Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Plateau principle wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacognosy wikipedia , lookup
Neuropharmacology wikipedia , lookup
Psychopharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Dydrogesterone wikipedia , lookup
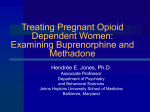
Subjective and physiologic effects of intravenous buprenorphine in humans The pharmacologic profile of sublingual and subcutaneous buprenorphine, a partial opioid agonist, indicates it may be useful as a maintenance drug in the treatment of opioid dependence. However, illicit intravenous self-administration suggests that it may have a greater abuse potential by this route of administration. Physiologic and subjective effects of intravenous buprenorphine (0.0, 0.3, 0.6, and 1.2 mg) were determined in a dose-escalation study in six nondependent volunteers with histories of opioid use. Buprenorphine caused miosis and decreased respiratory rate, increased diastolic blood pressure, and transiently increased heart rate. Buprenorphine increased positive responses on a "feel drug" question and scores on scales of "liking," "good effects," euphoria, and apathetic sedation. Physiologic and subjective responses were not consistently dose related, a finding compatable with the pharmacologic profile of a partial agonist. The findings indicate that buprenorphine has substantial potential for abuse when administered intravenously. (CLIN PHARMACOL THER 1993;53:570-6.) Wallace B. Pickworth, PhD, Roney E. Johnson, PharmD,a Barbara A. Holicky, RN, and Edward J. Cone, PhD Baltimore, Md. Buprenorphine is a partial opioid agonist1'2 with an analgesic potency 25 to 40 times that of morphine.3 Buprenorphine has a high therapeutic index and low toxicity even at high doses.4'5 These characteristics led Jasinski et al.6 to study the effects of short- and long-term subcutaneous administration of buprenorphine in former opioid addicts. They found that single doses of buprenorphine produced morphine-like effects, including miosis and elevations of the morphine-benzedrine group (MBG) and pentobarbitalchlorpromazine-alcohol group (PCAG) subscales of the Addiction Research Center Inventory (ARCI).7 During long-term administration of buprenorphine, the effects of subcutaneously administered morphine (120 mg) were attenuated, and on abrupt discontinuation of buprenorphine a mild and delayed abstinence syndrome was observed. These findings suggested that buprenorphine may be effective for the treatment of opioid addiction.6 Subsequently, Mello and MendelFrom the National Institute on Drug Abuse, Addiction Research Center. Received for publication Sept. 21, 1992; accepted Dec. 26, 1992. Reprint requests: Edward J. Cone, PhD, Clinical Pharmacology Branch, NIDA, Addiction Research Center, P.O. Box 5180, Baltimore, MD 21224. 'Present address: The Johns Hopkins School of Medicine, Department of Psychiatry and Behavioral Sciences, Behavioral Pharmacology Research Unit, 5510 Nathan Shock Dr., Baltimore, MD 21224. 13/1/45127 570 son8 reported that subjects maintained on daily sublin- gual doses of buprenorphine self-administered fewer opioids than those maintained on placebo. Bickel et al.9 compared the efficacy of daily administration of buprenorphine (2 mg, sublingual) and methadone (30 mg, oral) in a double-blind outpatient detoxification study. They concluded that buprenorphine was acceptable to patients and as effective as methadone. In a second study, Bickel et al.1° reported that long-term buprenorphine treatment caused dose-dependent blockade of hydromorphone challenges. These findings were extended in studies that assessed a rapid-dose induction procedure," and once daily versus every-other-day dosing of sublingual buprenorphine.12 Further, in an outpatient clinical trial, buprenorphine (8 mg, sublingual) was as effective as methadone (60 mg, oral) in decreasing the number of opioid-positive urine samples.13 The findings from these and other pharmacologic and treatment studies led to the initiation of a multicenter trial with buprenorphine to assess its usefulness in treating opioid-dependent patients. The increased availability of buprenorphine could lead to its abuse, particularly if the dosage form could be injected intravenously. Self-administration of buprenorphine has been reported to occur in countries in which buprenorphine is easily available. Pharmacists and physicians in New Zealand noted increasing demands for buprenorphine.14'15 Subsequently, abuse of buprenorphine among opioid addicts was reported in Ireland,16 Germany,17 Scotland, /8 and CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 53, NUMBER 5 Australia. 19 In most instances, addicts reportedly preferred the intravenous route of administration 20 Typically the user would obtain one or more 0.2 mg tablets, manufactured for sublingual administration, dissolve them in water, and inject the solution intravenously.21 In the present study, the pharmacologic and subjective effects of high intravenous doses of buprenorphine were evaluated. For safety reasons, placebo and three doses of buprenorphine were administered in as- cending order. Subjects were aware that they were participating in a dose run-up safety evaluation study of intravenously administered buprenorphine, but they were not aware of actual doses. METHOD Subjects Six healthy paid male volunteers participated in this inpatient research study. All subjects had histories of opioid abuse but were not opioid dependent at the time of their admission to the clinical research ward of the Addiction Research Center (NIDA, Baltimore, Md.). Each subject was a current smoker (average, 16 cigarettes per day) and each self-reported regular ethanol use before admission. The subjects' mean age was 34.1 years (age range, 27 to 40 years), and their weight averaged 68.6 kg (weight range, 63.6 to 73.3 kg). Each subject signed a consent form approved by the local institutional review board (Francis Scott Key Medical Center, Baltimore, Md.) that described the experiment's procedures, risks, and benefits. The study protocol and consent form met Department of Health and Human Services guidelines for human experimentation. Drug administration This dose run-up phase preceded a study of the bioavailability of buprenorphine. In the dose run-up phase, each subject received intravenous injections in the following ascending order: placebo (water for injection) and 0.3, 0.6, and 1.2 mg buprenorphine. Drug solutions were prepared for injection by dissolving buprenorphine hydrochloride in water for injection; the pH was adjusted to 4.0 to 4.5 with 0.1 mol/L hydrochloric acid. Drug solutions were administered in a 1 ml volume over 1 minute through a catheter inserted into an antecubital vein. Drug administration sessions were separated by at least 48 hours. Study measures Physiologic measures. Systolic and diastolic blood pressure and pulse rate were recorded from an auto- Pickworth et al. 571 mated recording device. The pupil diameter was determined from Polaroid (Polaroid Corp., Cambridge, Mass.) photographs of the eye by use of methods described by Marquardt et al.22 Respiration rate was obtained from 15 second observations of chest excursion. Subjective measures. Subjects rated the drug effect by drawing a vertical line through a 200 mm visual analog scale anchored with the adjectives "good" and "bad." The opiate Single Dose Questionnaire (SDQ)23 and subscales of the ARCI,7 including the MBG (a measure of euphoria), PCAG (a measure of apathetic sedation), and the lysergic acid diethylamide (LSD; a measure of drug-induced dysphoria) subscales24 were administered by means of a computer. Performance measure. The circular lights task,25 a hand-eye coordination test, was used for evaluation of drug-induced performance effects. Data collection Physiologic, subjective, and performance data were collected before and up to 48 hours after drug administration. Measurement times differed for each dependent variable. The number of measurements varied as follows: two in the hour before the drug (after the insertion of the venous catheter), seven in the first hour after the drug, seven at 1/2-hour intervals between 1 and 4 hours, three at hourly intervals between 4 and 6 hours, and four at 2-hour intervals between 6 and 14 hours. On the second day, dependent measures were collected at 22, 24, 26, 28, 32, and 38 hours after drug administration. Data analysis Treatment conditions were presented in ascending order and the subjects were aware of this aspect of the experimental design. Because the treatments were not administered randomly, subjective measures could have been influenced by expectation and anticipation of drug effect. It is also possible that residual effects from previously administered doses of buprenorphine influenced the response to subsequent administrations. These considerations precluded the use of conventional ANOVA procedures. Consequently, the findings were presented with descriptive statistics. RESULTS Physiologic measures Respiration. As shown in Fig. 1, A, intravenous buprenorphine caused a dose- and time-related decrease in the respiratory rate. The effect was evident within 15 minutes and reached a maximum at 45 min- CLINICAL PHARMACOLOGY & THERAPEUTICS 572 Pickworth et al. MAY 1993 Respiration A 22B o 20- 2 18- 2 16- 75 .73 r, 70 65 gi 14- 60 12 Pulse Rate 90 ID 0-M Placebo 0.3 mg 0.6 mg 1.2 mg 5 g 80 4 oda Pupil Diameter 6p 85 75 Diastolic Blood Pressure 80- 3 2 70 65 Pre- Pre- 0 0 1 2 3 4 5 6 12 18 24 Hour Fig. 1. Time-action curves for physiologic parameters: respiration (A), diastolic blood pressure (B), pulse rate (C), and pupil diameter (D) after intravenous buprenorphine (0.3, 0.6, and 1.2 mg) and placebo (n = 6). utes after drug administration. Respiratory rate gradually increased and attained baseline levels after 6 hours. Blood pressure. Diastolic blood pressure (Fig. 1, B) increased after buprenorphine. The diastolic pressure increase was small (average, 5 mm Hg), and the values returned to control levels within 4 hours. Systolic blood pressure (data not shown) was not significantly affected by buprenorphine. Heart rate. Each dose of buprenorphine, but not placebo, transiently increased the pulse rate (Fig. 1, C). The effect was maximal 5 to 10 minutes after the injection and returned to baseline level in approximately 3 hours. The response was not dependent on the dose of buprenorphine. Pupil diameter. Buprenorphine decreased pupil diameter (Fig. 1, D). The effect was evident within 10 minutes and persisted for 24 hours after the 0.3 and 0.6 mg doses and for 48 hours (data not shown) after the 1.2 mg dose. Performance measure Buprenorphine caused a slight (7%) but sustained decrease in response rate on the circular lights task between 1/2 hour and 3 hours after drug administration (Fig. 2, A). Subjective effects Feel drug. Subjects consistently answered affirmatively to the question "Do you feel the drug?" from the SDQ.23 As shown in Fig. 2, B, beginning 5 minutes after buprenorphine and lasting for 4 hours, at least five of the six subjects reported positive responses. After placebo administration, there were no affirmative responses to the question "Do you feel the drug?" Subject liking. Buprenorphine caused an orderly increase of scores on the drug-liking question of the SDQ (Fig. 2, C). The effect peaked during the first hour and gradually declined to values that were not different from placebo at 8 hours. Good and bad effects. Subjects reported no bad effects after placebo or at any time after buprenorphine, but ratings of good effects increased after buprenorphine. Increases were evident 5 minutes after the injection, peaked at 1 hour, and gradually declined to baseline values within 5 hours (Fig. 2, D). The 0.6 mg dose exerted a greater effect than the 1.2 mg dose, but analysis of area under the curve indicated no difference. ARC! subscales. Buprenorphine increased scores on the MBG (Fig. 3, A) and PCAG (Fig. 3, B) subscales of the ARCI. There was a slight transient in- CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 53, NUMBER 5 105 100 Pickworth et al. Circular Lights A 573 1.0 0.8 Aso 0.8 95. 0.4 90 - 0.2 e0 6 Subject's Liking Pre- 0 1 2 3 4 5 12 0.0 Placebo Good Effects 0.3 mg 0.6 mg 1.2 mg 18 24 Pre- 0 1 2 3 4 56 12 18 24 Hour Fig. 2. Time-action curves for circular lights (A), feel drug (B), subject's liking (C), and good effects (D) after intravenous buprenorphine (0.3, 0.6, and 1.2 mg) and placebo (n = 6) (maximal score on subject's liking, 5; maximal score on good effects, 100). crease in scores on the LSD subscale (Fig. 3, C). The 1.2 and 0.6 mg doses caused similar increases in the MBG subscale; these scores were greater than after the 0.3 mg dose. After all doses, MBG increases were maximal within 30 minutes and declined to placebo values within hour after the low dose and 21/2 hours after the higher doses. The PCAG subscale score gradually increased, reaching a peak 2 hours after the high dose and 5 hours after the low dose. Increases in scores on the PCAG subscale occurred later and persisted longer than those observed for the MBG or LSD subscales. 1 DISCUSSION Although there have been numerous reports of buprenorphine abuse,14-16.19'2° this appears to be the first study that shows increases in scores for drug liking, good effects, and drug-induced euphoria after intravenous buprenorphine administration. Intravenous buprenorphine changed physiologic and subjective measures that are valid predictors of the abuse liability of opioids.24 However, the changes in subjective and physiologic responses were not consistently dose related. This profile is compatible with the characterization of buprenorphine as a partial opioid agonist. Buprenorphine increased scores on the MBG subscale of the ARCI to mean 5-hour total score of 60. This score was comparable to that observed for intravenous morphine (20 mg/70 kg) or heroin (10 mg/70 kg).26 Other measures of drug-induced euphoria (e.g., liking scale of the SDQ23 and the visual analog "good effects") were increased; these responses were similar to those of intravenous morphine (30 mg).27 The lack of increase in MBG subscale scores between the 0.6 and 1.2 mg doses suggests a ceiling effect occurred on this measure. A curvilinear dose-response curve is typical of the buprenorphine response in animal studies,2 and plateau effects have been reported for MBG and drug-liking scales in human studies.6.28 The high dose of buprenorphine increased PCAG subscales scores; the peak effect occurred between 2 and 5 hours after the intravenous administration of the drug. In a study of long-term buprenorphine (Mello et al.29), drowsiness and sedation occurred in three of seven subjects during the first 6 days of subcutaneous buprenorphine administration; however, tolerance seemed to develop to the effect with continued daily administration. Jasinski et al.6 also reported PCAG score increases after subcutaneous buprenorphine. In this study and the study by Jasinski et al.,6 increases in PCAG subscales scores occurred later than the increases in MBG scores. Concurrent with the PCAG score increase, there was a small decrement in circular lights performance. Weinhold et al.3° also reported a CLINICAL PHARMACOLOGY & THERAPEUTICS MAY 1993 574 Pickworth et al. A MBG 161 12 10 - 8 6- oAN 42 PCAG 15), 7 6 4 3 0 OE 2 LSD --0 0----- Placebo 0.3 mg 0.8 mg 1.2 mg 3- 2- 1 A 0 Pre- 0 2 4 5 6 12 18 24 Hour Fig. 3. Time-action curves for the morphine-benzedrine group (MBG) subscale (A), the pentobarbital-chlorpromazine-alcohol group (PCAG) subscale (B), and the lysergic acid diethylamide (LSD) subscale (C) after intravenous buprenorphine (0.3, 0.6, and 1.2 mg) and placebo (n = 6). Maximal scores are indicated on the ordinate. small but significant decrease in performance on the Digit Symbol Substitution Test after intramuscular buprenorphine administration. Together, these findings suggest that high intravenous doses of buprenorphine cause drowsiness, sedation, and impaired performance. In the present study, buprenorphine caused a small decrease in respiratory rate that persisted for 6 hours. This finding agrees with Weinhold et al.,3() who reported that intramuscular buprenorphine decreased respiratory rates, and with the report by Ga1,31 who found that intravenous buprenorphine (0.3 mg/70 kg) reduced indexes of carbon dioxide responsiveness to about one half of control values. Walsh et al.28 reported a small decrease in respiratory rate that appeared to plateau as the sublingual dose of buprenorphine was increased to 32 mg. However, after subcutaneous administration of doses up to 8 mg, decreases in respiratory rate were not reported.° Our findings differ from those of Budd,32 where intravenous buprenorphine (0.4 to 7 mg) did not change depth, rate, or patterns of breathing in postoperative patients. The lack of respiratory depression in the Budd study32 might be explained by an inverted U-shape dose-response curve. A dose-dependent miosis was evident immediately after intravenous buprenorphine administration and persisted for 24 hours after the lower doses and up to 48 hours after the high dose. In these same subjects, intravenous buprenorphine caused a long-lasting decrease in pupil size and a diminution in the constriction and dilation velocities and the amplitude of the light reflex.33 Jasinski et al.° reported that 8 mg subcutaneous buprenorphine caused miosis. Sublingual buprenorphine also caused miosis and decreased the light reflex in heroin-dependent addicts.34 The findings of our study indicate that intravenous buprenorphine has a pharmacologic profile similar to other opioid agonists. Buprenorphine causes miosis, a slight decrease in respiratory rate, and subjective effects that included elevation in drug liking, good effects, and increases in the MBG scores. These actions are consistent with the suggestion that intravenous buprenorphine has substantial abuse potential. This suggestion is supported by worldwide reports of unauthorized intravenous administration of buprenorphine. On the other hand, the respiratory rate decrease, MBG elevations, and estimates of good effects after the 1.2 mg dose were not significantly greater than those after the 0.6 mg dose. It appears that a plateau exists for these measures. Further increases in the dose of buprenorphine may not increase these effects. A decrease of effect could occur, as it does for electroencephalographic,35 analgesic,2 and operant behavior in animal studies,36 and for respiratory and subjective effects after sublingual doses in humans.28 These effects are characteristic of partial agonists. Thus the agonist effects of buprenorphine may be self-limiting and the abuse potential restricted to lower doses. If this is the case, it is unclear how tolerance would affect the abuse potential of buprenorphine under conditions of long-term administration. Understanding the abuse potential of intravenous buprenorphine has practical and theoretic importance. If buprenorphine becomes a widely used treatment for CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 53, NUMBER 5 opioid dependence, drug diversion is likely to occur. Combinations of buprenorphine with opioid antagonists may prevent illicit intravenous use. Preston et al." reported that combinations of buprenoThine and naloxone administered to opioid-dependent subjects produced fewer opioid withdrawal signs and symptoms than naloxone alone. The authors suggested that a buprenorphine-naloxone combination would have a low potential for abuse in opioid-dependent subjects. In another study, concurrent naloxone administration attenuated the opioid effects of buprenorphine in nondependent opioid users." The findings from the present study indicate that buprenorphine formulations to be used in the treatment of opioid dependence should be examined carefully for abuse potential in both dependent and nondependent subjects. We gratefully acknowledge the technical support of Ms. Michelle Whitely and the editorial assistance of Ms. Patricia Y. Thomas. References Cowan A, Doxey JC, Harry ETR. The animal pharmacology of buprenorphine, an oripavine analgesic agent. Br J Pharmacol 1977;60:547-54. Cowan A, Lewis JW, Macfarlane IR. Agonist and antagonist properties of buprenorphine, a new antinociceptive agent. Br J Pharmacol 1977;60:537-45. Houde RW. Analgesic effectiveness of the narcotic agonist-antagonists. Br J Clin Pharmacol 1979;7:297S308S. Lewis JW, Rance MJ, Sanger DJ. The pharmacology and abuse potential of buprenorphine: a new antagonist analgesic. In: Mello NK, ed. Advances in substance abuse: behavioral and biological research, vol. 3. Greenwich: JAI Press, 1982:103-54. Banks CD. Overdose of buprenorphine: case report. NZ Med J 1979;89:255-6. Jasinski DR, Pevnick JS, Griffith JD. Human pharmacology and abuse potential of the analgesic buprenorphine. Arch Gen Psychiatry 1978;35:501-16. Haertzen CA. An overview of the Addiction Research Center Inventory (ARCI): an appendix and manual of scales. DHEW pub no (ADM) 79. Washington: Department of Health Education and Welfare, 1974. Mello NK, Mendelson JH. Buprenorphine suppresses heroin use by heroin addicts. Science 1980;207:657-9. Bickel WK, Stitzer ML, Bigelow GE, Liebson IA, Jasinski DR, Johnson RE. A clinical trial of buprenorphine: comparison with methadone in the detoxification of heroin addicts. CLIN PHARMACOL TIER 1988;43:72-8. Bickel WK, Stitzer ML, Bigelow GE, Liebson IA, Jasinski DR, Johnson RE. Buprenorphine: dose-related blockade of opioid challenge effects in opioid dependent humans. J Phannacol Exp Ther 1988;247:47-53. Pickworth et al. 575 Johnson RE, Cone El, Henningfield JE, Fudala PJ. Use of buprenorphine in the treatment of opiate addiction. I. Physiologic and behavioral effects during a rapid dose induction. CLIN PHARMACOL THER 1989;46:335-43. Fudala PJ, Jaffe JH, Dax EM, Johnson RE. Use of buprenorphine in the treatment of opioid addiction. II. Physiologic and behavioral effects of daily and alternate-day administration and abrupt withdrawal. CLIN PHARMACOL THER 1990;47:525-34. Johnson RE, Jaffe JH, Fudala PJ. A controlled trial of buprenorphine treatment for opioid dependence. JAMA 1992;267:2750-5. Harper I. Temgesic abuse. NZ Med J 1983;777. Rainey HB. Abuse of buprenorphine. NZ Med J 1986;72. O'Connor JJ, Moloney E, Travers R, Campbell A. Buprenorphine abuse among opiate addicts. Br J Addict 1988;83:1085-7. Richert S, Strauss A, von Arnim T, Vogel P, Zech A. Medilcamentenabhangigkeit von buprenorphin. MMW 1983;125:1195-8. Robertson JR, Bucknall ABV. Buprenorphine: dangerous drug or overlooked therapy. Br Med J 1986;292: 1465. Quigley AJ, Bredemeyer DE, Seow SS. A case of buprenorphine abuse. Med J Aust 1984;140:425-6. Sakol MS, Stark C, Sykes R. Buprenorphine and temazepam abuse by drug takers in Glasgow-an increase [Letter]. Br J Addict 1989;84:439-41. Gray RF, Ferry A, Jauhar P. Emergence of buprenorphine dependence. Br J Addict 1989;84:1373-4. Marquardt WG, Martin WR, Jasinski DR. The use of the Polaroid CU camera in pupillography. Int J Addict 1967;2:301-4. Fraser HF, Van Horn GD, Martin WR, Wolbach AB, Isbell H. Methods of evaluating addiction liability. (A) Attitude of opiate addicts toward opiate-like drugs, (B) a short term direct addiction test. J Pharmacol Exp Ther 1961;133:371-87. Jasinski DR. Assessment of the abuse potentiality of morphine-like drugs (methods used in man). In: Martin WR, ed. Handbook of experimental pharmacology: drug addiction I, morphine, sedative-hypnotic and alcohol dependence. Heidelberg: Springer-Verlag, 1977: 197-258. Heishman Si, Huestis MA, Henningfield JE, Cone EL Acute and residual effects of marijuana: profiles of plasma THC levels, physiologic, subjective, and performance measures. Phannacol Biochem Behav 1990; 37:561-5. Jasinski DR, Preston KL. Comparison of intravenously administered methadone, morphine and heroin. Drug Alcohol Depend 1986;17:301-10. Jasinski DR, Martin WR, Hoeldtke R. Studies of the dependence producing properties of GPA-1657, profadol and propiram in man. CLIN PHARMACOL THER 1971;12:613-49. 576 CLINICAL PHARMACOLOGY & THERAPEUTICS Pickworth et al. Walsh SL, Preston KL, Stitzer ML, Bigelow GE, Liebson IA. The acute effects of high dose buprenorphine in nondependent humans. In: Harris L, ed. Problems of drug dependence 1991. NIDA Research Monograph 119;1992:245. Mello NK, Mendelson JH, Kuehnle JC. Buprenorphine effects on human heroin self-administration: an operant analysis. J Phannacol Exp Ther 1982;223:30-9. Weinhold LL, Preston KL, Farre M, Liebson IA, Bigelow GE. Buprenorphine alone and in combination with naloxone in non-dependent humans. Drug Alcohol Depend 1992;30:263-74. Gal TJ. Naloxone reversal of buprenorphine-induced respiratory depression. CLIN PHARMACOL THER 1989;45: 66-71. Budd K. High dose buprenorphine for postoperative analgesia. Anesthesia 1981;36:900-3. MAY 1993 Pickworth WB, Bunker E, Welch P, Cone E. Intravenous buprenorphine reduces pupil size and the light reflex in humans. Life Sci 1991;49:129-38. Pickworth WB, Lee H, Fudala PJ. Buprenorphineinduced pupillary effects in human volunteers. Life Sci 1990;47:1269-77. Kareti S. Moreton JE, Khazan N. Effects of buprenorphine, a new narcotic agonist-antagonist analgesic on the EEG, power spectrum and behavior of the rat. Neuropharmacology 1980;19:195-201. Leander JD. Opioid agonist and antagonist behavioral effects of buprenorphine. Br J Pharmacol 1983;78:60715. Preston KL, Bigelow GE, Liebson IA. Buprenorphine and naloxone alone and in combination in opioiddependent humans. Psychophannacology 1988;94:48490. Bound volumes available to subscribers Bound volumes of CLINICAL PHARMACOLOGY & THERAPEUTICS are available to subscribers (only) for the 1993 issues from the Publisher, at a cost of $52.50 for domestic, $69.18 for Canadian, and $65.50 for international subscribers for Vol. 53 (January-June) and Vol. 54 (July-December). Shipping charges are included. Each bound volume contains a subject and author index and all advertising is removed. Copies are shipped within 60 days after publication of the last issue of the volume. The binding is durable buckram with the journal name, volume number, and year stamped in gold on the spine. Payment must accompany all orders. Contact Mosby, Subscription Services, 11830 Westline Industrial Drive, St. Louis, MO 63146-3318, USA; phone (800)453-4351, or (314)453-4351. Subscriptions must be in force to qualify. Bound volumes are not available in place of a regular journal subscription.