Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
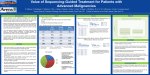
Feasibility Study of Genomic Biomarker Profiling for Patients with Metastatic Colorectal Cancer Bradley L. Smith1, Philip Breitfeld1, Jennifer Cubino1, Victor Weigman1, Donald P. Richards2, Ki Y. Chung3.1 1 Quintiles, Durham, NC; 2 Texas Oncology - Tyler, TX; 3 Cancer Center of the Carolinas, Spartanburg, SC Abstract Background: The adoption of Next-Generation Sequencing (NGS) platforms AmpliSeq Cancer Hotspot Panel v2 assay, enriching for hotspots within 50 cancer- therapies in other indications. 84.3% of patients had variant associated with open and development of targeted oncology drugs have enabled matching of patients related genes. Clinical annotation and reporting to the doctors was provided by clinical trials. Of these 43 patients, 32 had multiple biomarkers with associated and drugs. The authors undertook an observational, clinical study to explore the N-of-One. Basic demographic and clinical information was collected but formal trials. Overall, more than 100 mutations were identified including alterations in feasibility and potential clinical benefits of an upfront approach to the genomic disease monitoring and follow-up was not performed. Clinicians were asked to KRAS, BRAF, EGFR, PIK3CA, GNAS, TP53, APC and other genes. The number profiling of tumors from metastatic colorectal cancer (mCRC) patients. The study report the impact of the genomic test report on patient recommendations. of actionable mutations was not associated with progressor status. Doctors sought to determine the number of drug targetable genomic changes, which Results: The study enrolled and profiled 51 stage IV mCRC patients from July recommended clinical trials following profiling and reporting of genomic alterations occur within mCRC patients including a comparison of patients who progress early 2013 to October 2013 from 14 sites in the U.S.; one additional patient was enrolled in 15 out of the 43 patients (35%) that had actionable mutations. over the targeted number. Subjects were stratified by time to progression prior to Conclusions: The outcome of this observational study demonstrates the Methods: The study targeted enrollment of 50 mCRC patients within the U.S. entering the study. The study population was evenly distributed across early feasibility of rapid screening and reporting of NGS genomic results targeting Oncology Network followed by collection of archival formalin-fixed paraffin (<1 yr) and late progressors (>1 yr) with a median age of 62. Test turn-around time actionable mutations in mCRC. The lack of an association between early and late embedded (FFPE) samples and genomic testing. Sample collection and averaged 15 days. 98% of the bases sequenced in the genomic analysis reached progressors, suggests that a greater sample size will be required for future studies. processing was performed at Quintiles Central Laboratories followed by testing and the target coverage necessary to identify 5% variant frequency in the sample. The reported impact on clinician recommendations indicates the value of the bioinformatic analysis at the Quintiles EA Genomic Laboratory. Genomic profiling Genomic variants associated with approved therapies in mCRC were observed results to inform treatment and clinical trial decisions. was performed on the Ion Torrent PGM following enrichment of tumor DNA via the in 7.8% of patients while 64.7% of patients had variants associated with approved versus late. Background Introduction • Cancer genomics is moving into practice driven by the increased molecular complexity of cancer and drugs that target those genomic alterations. • Explosion of targeted agents in cancer; 22% of the pipeline agents currently in pivotal trials are being developed in a biomarker-defined patient population. Potential solution: • Remove barriers to patient participation in clinical trials: multiplex testing allows for efficient use of scarce tumor samples and rapid testing of the sample ensures patients are not delayed in receiving treatment. • Genomic profile patients to match study criteria prior to site startup. • Recent technical development of genomic platforms enables rapid and broad genomic profiling. • Clinically annotate and report results to clinician. Patient pre-profiling platform Summary: mCRC 50 patient trial with 50-gene NGS profiling and reporting to clinicians performed in collaboration with U.S. Oncology Research (USOR) Network The Challenge: efficient execution of programs targeting niche oncology populations with specific genomic alterations. Feasibility study to demonstrate pre-profiling operational platform • How do I cost-effectively develop a drug with an anticipated high screen failure rate in a timely fashion? Primary objective: •To determine the number of drug targetable genetic changes, which occur within patients with mCRC. The number of clinically actionable mutations with FDAapproved drugs will be compared to the number without FDA- approved drugs and to actionable mutations with associated clinical trials. Secondary objectives: •To determine the feasibility of collecting tumor samples and having those patients undergo tumor genomic analysis. •To investigate the number and cause of failed analyses after registration and tissue submission. •To determine if physicians took into consideration regimens that were suggested by the results of the sequencing analysis when deciding their patients’ next line of therapies. Operational results Pilot study description Ion Torrent PGM NGS Platform Introduction •50 genes; Hot Spot coverage (not total open reading frames) •2800 COSMIC mutations •~26kbp of captured sequence Study Characteristics • Total months of enrollment: Approx. 3 months (planned for 6 months) • Number of Sites: 14 (all within U.S. Oncology Research Network and the U.S.) • Sample type: FFPE archival slides or blocks • Total patients in Early (recurrence <1 year) Occurrence arm: 25 patients • Total patients in Late (recurrence after 1 year) Occurrence arm: 26 patients • Total patients diagnosis: 100% Stage IV Colorectal Cancer • Both recurrence and gender were distributed evenly across patient age groups • 80% of enrolled patients were Caucasian Performance •> 400X depth of coverage for ≥ 95% of the targeted regions •98.4% of samples in study were powered to identify alleles at ≥5% frequency (i.e. “callable bases”) • 10% of patients in this study had callable bases with between 90-95% coverage, potentially due to biological factors Genomic test turn-around-time (TAT) summary PGM - GENE LIST ABL1 EZH2 JAK3 PTEN AKT1 FBXW7 IDH2 PTPN11 ALK FGFR1 KDR RB1 APC FGFR2 KIT RET ATM FGFR3 KRAS SMAD4 BRAF FLT3 MET SMARCB1 CDH1 GNA11 MLH1 SMO CDKN2A GNAS MPL SRC CSF1R GNAQ NOTCH1 STK11 CTNNB1 HNF1A NPM1 TP53 EGFR HRAS NRAS VHL ERBB2 IDH1 PDGFRA ERBB4 JAK2 PIK3CA TAT summary: Min: 9 Days Max: 21 Days Avg: 15 Days Five samples were excluded due to prospective decision to re-sequence samples Genomic & clinical results Results of Genomic Analysis & Clinical Annotation Distribution of mutations in patient population Influence of genomic data on clinician decision making (3 categories of actionable genomic alterations) Approximately 3% of oncology patients participate in clinical trials in the U.S. The much higher percentage of patients informed of relevant trials in the preprofiling study suggests preprofiling may improve clinical trial participation. This may be due to: 1. Providing genomic data improves awareness and interest in trial options 2. Patients enrolled in pre-profiling were more likely to be eligible or interested in clinical trials than patients not enrolled in preprofiling Overall 100 mutations were observed, encompassing all 3 categories of action-ability including mutations in PIK3CA corresponding to open clinical studies. • Distribution of clinical recommendations and associated therapies or trials was similar across gender and age • Data provided by N-of-One • Number and distribution of mutations was similar between early and late progressors. • However, a few genes/mutations were primarily found in one group and not the other (BRAF, CDKN2). Summary Test / profiling feasibility and performance • High quality genomic data and a clinical report was delivered to doctors in a reasonable time (average 15 days from sample submission to report) utilizing archival FFPE samples • Rapid patient enrollment indicates clinician and patient excitement for this type of information Profiling results • Overall 100 mutations were observed, encompassing all 3 categories of action-ability • 60 distinctly different actionable alterations were observed in 43 out of the 51 total patients (84%) *Physicians response was limited to a single category **8/51 patient samples had no actionable mutations or clinical recommendations ***Physicians may have reported “not influenced” due to existing use of standard of care FDA approved drug consistent with preprofiling report Discussion • The most frequent actionable mutations had associated clinical trials, followed by therapeutics approved in other indications and therapeutics approved in CRC • The number of actionable mutations did not statistically correlate with patient demographics or progression status • Progression status did not statistically correlate with specific alterations although further investigation may be warranted Study impact • Genomic pre-profiling and the genomic report impacted clinician recommendations for available clinical trials in a significant percentage of cases that reported actionable mutations (15/43; 35%) • Patient pre-profiling may rapidly identify qualified patients for biomarker-driven oncology drug development • Pre-profiling may improve trial timelines by increasing the pool of patients participating and screened for clinical trials • Implementation of pre-profiling will require collaboration across key stakeholders including sponsors, CROs, clinicians and patients