Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Special needs dentistry wikipedia , lookup
Focal infection theory wikipedia , lookup
Dental implant wikipedia , lookup
Remineralisation of teeth wikipedia , lookup
Scaling and root planing wikipedia , lookup
Impacted wisdom teeth wikipedia , lookup
Periodontal disease wikipedia , lookup
Tooth whitening wikipedia , lookup
Endodontic therapy wikipedia , lookup
Dental anatomy wikipedia , lookup
Crown (dentistry) wikipedia , lookup
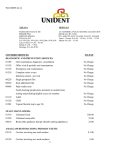
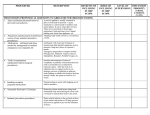
SCHEDULE OF BENEFITS Benefits provided by SafeGuard Health Plans, Inc., a MetLife company Self-Referral Dental Plan Univ II This Schedule of Benefits lists the services available to you under your SafeGuard plan, as well as the copayments associated with each service. There are other factors that impact how your plan works and those are included here in the Exclusions & Limitations. We have added some dental terminology definitions to help you better understand your plan – these can be found at the back of this Schedule. SafeGuard is an affiliate of MetLife. The following co-payments apply only when services are performed by your selected SafeGuard general dentist. SafeGuard also contracts with dentists who provide specialty care services (periodontics, oral surgery, endodontics, pedodontics, orthodontics). If you choose to receive care from one of these contracted specialists, your co-payment will be 75% of the specialist’s usual treatment fee. A list of Safeguard contracted general and specialty care dentists may be found online at www.safeguard.net (“Directories”). Code Service Diagnostic Treatment D0120 Periodic oral evaluation D0140 Limited oral evaluation - problem focused Oral Evaluation for a patient under three years of age and counseling with D0145 primary caregiver D0150 Comprehensive oral evaluation - new or established patient D0171 Re-evaluation – post-operative office visit D0180 Comprehensive periodontal evaluation - new or established patient Office visit - per visit (including all fees for sterilization and/or infection control) Radiographs / Diagnostic Imaging D0210 Intraoral - complete series of radiographic images D0220 Intraoral - periapical first radiographic image D0230 Intraoral - periapical each additional radiographic image D0240 Intraoral - occlusal radiographic image D0270 Bitewing - single radiographic image (once per year) D0272 Bitewings - two radiographic images (once per year) S0272 D0273 D0273 D0274 D0274 D0321 D0330 D0330 D0340 D0350 UNIVII-SOB Bitewings – two radiographic images (additional pair per year) Bitewings- three radiographic images (once per year) Bitewings – three radiographic images (additional pair per year) Bitewings - four radiographic images (once per year) Bitewings – four radiographic images (additional pair per year) Other temporomandibular joint radiographic images, by report Panoramic radiographic image Panoramic radiographic image (each additional) 2D cephalometric radiographic image – acquisition, measurement and analysis 2D oral/facial photographic image obtained intra-orally or extra-orally Customer Service (800) 880-1800 Co-payment $0 $20 $0 $0 $0 $50 $5 $0 $0 $5 $10 $0 $0 $12 $0 $18 $0 $20 $0 $0 $40 $34 $0 01/16 Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. SCHEDULE OF BENEFITS (continued) Code Service Co-payment Tests and Examinations D0415 Collection of microorganisms for culture and sensitivity D0425 Caries susceptibility tests D0460 Pulp vitality tests D0470 Diagnostic casts Preventive Services D1110 Prophylaxis – adult (twice per year) Prophylaxis –adult (each additional) Note: Routine cleaning does not apply to patients diagnosed with periodontal disease. D1120 Prophylaxis – child (twice per year) Prophylaxis – child (each additional) D1206 D1208 D1320 D1330 D1351 D1510 D1515 D1520 D1525 D1550 Topical application of fluoride varnish Topical application of fluoride – excluding varnish Tobacco counseling for the control and prevention of oral disease Oral hygiene instructions Sealant - per tooth Space maintainer - fixed – unilateral** Space maintainer - fixed – bilateral** Space maintainer - removable – unilateral** Space maintainer - removable – bilateral** Re-cement or re-bond space maintainer D1555 Removal of fixed space maintainer Restorative Treatment D2140 Amalgam - one surface, primary or permanent D2150 Amalgam - two surfaces, primary or permanent D2160 Amalgam - three surfaces, primary or permanent D2161 Amalgam - four or more surfaces, primary or permanent D2330 Resin-based composite - one surface, anterior D2331 Resin-based composite - two surfaces, anterior D2332 Resin-based composite - three surfaces, anterior D2335 Resin-based composite - four or more surfaces or involving incisal angle (anterior) Crowns D2740 Crown - porcelain/ceramic substrate** D2750 Crown - porcelain fused to high noble metal** D2751 Crown - porcelain fused to predominantly base metal** D2752 Crown - porcelain fused to noble metal** D2790 Crown - full cast high noble metal** D2791 Crown - full cast predominantly base metal** D2792 Crown - full cast noble metal** D2794 Crown – titanium D2910 Re-cement or re-bond inlay, onlay, veneer or partial coverage restoration UNIVII-SOB $0 $0 $10 $28 $0 $35 $0 $25 $0 $0 $0 $0 $18 $100 $146 $125 $171 $25 $25 $45 $55 $65 $80 $55 $70 $85 $100 $450 $409 $386 $389 $398 $359 $363 $398 $21 Customer Service (800) 880-1800 Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. SCHEDULE OF BENEFITS (continued) Code Service Co-payment D2915 Re-cement or re-bond indirectly fabricated or prefabricated post and core D2920 Re-cement or re-bond crown D2930 Prefabricated stainless steel crown - primary tooth D2931 Prefabricated stainless steel crown - permanent tooth D2940 Protective restoration D2950 Core buildup, including any pins when required D2951 Pin retention - per tooth, in addition to restoration D2952 Cast post and core in addition to crown** D2954 Prefabricated post and core in addition to crown** D2960 Labial veneer (resin laminate) - chairside D2961 Labial veneer (resin laminate) – laboratory** D2962 Labial veneer (porcelain laminate) – laboratory** Endodontics D3110 Pulp cap - direct (excluding final restoration) D3120 Pulp cap - indirect (excluding final restoration) D3220 Therapeutic pulpotomy (excluding final restoration) - removal of pulp coronal to the dentinocemental junction and application of medicament D3310 Endodontic therapy, anterior tooth (excluding final restoration) D3320 Endodontic therapy, bicuspid tooth (excluding final restoration) D3330 Endodontic therapy, molar (excluding final restoration) D3332 Incomplete endodontic therapy; inoperable, unrestorable or fractured tooth D3351 Apexification/recalcification – initial visit (apical closure / calcific repair of perforations, root resorption, etc.) D3352 Apexification/recalcification – interim medication replacement D3353 Apexification/recalcification - final visit (includes completed root canal therapy apical closure/calcific repair of perforations, root resorption, etc.) D3410 Apicoectomy – anterior D3421 Apicoectomy – bicuspid (first root) D3425 Apicoectomy – molar (first root) D3426 Apicoectomy (each additional root) D3430 Retrograde filling - per root D3450 Root amputation - per root D3460 Endodontic endosseous implant D3920 Hemisection (including any root removal) not including root canal therapy D3950 Canal preparation and fitting of preformed dowel or post Periodontics D4210 Gingivectomy or gingivoplasty - four or more contiguous teeth or bounded teeth spaces per quadrant D4211 Gingivectomy or gingivoplasty - one to three contiguous teeth or bounded teeth spaces per quadrant D4240 Gingival flap procedure, including root planing - four or more contiguous teeth or bounded teeth spaces per quadrant D4241 Gingival flap procedure, including root planing - one to three contiguous teeth or bounded teeth spaces per quadrant D4245 Apically positioned flap UNIVII-SOB $21 $65 $85 $25 $26 $85 $0 $120 $101 $204 $250 $395 $16 $14 $44 $285 $325 $450 $285 $285 $150 $150 $295 $295 $295 $270 $92 $250 $738 $170 $77 $139 $104 $191 $143 $225 Customer Service (800) 880-1800 Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. SCHEDULE OF BENEFITS (continued) Code Service Co-payment D4260 Osseous surgery (including elevation of a full thickness flap and closure) – four or more contiguous teeth or tooth bounded spaces per quadrant D4261 Osseous surgery (including elevation of a full thickness flap and closure) – one to three contiguous teeth or tooth bounded spaces per quadrant D4263 Bone replacement graft - first site in quadrant D4270 Pedicle soft tissue graft procedure D4320 Provisional splinting – intracoronal D4321 Provisional splinting – extracoronal D4341 Periodontal scaling and root planing - four or more teeth per quadrant D4342 Periodontal scaling and root planing - one to three teeth per quadrant D4355 Full mouth debridement to enable comprehensive evaluation and diagnosis D4910 Periodontal maintenance (2 in a 12 month period) Removable Prosthodontics D5110 Complete denture – maxillary** D5120 Complete denture – mandibular** D5130 Immediate denture – maxillary** D5140 Immediate denture – mandibular** D5211 Maxillary partial denture - resin base (including any conventional clasps, rests and teeth)** D5212 Mandibular partial denture - resin base (including any conventional clasps, rests and teeth)** D5213 Maxillary partial denture - cast metal framework with resin denture bases (including any conventional clasps, rests and teeth)** D5214 Mandibular partial denture - cast metal framework with resin denture bases (including any conventional clasps, rests and teeth)** D5221 Immediate maxillary partial denture – resin base (including any conventional clasps, rests and teeth) D5222 Immediate mandibular partial denture – resin base (including any conventional clasps, rests and teeth) D5223 Immediate maxillary partial denture – cast metal framework with resin denture bases (including any conventional clasps, rests and teeth) D5224 Immediate mandibular partial denture – cast metal framework with resin denture bases (including any conventional clasps, rests and teeth) D5410 Adjust complete denture – maxillary D5411 Adjust complete denture – mandibular D5421 Adjust partial denture – maxillary D5422 Adjust partial denture – mandibular D5510 Repair broken complete denture base** D5520 Replace missing or broken teeth - complete denture(each tooth)** D5610 Repair resin denture base** D5620 Repair cast framework** D5630 Repair or replace broken clasp - per tooth** D5640 Replace broken teeth - per tooth** D5650 Add tooth to existing partial denture** D5660 Add clasp to existing partial denture - per tooth** D5730 Reline complete maxillary denture (chairside) UNIVII-SOB $357 $172 $169 $226 $72 $61 $90 $68 $69 $52 $485 $485 $515 $515 $420 $523 $552 $563 $420 $523 $552 $563 $0 $0 $0 $0 $45 $40 $47 $48 $40 $37 $58 $76 $75 Customer Service (800) 880-1800 Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. SCHEDULE OF BENEFITS (continued) Code Service Co-payment D5731 Reline complete mandibular denture (chairside) D5740 Reline maxillary partial denture (chairside) D5741 Reline mandibular partial denture (chairside) D5750 Reline complete maxillary denture (laboratory)** D5751 Reline complete mandibular denture (laboratory)** D5760 Reline maxillary partial denture (laboratory)** D5761 Reline mandibular partial denture (laboratory)** D5850 Tissue conditioning, maxillary D5851 Tissue conditioning, mandibular D6210 Pontic – cast high noble metal** D6211 Pontic - cast predominantly base metal** D6212 Pontic - cast noble metal** D6214 Pontic - titanium D6240 Pontic - porcelain fused to high noble metal** D6241 Pontic - porcelain fused to predominantly base metal** D6242 Pontic - porcelain fused to noble metal** D6250 Pontic - resin with high noble metal** D6251 Pontic - resin with predominantly base metal** D6252 Pontic - resin with noble metal** D6545 Retainer - cast metal for resin bonded fixed prosthesis** D6720 Retainer crown – resin with high noble metal D6721 Retainer crown – resin with predominantly base metal D6722 Retainer crown – resin with noble metal D6750 Retainer crown – porcelain fused to high noble metal D6751 Retainer crown – porcelain fused to predominantly base metal D6752 Retainer crown – porcelain fused to noble metal D6780 Retainer crown – ¾ cast high noble metal D6781 Retainer crown – ¾ cast predominantly base metal D6782 Retainer crown – ¾ cast noble metal D6790 Retainer crown – full cast high noble metal D6791 Retainer crown – full cast predominantly base metal D6792 Retainer crown – full cast noble metal D6794 Retainer crown – titanium D6930 Re-cement or re-bond fixed partial denture D6940 Stress breaker** D6950 Precision attachment** Oral Surgery D7140 Extraction - erupted tooth or exposed root (elevation and/or forceps removal) D7210 Surgical removal of erupted tooth requiring removal of bone and/or sectioning of tooth, and including elevation of mucoperiosteal flap if indicated D7220 Removal of impacted tooth - soft tissue D7230 Removal of impacted tooth - partially bony D7240 Removal of impacted tooth - completely bony UNIVII-SOB $75 $75 $75 $75 $75 $75 $75 $45 $45 $387 $351 $351 $392 $392 $375 $375 $359 $331 $347 $137 $391 $383 $387 $402 $379 $379 $389 $389 $389 $382 $353 $354 $382 $40 $114 $201 $65 $102 $112 $140 $175 Customer Service (800) 880-1800 Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. SCHEDULE OF BENEFITS (continued) Code Service D7250 D7260 D7270 D7280 D7285 D7286 D7290 D7310 D7311 Surgical removal of residual tooth roots (cutting procedure) Oroantral fistula closure Tooth reimplantation and/or stabilization of accidentally evulsed or displaced tooth Surgical access of an impacted unerupted tooth Incisional biopsy of oral tissue – hard (bone, tooth) ( Incisional biopsy of oral tissue – soft** Surgical repositioning of teeth Alveoloplasty in conjunction with extractions - per quadrant Alveoloplasty in conjunction with extractions - one to three teeth or tooth spaces, per quadrant Alveoloplasty not in conjunction with extractions - per quadrant Alveoloplasty not in conjunction with extractions - one to three teeth or tooth spaces, per quadrant Vestibuloplasty – ridge extension (secondary epithelialization) Excision of benign lesion up to 1.25 cm Excision of benign lesion greather than 1.25 cm Excision of benign lesion, complicated Removal of benign odontogenic cyst or tumor – lesion diameter up to 1.25 cm Removal of benign odontogenic cyst or tumor – lesion diameter greater than 1.25 cm Removal of benign nonodontogenic cyst or tumor – lesion diameter up to 1.25 cm Removal of benign nonodontogenic cyst or tumor – lesion diameter greater than 1.25 cm Destruction of lesion(s) by physical or chemical method, by report Removal of lateral exostosis (maxilla or mandible) Removal of torus palatinus Removal of torus mandibularis Incision and drainage of abscess - intraoral soft tissue Incision and drainage of abscess - intraoral soft tissue - complicated(includes drainage of multiple fascial spaces) Incision and drainage of abscess - extraoral soft tissue Incision and drainage of abscess - extraoral soft tissue - complicated(includes drainage of multiple fascial spaces) Removal of reaction producing foreign bodies, musculoskeletal system Partial ostectomy/sequestrectomy for removal of non-vital bone Aleveolus – closed reduction, may include stabilization of teeth Occlusal orthotic device, by report Osteoplasy – for orthognathic deformities Osseus, osteoperiosteal, or cartilage graft of the mandible or maxilla – autogenous or nonautogenous, by report Frenulectomy – aka frenectomy or frenotomy – separate procedure not incidental to another procedure Frenuloplasty Excision of hyperplastic tissue - per arch Excision of pericoronal gingival D7320 D7321 D7340 D7410 D7411 D7412 D7450 D7451 D7460 D7461 D7465 D7471 D7472 D7473 D7510 D7511 D7520 D7521 D7540 D7550 D7670 D7880 D7940 D7950 D7960 D7963 D7970 D7971 UNIVII-SOB Co-payment $90 $250 $80 $138 $91 $81 $75 $73 $30 $110 $45 $136 $126 $254 $153 $105 $347 $120 $191 $62 $146 $146 $146 $40 $40 $54 $54 $79 $116 $292 $126 $2,300 $607 $103 $103 $82 $52 Customer Service (800) 880-1800 Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. SCHEDULE OF BENEFITS (continued) Code Service Co-payment Adjunctive General Services D9110 Palliative (emergency) treatment of dental pain - minor procedure D9120 Fixed partial denture sectioning D9215 Local anesthesia in conjunction with operative or surgical procedures D9219 Evaluation for deep sedation or general anesthesia D9230 Inhalation of nitrous oxide/analgesia, anxiolysis D9243 Intravenous moderate (conscious) sedation/analgesia – each 15 minute increment D9310 Consultation (diagnostic service provided by dentist other than practitioner providing treatment) D9420 Hospital call D9430 Office visit for observation (during regularly scheduled hours) -no other services performed D9440 Office visit - after regularly scheduled hours D9450 Case presentation, detailed and extensive treatment planning D9610 Therapeutic drug injection, by report D9612 Therapeutic parental drugs, two or more administrations, different medications D9630 Other drugs and/or medicaments, by report D9910 Application of desensitizing medicament D9950 Occlusal analysis – mounted case D9951 Occlusal adjustment - limited D9952 Occlusal adjustment - complete D9972 External bleaching - per arch – performed in office D9974 Internal bleaching – per tooth D9986 Missed appointment (less than 24-hr notice) D9987 Cancelled appointment (if less than 24-hr notice, see D9986) $25 $0 $0 $0 $25 $60 $0 $75 $0 $35 $0 $25 $40 $15 $15 $48 $25 $125 $200 $40 Not to exceed $25 $0 Current Dental Terminology © American Dental Association UNIVII-SOB Customer Service (800) 880-1800 Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. Dental Terminology Definitions These definitions are designed to give you a “layman’s understanding” of some dental terminology in order for you to better understand your plan; they are not full descriptions. Amalgam: A silver filling Anterior: Teeth that are in the front of the mouth Bicuspid: Most people have eight bicuspid teeth; they are located immediately preceding the molar teeth with two in each quadrant of the mouth. Bridge: A replacement for one or more missing teeth that is permanently attached to the teeth adjacent to the empty space(s). Crown: A covering created to place over a tooth to strengthen and/or replace tooth structure. A crown can be made of different materials (noble, high noble), base metal, porcelain or porcelain and metal. Endodontics: Procedures that treat the nerve or the pulp of the tooth due to injury or infection. Oral Surgery: Surgery to remove teeth, reshape portions of the bone in the mouth, or biopsy suspect areas of the mouth. Orthodontics: Braces and other procedures to straighten the teeth. Periodontics: Procedures related to treatment of the supporting structures of the teeth (gums, underlying bone). Posterior: Teeth that set towards the back of the mouth, including molars and bicuspids (premolars). Primary Teeth: The first set of teeth (“baby” teeth). Prophylaxis: Scaling and polishing of teeth by removal of the plaque above the gum line. Prosthodontics: The restoration of natural and/or the replacement of missing teeth with artificial substitutes. Quadrant: One of the four equal sections into which your mouth can be divided (some procedures like periodontics are done in quadrants). Resin-based Composite: UNIVII-SOB Tooth-colored (white) fillings. Customer Service (800) 880-1800 Exclusions and Limitations Exclusions SafeGuard does not provide coverage for the following services: 1. Services which, in the opinion of the contracted general dentist or specialist, are not necessary for the patient’s dental health, except those procedures listed on the co-payment schedule classified as cosmetic procedures. 2. Cost of hospitalization, pharmaceuticals and general anesthesia. 3. Any services performed by a non-contracted general dentist or specialist. 4. Services that cannot be performed because of the general health condition of the patient. 5. Treatment which, in the opinion of the general contacted dentist, must be performed by a noncontracted specialist. 6. Any services which are not consistent with the usual and customary services provided by the general contracted dentist. 7. Services for injuries or conditions that are covered under Workers’ Compensation or Employer Liability Laws. 8. Services provided without cost to any subscriber or member by any municipality, county, or other political subdivision, or because of injury arising out of, or in the course of work for wage or profit. 9. Services which, in the opinion of the general contracted dentist or specialist, are not necessary for the subscriber’s or member’s health or cannot be performed due to the general health condition of the subscriber or member. 10. Cost of dental care, which is covered under automobile, medical, no-fault or similar type of insurance. 11. Services for injuries or conditions resulting from military service or any act of war, declared or undeclared. 12. Experimental dental care, implantology (except those covered services listed in the Schedule of Benefits), or dental care which is not generally accepted by the American Dental Association or the Academy of General Dentistry. 13. Cost of hospitalization or inpatient services for any dental procedure. 14. Dispensing of drugs or medications (except oral anesthesia). 15. Oral surgery requiring setting of fractures or dislocations. 16. Procedurees performed before a person becomes a subscriber or member. 17. Procedures not contained within the Plan’s Schedule of Benefits. 18. Dental services received from a non-contracted general dentist or non-contracted specialist. 19. Treatment of cysts (except those covered services listed on the Schedule of Benefits), neoplasms and malignancies. Limitations 1. Cleanings (prophylaxis) and fluoride treatments are limited to two (2) per 12 months. Additional cleanings (prophylaxis) are available at the co-payment listed on this Plan’s Schedule of Benefits. 2. Periodontal maintenance procedures (following active periodontal therapy) are limited to 2 in a 12month period. 3. Full-mouth x-rays are limited to once every 3 years. Panoramic x-rays are limited to once every 3 years. Additional panoramic x-rays are available at the co-payment listed on this Plan’s Schedule of Benefits. 4. Bitewings are limited to once every 12 months. Additional films are available once per 12 months at the co-payment listed on this Plan’s Schedule of Benefits. 5. Members are responsible for additional lab fees for services designated with two asterisks (**). Lab fees shall not exceed $100 for each procedure. If porcelain, noble, high noble or any other metal is used, the cost is included in the co-payment. 6. Broken appointment without 24 hour notice – per 15 minute unit – maximum $40. UNIVII-SOB Customer Service (800) 880-1800