinal scale variables
are represented in table form using a suitable method such as
cross-tabulation by time point, etc. The 95% confidence intervals
at each time point are estimated for the above-mentioned
variables.
Pharmacokinetics
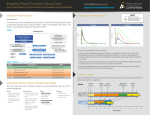
The serum MRA concentration slowly decreased after treatment
and followed a similar time course for all of the renal impairment
classes.
The Cmax did not differ as a result of the degree of renal
impairment, but the AUCfin was slightly greater in the patients
with severe renal impairment than in the patients of the other
renal impairment classes.
Summary - Conclusions
Examination of the relationship between baseline CrCL and the
Cmax and AUCfin, the coefficient of correlation with CrCL was
small for both parameters.
Efficacy
The ACR20 response rate for the patients as a whole was 28.6%
(4 of 14 patients). The ACR20 response rate by renal impairment
class was 25.0% (1 of 4 patients) in the patients with mild renal
impairment, 20.0% (1 of 5 patients) in the patients with
moderate renal impairment, 33.3% (1 of 3 patients) in the
patients with severe renal impairment and 50.0% (1 of 2
patients) in the patients without renal impairment. The DAS28
score on Day 28 after treatment was similarly decreased in all of
the groups.
Safety
The incidence did not differ as a result of the degree of renal
impairment. The most common events (PT) were increased blood
triglycerides and eczema. There were no events that appeared to
have been attributable to renal impairment.
Serious adverse events consisted of a skin ulcer and peripheral
neuropathy with moderate renal impairment. The outcome was
“resolved/recovered” for the skin ulcer and “improved” for
peripheral neuropathy.
None of the laboratory test variables showed clinically
problematic changes and renal function did not worsen either.
Conclusions
The degree of renal impairment did not have any effect on the
pharmacokinetics of MRA. Based on these results, dosage of
MRA therefore does not need to be adjusted even if the patient
has rheumatoid arthritis with renal impairment.
Date of report
8 July 2011