Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
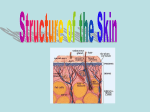
INTRO TO DERMATOLOGY [Dermatology - Study of the skin, hair, glands, nails Dermatologist - specialist of the skin -Calcitriol: important in production of calcium, phosphorous in small intestine, bone development -I missed the first couple lines, but I have most if not all of the rest…] -Epidermis - outermost, no blood vessels or blood supply -New layer produced every 30 days -Waterproof, functions as barrier to microorganisms -Dermis - vascular layer/sensation. Strength and elasticity to the skin. -Does not regenerate -Scar: fibrous tissue that replaces normal tissue after dermis has been destructed -No sweat glands, no hair follicles -Located below epidermis -Hypodermis - subcutaneous layer - protects bone, tendon, muscles -Helps attach the skin to muscles below -Insulation, protection, energy source -Accessory structures: hair, nails, glands EPIDERMIS -Stratum corneum - outermost layer -15-30 layers of flattened dead keratinized cells -Tightly connected by desmosomes -Sheds 40 lbs over a human lifetime -Stratum lucidum - only found in palms and soles -Thin layer of flat cells, present in thick skin -Helps reduce friction protection -Stratum granulosum - few layers of flattened cells containing keratohyalin -Produce keratin, release lipids (water resistance) -Stratum spinosum - formed as basal layer moves outward towards surface -2-4 cell layers thick, has desmosomes (have spiny projections) -Langerhan cells -- important for immunity -Keratinocytes -- produce keratin -Stratum basale - deepest layer of the epidermis -Single layer of keratinocytes and melanocytes -Produce melanin -Covers basement membrane (basal lamina) - separates epidermis from dermis -Undergo rapid cell division to produce more cells Californians Like Girls In String Bikinis Melanocytes - produce melanin, not many in soles or palms of hands -Albinos lack tyrosinase - enzyme required to make melanin -Cancer of melanocyte = melanoma, fast metastasizing Keratinocytes - produce keratin -Secrets cytokines and inflammatory mediators -Protection and waterproofing Merkel’s cells - touch receptors found in fingers, toes, mouth -Free nerve endings attached to epidermal cells Langerhans cells - derived from bone marrow, involved in hypersensitivity, antigen processing, etc Parakeratosis - retention of nuclei in stratum corneum (usually dead) -Hypertrophy of the corneum (hyperkeratosis) -Flaky, scaly skin Spongiosis - intercellular edema of the epidermis - leads to inflammation -Physically pulls epidermis away from each other - intraepidermal vesicles (contact dermatitis, eczema) Basal lamina (Basement membrane) -Separates dermis from epidermis -Allows epidermis to adhere to dermis -Selectively filters molecules moving bt two layers, prevents malignant cells from moving any deeper -Blister formation from immunoglobulin and complement deposition DERMIS -Thickest skin layer/connective tissue layer -Separates epidermis from subcutaneous fat layer -Strong, flexible -Composed of collagen, blood vessels, nerves, ,hair follicles, sweat glands -Provides nutrition -Thermoregulation, protection SUBCUTANEOUS TISSUE -Fat, blood vessels -Eccrine glands and deep hair follicles extend to this layer -Important insulator, shock absorber, stores energy HAIR -Associated with sebaceous gland pilosebaceous unit -No new hair follicles after birth, some need hormonal stimulation -Made of keratin -Growth is cyclic -Anagen - 90% of hair follicles undergo growth -Catagen- hair falls out, new hair begins to grow -Telogen - resting phase (10% of time) Hair loss due to-Stress, poor nutrition, genetics, hormones, pregnancy, medications NAILS -Hardened keratinized plates - dead cells -Grow under the lunula (white portion on bottom of nailbed) -Protection, dexterity -Grow continuously bc they are continuously produced (keratin) GLANDS Sebaceous - Entire skin surface except palms, soles, sides of feet, secrete sebum -Sebum: lipids, cholesterol, wax -Mildly bactericidal, lubricates -Influenced by hormones, adolescence Sweat - found in hands, soles, axillae -eccrine - originate in dermis and open on skin surface -apocrine - large deep in dermal layer, secrete oily substance -mixed with bacteria = body odor -odor can also be caused by fat and protein and sweat decompose SKIN LESIONS EQUAL TO PLANE OF SKIN Macule - circumscribed, round, up to 1 cm in diameter, flat, distinguished from surrounding skin by color - freckles Patch - large macule greater than 1 cm in diameter, flat Telangiectasia - spider veins - dilated superficial blood vessels (found in scleroderma, cirrhosis) Petechiae - small, non-blanching erythematous macules <2mm in diameter, pinhead size, due to rupture of small blood vessels which lead to minor hemorrhage (don’t go away when you press on it) - sign of thrombocytopenia - low platelet count Purpura - >2mm, large petechiae discoloration of skin, mucous membrane due to hemorrhage, non-blanching, reddish discoloration -Ecchymosis - blueish discoloration, deeper bleeding in skin Sclerosis - hardening, immobility of affected skin (induration) Lichenification - focal area of thickened skin with accentuation of skin markings (skin lines) due to repeated rubbing or scratching in a susceptible patient (ie patients with eczema) Acanthosis - thickening of epidermis on neck, under the arms, in groin area, due to elevated levels of insulin (activate receptors in skin), proliferation of keratinocytes (parakeratosis) ABOVE PLANE Actinic Keratosis - rough, raised spot on skin, found on skin chronically exposed to the sun (precancerous) - can appear light, dark, pink or red in color Hyperkeratosis - hypertrophy of stratum corneum - excessive keratin being produced Callus - thickening and enlargement of stratum corneum (hyperkeratosis leads to callus) Corn - small callused area caused by local pressure, irritating tissue over a bony prominence Papule - well circumscribed, elevated solid lesion up to about 1cm in diameter, usually dome shaped Nodule - palpable solid region that can involve the epidermis, dermis, subQ layer; can be due to neoplasm, usually bt .5 - 2 cm in diameter, deeper in skin than papule Wheal - transient, pink/red raised area with central pallor; shape and size of wheals vary (hives, mosquito bites) Plaque - elevated, flat-topped area, usually >1cm in diameter, rarely >5mm in height Vesicle - raised, contain serous fluid, usually 1 cm or less in diameter Bulla - large vesicle, >1cm Pustule - discrete pus-filled raised area (acne, folliculitis) filled with leukocytes or dead cellular material Cyst - elevated, encapsulated mass, can be semi-solid or fluid filled, epithelial lined, contains fluid or semi-solid material inside Tumor - Well demarcated (can tell borders around it), usually >2cm in diameter (increasing size: papule --> nodule --> tumor) Verruca - epidermal growth due to a virus - wart Scale/crust - flakes of the stratum corneum; can be large membrane or tiny (like dust), can adhere to skin (scab) or can be loose (dandruff in hair); white area = scaling; crust = dried serum, blood or pus on surface of skin Desquamation - peeling of the skin Exudate - fluid that has exuded from a tissue or capillary due to inflammation or injury; can be serum, blood or pus Comedone - enlarged hair follicles plugged with oil, bacteria (acne) - can be either whiteheads or blackheads BELOW PLANE OF SKIN Erosion - loss of the superficial layer of the upper epidermis by wearing away from friction or pressure Ulcer - indentation in skin - crater-like; circumscribed area of skin loss extending through the epidermis through the dermis, subQ layer, may extend to muscle and bone (decubitus ulcers) Fissure - small crack or break in skin which exposes the dermis and appears erythemic (paper cut) Excoriation - traumatic self-induced lesion due to scratching; erythematous; makes pt prone to infection Eschar - thick, coagulated crust or slough which develops following a burn Disorders of Pigmentation and Melanocytes Vitiligo - Melanocytes are destroyed - leads to white patches on skin - possibly autoimmune disorder Albinism - have melanocytes but lack tyrosinase enzyme, melanin cannot be produced - no protection from sun’s rays Melasma - mass-like zone of facial melanosis (hyperpigmentation) - known as chloasma in pregnancy Lentigo - melanocyte proliferation - small, circumscribed, pigmented macule surrounded by normal skin - can be due to hyperkeratosis, Addison’s disease, hemochromatosis; may be bleached by hydroquinone Skin Lesions Based on Color Erythema - redness due to capillary dilation, inflammation, cellulitis or sunburn -Blanches with pressure - intact capillaries Cyanosis - blueish discoloration usually due to hypoxia Jaundice - yellow staining of the skin due to bile pigments and increased levels in the plasma Approach to pt Normal vs. abnormal Appropriate differential diagnosis Pros of dermatology - visual, no special instrumentation, easy biopsy Cons of dermatology - easily misled by variety of stimuli and overall look of disease -- subtle Hx Acute vs. chronic Onset - when/how it started Subjective symptoms - does it hurt/itch/burn/etc Location - where it started Distribution - where is it? - generalized, specific Spread, change in lesions - chicken pox, herpes zoster What makes it worse/better Has there been contact with anyone with a similar rash? Did you get a new pet? Recent travel? Physical Exam FOUR points: Type of Lesion Shape Arrangement Distribution Palpate lesions - are they consistent? Tender? Temperature change? Mobility? Margins? Systemic exam: lymphadenopathy (bacterial infection, elephantitis), organomegaly, jaundice, arthralgia, neurological changes Rash - temporary eruption of the skin seen in childhood disease, in heat, drug-induced, diaper rash, etc Lesion - break in tissue integrity, continuity - pathological or traumatic change in tissue Shape of the lesion -Round -Oval -Polygonal -Annular - circular, ring shaped -Serpenginious - snakelike -Umbilicated - indentation in the middle Arrangement of lesions -Grouped - herpetiform (like herpes), arciform (in an arc), annular (ring shaped), reticulated (web) -Disseminated - widely scattered, discretely with borders; can be either discrete or diffuse (cannot tell where borders end) -Demarcated - (may or may not be discrete) have clear boundaries - each individual lesion is pointed out -Diffuse - no clear boundaries - opposite of demarcated Extent: isolated, localized, regional, generalized, universal Pattern: symmetrical, exposed areas (substance, sun), pressure related (heels), random -Any characteristic patterns such as seen in acne, chicken pox Darier sign - rubbing on lesion leads to wheal or flare Auspitz sign - pinpoint bleeding after scales are removed - common in psoriasis Nikolsky sign - slight rubbing causes separation of the skin layers (desquamation) Diascopy - putting a glass slide against the skin - blanching = capillaries are intact (ie suburn); non-blanching = capillaries broken Koebner phenomenon - minor scratching leads to lesions Diagnostic Techniques Wood Light Exam: Use ultraviolet light -Some organisms turn colors under light -Green fluorescence in tinea capitis -Skin: erythrasma (chronic bilateral infection caused by cornybacteria): bacteria give coral red fluorescence -Hypomelanosis: decrease in intensity Acetowhitening: acetic acid allows a transient whitening of penile or vulvar (genital) warts Patch test: for allergies - hypersensitivity test where pt is pricked with diff allergens to see where they produce a response KOH preparation: dissolves keratin and cellular material, does not affect fungi (tinea capitis) For bacteria: gram stain For virus: Tzanck smear For spirochetes: dark field examination - spirochetes appear bright spiral objects against black background Cultures: used for bacterial, viral, parasitic, mycologic Biopsy: used for diagnosis