Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
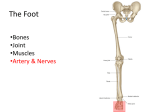
Anatomy Block 2 Test #2 Notes Bony Pelvis, Hip and Femur Hip joint o 3 main bones: ilium, ischium, pubis Ilium: superior “wing” Ischium: located inferior and posterior Pubis: located inferior and anterior o Acetabulum: socket in the hip where the head of the femur sits Has contributions from all three hip bones The three hip bones in the acetabulum are separated by the triradiate cartilage Lined with articular (lunate) cartilage Has a half-moon shape Gives rise to the labrum which in turn gives rise to the transverse acetabular ligament Also contains synovial membrane Structurally contains a labrum (like that seen in the shoulder) to help the stabilize the head of the femur in the acetabulum Labrum deepens the fossa where the femoral head sits o Is a ball-and-socket joint (but unlike you may think, it is quite stable) Allows for the following actions: Flexion: bring leg forward Extension: bring leg backward Abduction: bring leg out to the side Adduction: bring leg back to midline Circumduction: moving leg in a circle (clockwise or counter-clockwise) Medial rotation: rotating the leg inward (toward the midline) Lateral rotation: rotating the leg outward (away from the midline) o Contains a strong joint capsule Allows for support during motion and at rest Contains three intrinsic (deep) ligaments From strongest to weakest o Iliofemoral (two): connects the ilium to the femur o Ischiofemoral: connects ischium to femur o Pubofemoral: connects pubis to femur o Contains hyaline cartilage o Femoral fovea: point of attachment of the ligament of the head of the femur (on the femoral head); no articular cartilage at this location o Arterial supply to the hip joint: circumflex femoral arteries o Innervation at the hip joint: Femoral nerve Obturator nerve Superior gluteal nerves o Points of articulation at the hip joint: Acetabular (lunate) cartilage w/articular cartilage of the femoral head Remember no articular cartilage at the femoral fovea b/c this is where the ligament of the head of the femur attaches Note that the entire acetabulum is not lined w/articular cartilage There is a region at the bottom of the acetabulum that is cartilage-free; this is the location of the transverse acetabular ligament o Muscles of the hip joint: Iliopsoas: flexion Sartorius: flexion Tensor fascia latae: flexion, abduction, medial rotation Rectus femoris: flexion Pectineus: flexion, adduction Adductor longus: flexion, adduction, Adductor brevis: flexion, adduction Adductor magnus: flexion (anterior part), adduction, extensor (posterior part) Gracillus: flexion, adduction Obturator externus: adduction, lateral rotation Obturator internus: lateral rotation Gemelli: lateral rotation Piriformis: lateral rotation Quadratus femoris: lateral rotation Gluteus maximus: lateral rotation, extension Hamstrings (semitendinosus, semimembranosus, long head of biceps femoris): extension Gluteus medius: abduction, medial rotation (anterior part) Gluteus minimus: abduction, medial rotation (anterior part) Knee joint o Allows for the following motions: Flexion: bending the knee Extension: straightening the knee Moderate rotation o A “stable” joint w/2 mensici Meniscus: a cartilaginous hemi-disc that prevents bone on bone contact Serves as a shock absorber o Knee joint contains numerous intrinsic and extrinsic ligaments Fibular (lateral) collateral ligament Tibial (medial) collateral ligament Oblique popliteal ligament Arcuate popliteal ligament Patellar ligament o Anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) are designed to restrict anterior and posterior motion between the tibia and the femur Both are named for their attachment to the tibia Form a cross between the femur and tibia o Knee joint consists of three main bones: Tibia, femur, patella o Arterial supply to the knee: Genicular branches of the femoral, tibial and popliteal arteries o Nerves in the knee: Femoral nerve, tibial nerve, common fibular nerve o Knee also consists of an extensive network of bursa Bursae: fluid-filled synovial sac that serves as a cushion at points of boney contact o True knee joint is the articulation between the medial/lateral condyles of the femur with the medial and lateral condyles of the tibia Tibial plateau: superior surface of the tibia where the medial and lateral condyles of the tibia are situated Note that a synovial membrane immediately surrounds the tibial plateau and a joint capsule surrounds the synovial membrane Or put another way: inward to outward o Tibial plateau, synovial membrane, joint capsule o All muscles that cross the knee joint help to contribute to joint stability Ankle joint o Is a hinge joint Also referred to as a mortise joint Is relatively stable due to the abundance of ligaments o Borders of the ankle joint Tibia: roof, medial side Fibula: lateral side Talus: fits into the groove formed between the lateral malleolus (of the fibula) and the medial malleolus (of the tibia) Supported by the calcaneus o Movements at the ankle joint: Dorsiflexion: bring toes towards tibia Plantar flexion: point toes towards the ground Inversion: bring medial malleolus up Eversion: bring lateral malleolus up o Deltoid ligament (consists of 4 parts) Anterior tibiotalar ligament Tibionavicular ligament Tibiocalcaneal ligament Posterior tibiotalar ligament o Muscles that cross the ankle joint contribute to its stability o Contains a thin joint capsule both anteriorly and posteriorly Is reinforced medially and laterally by collateral ligaments o Arterial supply to the ankle: fibular and tibial arterial branches o Nerves in the ankle joint: tibial nerve, deep fibular nerve Feet o Bones of the foot Tarsal bones (ankle bones) Talus, calcaneus, cuboid, navicular, cuneiforms (lateral, middle, medial) o Talus consists of head, neck and body 5 metatarsals (#1 starts w/big toe) Phalanges: digits 2-5 have proximal, middle and distal Digit #1 (big toe) just has proximal and distal o Zones of the foot Hindfoot: calcaneus, talus Midfoot: cuboid, navicular, cuneiforms Forefoot: metatarsals, phalanges Transverse tarsal line separates the hindfoot from the midfoot Tarsometarsal line separates the midfoot from the forefoot o There are NUMEROUS joints in the foot Intertarsal, tarsal-metatarsal, metatarsal-phlangeal, interphalangeal o The foot is primarily composed of hinge joints Allows for plantar flexion and dorsiflexion These joints usually undergo little movement Exceptions: talocalcaneal, calcaneocuboid, talonavicular joints o Allows for inversion/eversion o Main ligaments in the foot (support the plantar arches) Plantar calcaneonavicular Long plantar Plantar calcaneocuboid o Toe joints are hinge joints Digits 2-5 contain a PIP and DIP Digit 1 has a single IP joint o Joint capsules in the feet are incredibly strong due to the stress your feet take in everyday o Arterial supply to the feet: Posterior tibial, fibular, lateral and medial tarsal arteries o Nerves to the feet: Medial and lateral plantar nerves, deep fibular nerve, digital nerves Review of joints o Joint: a point of articulation between bones Most are of the synovial type Contains a capsule, cartilage, synovial fluid, articular discs/menisci o Hilton’s Law: joints receive innervation due to branches of nerves that innervate the muscles that move the joint o Arteries that pass by a joint will provide blood to that joint w/large joints you have arterial anastomoses o venous drainage think “venae comitantes” Anterior and Medial Thigh Lower limb consists of 6 regions: o Gluteal (buttocks, hip), femoral (thigh), knee, leg (tibia,fibula), ankle, foot Somatic motor and general sensory innervation of the lower limb is provided via: o Lumbar plexus: Located on posterior abdominal wall and consists of anterior rami of L1-L4 o Sacral plexus: Located on the posterior pelvic wall and formed by anterior rami of L4-S3 o Remember rami (dorsal and ventral) come off from the spinal nerve and for the most part are mixed (have both sensory and motor) o Note: the lumbar plexus is SUPERIOR to the sacral plexus Lumbar plexus innervates anterior portion of lower limb Sacral plexus innervates posterior portion of lower limb Fascia lata: the deep fascia of the thigh o Gives rise to the lateral and medial intermuscular septa In turn forming the anterior and posterior osteofascial compartments (contains the musculature of the thigh) Technically there is also a medial compartment but it is not separated by fascial planes Fascia: the wrapping, packing and insulating material of the body o Deep fascia is thought to help facilitate/enhance muscle movement Compartments of the thigh o Each compartment contains muscles that perform similar functions Three compartments: anterior, posterior, medial o Blood supply to the lower limb: Aorta gives rise to the common iliac artery which becomes the external iliac artery which becomes the femoral artery It is the femoral artery that INDIRECTLY supplies the entire lower limb o Innervation to the compartments Anterior compartment: femoral nerve Posterior compartment: sciatic nerve Medial compartment: obturator nerve Anterior compartment of the thigh o Contains the anterior thigh muscles Divided into: Flexors of the hip Extensors of the knee o These muscles innervated by the femoral nerve EXCEPTION: psoas major and minor are innervated by the anterior rami of L1-L2 o Flexors of the hip (in the anterior compartment) Pectineus: located in the anterior, superomedial thigh flexion, adduction, lateral rotation is a transition point between the anterior and medial compartments o therefore it may sometimes be innervated by a branch of the obturator nerve Iliopsoas: Consists of iliacus, psoas major and minor Iliacus: originates on iliac fossa and inserts on lesser trochanter of femur Psoas major: originates on lumbar vertebrae and inserts on lesser trochanter of femur Psoas minor: originates on the lumbar vertebrae and inserts on the iliopubic ramus Chief flexor of the thigh o If thigh is fixed, allows flexion of the trunk Is an important postural muscle; stabilizes the trunk and helps to maintain normal lumbar lordosis Sartorius: Originates on ASIS and inserts on medial tibia Crosses both hip and knee Allows for cross-legged sitting position Acts as a synergist; keeps the knee in line Flexion (thigh), abduction, external rotation (thigh), medial rotation of tibia (if knee is bent) Hip flexion allows acceleration of the thigh needed for swing phase of walking o Extensors of the knee (in the anterior compartment) Quadriceps: Largest muscle group in the body Consists of four individual muscles: o Rectus femoris, vastus medialis, vastus lateralis, vastus intermedius o Converge to form the quadriceps tendon, which envelops the patella and continues as the patellar ligament (inserting on the tibial tuberosity) Rectus femoris: o Originates on the AIIS and inserts on tibial tuberosity o Flexes the thigh and extends the leg (soccer kick) o Works w/iliopsoas during walking Vastus medialis/lateralis/intermedius o All originate on the femoral shaft and insert on the tibial tuberosity o Vastus intermedius is DEEP to rectus femoris Are powerful knee extensors o Most important function: to accept weight during the loading response (flat foot) of the stance phase o When these muscles are not used, atrophy is significant Medial compartment of the thigh o Consists primarily of adductor muscles Exception: obturator externus Originate on the anteroinferior surface of the bony pelvis and insert on the linea aspera of the femur o Main innervation is via the obturator nerve o These muscles also assist in flexion and extension of the thigh AGAINST RESISTANCE Ex.) running, weight-training o Obturator externus: Originates on the medial aspect of the obturator foramen (the foramen formed by the three pelvic bones) and inserts on the trochanteric fossa of the femur Stabilizes the femoral head in the acetabulum Also provides some flexion of and laterally rotates the femur o Adductor longus and brevis Flexion of the thigh NOTE: when the insertion of either rises above the origin, it’s function transitions from flexion to extension of the thigh o Adductor magnus The largest, strongest and most posterior of the medial compartment thigh muscles Has two components: Adductor portion: flexes the thigh Hamstrings portion: extends the thigh o Gracilis Adducts and medially rotates the femur o When you walk, your pelvis undergoes rotation (one side externally rotates while the other internally rotates), minimizing a drop in your center of gravity o Extensive or forcible adduction of the femur is typically not required Femoral triangle o Is one of three key areas of transition in the lower limb (along w/popliteal fossa and the tarsal tunnel) Transition areas are important b/c they conduct key structures between adjacent regions o Borders: Superior: inguinal ligament Lateral border: sartorius muscle Medial border: adductor longus muscle Floor: iliopsoas muscle (laterally) and pectineus (medially) Roof: fascia lata (deep fascia of the thigh) o Inguinal ligament Forms the superior border of the femoral triangle Goes from the ASIS to the pubic tubercle Is the inferior border of the external oblique muscle It serves in part to retain soft tissue structures Such structures are said to pass through the retroinguinal space o Retro-inguinal space Located deep to the inguinal ligament Inguinal ligament branches to form the iliopectineal arch and a continuation of the inguinal ligament Serves to divide the retro-inguinal space into a muscular compartment and a vascular compartment Muscular compartment: allows passage of iliopsoas muscle and femoral nerve Vascular compartment: allows passage of major vessels that run between the abdominopelvic cavity and the lower limb These vessels are surrounded by the femoral sheath o Femoral sheath A funnel-shaped fascial tube that surrounds vessels contained in the vascular compartment of the retro-inguinal space It allows said vessels to glide along the inguinal ligament during hip movements Divided into 3 compartments Lateral: femoral artery Intermediate: femoral vein Medial: lymphatic vessels NAVeL: contents of the femoral triangle (lateral to medial) Femoral nerve, femoral artery, femoral vein, lymphatics o Femoral canal = medial compartment of the femoral sheath Contains lymphatic vessels However these vessels do not fill the entire compartment, thus leaving empty space Femoral ring is an opening into the femoral canal Represents a potential site of herniation However normally the femoral ring is covered by the femoral septum Femoral septum derived from peritoneum and extraperitoneal fascia Hernias o The protrusion of a structure through the tissues that normally contain it o Abdominal hernias are common Typically involve loops of the small intestine protruding through areas of the abdominal wall that are muscularly deficient o Femoral hernias Usually originate at the femoral ring and appear as a tender mass in the femoral triangle The structure that is protruding (for example the small intestine) can become compromised due to the tough, inflexible lacunar ligament If the small intestines that are involved in the hernia have their blood flow reduced/constricted by the lacunar ligament, it can result in avascular necrosis Typically are more common in females due to the larger size of their pelvis Femoral artery o Aorta to common iliac artery to external iliac artery to femoral artery Note: the external iliac artery becomes the femoral artery when it passes inferior to the inguinal ligament o Bisects the femoral triangle and is RELATIVELY superficial Therefore its pulse can be taken by placing the palm of the hand inferior to the inguinal ligament However, because it is superficial it can be easily lacerated (cut) o Femoral artery gives off one major branch: The profunda femoris (deep artery of the thigh) This passes deep between the pectineus and adductor longus muscles in the femoral triangle It in turn gives off two branches: The lateral and medial circumflex femoral arteries o Note that it is possible for these to arise from the femoral artery itself rather than the profunda femoris (varies among individuals) o Note: the obturator artery (derived from the INTERNAL iliac artery) will also provide blood supply, specifically to the medial compartment of the thigh Veins o Venous drainage in the lower limb consists of superficial and deep veins o Femoral vein: major DEEP vein of the lower limb Femoral vein becomes the external iliac vein upon passing SUPERIOR (remember veins run up towards the heart) to the inguinal ligament o Great and small saphenous veins: major SUPERFICIAL veins of the lower limb The great saphenous vein runs up the lower limb and merges with the femoral vein at the saphenous opening Nerves o Femoral Nerve Derived from L2-L4 of the lumbar plexus Innervates the anterior compartment muscles of the thigh Gives off multiple cutaneous and muscular branches Anterior cutaneous branches of the femoral nerve: Provides SENSORY information to the SKIN of the anteromedial thigh Lateral cutaneous branches of the femoral nerve: Provides SENSORY information to the SKIN of the anterolateral thigh o Obturator nerve Derived from L2-L4 of the lumbar plexus Innervates the medial compartment muscles of the thigh Divides into anterior and posterior branches at the adductor brevis Cutaneous branches of the obturator nerve Provides a small patch of SENSORY innervation to the SKIN of the medial thigh Adductor canal o A long, narrow intermuscular passageway in the middle third of the thigh o Extends from the apex (point) of the femoral triangle to the adductor hiatus Adductor hiatus is situated near the inferior aspect of adductor magnus o Contains the femoral artery, femoral vein and the saphenous nerve Saphenous nerve innervates the medial aspect of the tibia o Composed of tough vastoadductor fascia Knee and Lower Leg Anatomical leg: the portion of the lower limb located between the knee and the ankle o Remember that the thigh is between the hip and the knee Bones of the leg o Tibia: dominant, weight-bearing bone of the leg o Fibula: subordinate (almost vestigial in nature), functions in muscle attachment and closure of the ankle joint Gives rise to the lateral malleolus While the forearm of the upper limb was focused on mobility, the leg of the lower limb is concerned with weight bearing Tibiofibular joint: 3 components o Proximal tibiofibular joint o Interosseous membrane (between the bones) o Distal tibiofibular joint 3 muscular compartments of the leg o Anterior, posterior, lateral Separated by bones (tibia, fibula), interosseous membrane, fascial septa o Generally speaking, the muscles of each compartment have a similar function and innervation Anterior leg o Anterior compartment muscles are located lateral to the anterior border of the tibia o Muscles of the anterior compartment of the leg: Tibialis anterior Extensor digitorum longus Fibularis tertius Is actually an extra belly of the extensor digitorum longus Extensor hallucis longus Hallucis implies the big toe These muscles cross the ankle joint (talocrural joint) Allow for dorsiflexion of the ankle and extension of the toes (bring toes up to your chin) Dorsiflexion ROM: ~20 degrees o Note that strength and ROM of dorsiflexion is LESS than strength of plantarflexion Roles of dorsiflexion: o Provides balance while standing o Active during walking Keep foot flat to ground Permit smooth, eccentric lowering of foot Pull body forward over fixed foot o Tibialis Anterior Most medial, superficial muscle of the anterior compartment Origin: superior half of the lateral tibia and adjoining surfaces of the interosseous membrane Insertion: medial cuneiform and the base of the 1st metatarsal Actions: provides leverage for dorsiflexion and inversion, supports medial longitudinal arch o Compartment syndrome Fascial compartments are closed spaces ending at the joints Fascia in the leg (especially proximally) is strong and resistant to expansion Compartment syndrome is increased pressure within a limited anatomical space Example of a limited anatomical space is a fascial compartment Example: fluid builds up in the leg, due to either infection or injury; this accumulating fluid causes increased pressure in the fascial compartment and hence the structures within said compartment, i.e. blood vessels If these blood vessels become constricted, it can diminish perfusion of tissues distal to the point of compression, causing ischemia, hypoxia and possible necrosis Treatment usually involves a fasciotomy, in which the fascia overlying a compartment is incised, allowing the inherent structure more freedom Shin splints are a mild form of compartment syndrome in the anterior compartment of the leg Due to repetitive microtrauma of tibialis anterior Can occur with sudden overuse or intense training Treatment: rest, ice, strengthening o Extensor digitorum longus The most lateral of the anterior compartment leg muscles Consists of four tendons (on digits 2-5) Origin: superior and medial border of the fibula and the adjacent surfaces of the interosseous membrane Insertion Each tendon of extensor digitorum longus and extensor digitorum brevis (located deep to EDL) form an extensor expansion This extensor expansion divides into o o o o o Central band located at the base of the middle phalanx o 2 lateral bands located at the base of the distal phalanx Primary extensor of digits 2-5; also dorsiflexes the ankle Extensor hallucis longus Located deep and in-between tibialis anterior and extensor digitorum longus Extends digit #1 (big toe) and dorsiflexes the ankle Is the ONLY extensor of the hallux (big toe) and is critical in making sure this toe is “cleared” from the ground during walking Origin: medial anterior surface of the fibula Insertion: distal phalanx of the hallux (digit #1) Fibularis tertius Is actually another belly of extensor digitorum longus Goes to the 5th metatarsal Weak dorsiflexion; eversion; possible protection of the anterior tibiofibular ligament Retinacula Superior extensor retinaculum and inferior extensor retinaculum Two band-like thickenings of the deep (crural) fascia at the inferior end of the anterior compartment of the leg Serves to bind the tendons of the anterior compartment muscles and prevent anterior bowstringing during dorsiflexion Bowstringing during dorsiflexion would mean that the tendons become taught in a straight line during the action of dorsiflexion Nerve supply Anterior compartment muscles of the leg are innervated via the deep fibular nerve Located deep and in-between tibialis anterior, extensor digitorum longus and extensor hallucis longus o Blood supply Anterior compartment muscles derive their blood supply from anterior tibial artery Femoral artery becomes the popliteal artery which branches at the inferior border of the poplietus o The small terminal branch is the anterior tibial artery Lateral leg o The lateral compartment of the leg is the smallest of the three o Bordered by the anterior and posterior intermuscular septa o Muscles of the lateral compartment of the leg are responsible for eversion and weak plantarflexion Eversion: bringing the lateral malleolus up Plantarflexion: pointing the toes to the ground o 2 muscles Fibularis longus and brevis Longus is superficial and longer than brevis o Insertion Fibularis longus inserts on the base of the 1st metatarsal and the medial cuneiform Is the primary evertor of the foot Fibularis brevis inserts on the base of the 5th metatarsal o The tendons of fibularis longus and brevis pass through the superior fibular retinaculum and the inferior fibular retinaculum o Importance of eversion Keeps the medial margin of your foot on the ground during the toe-off stage of walking Prevents excessive inversion of the foot (that would otherwise lead to ankle sprain) o Because of the placement of fibularis longus in the human leg, it allows us greater eversion Ultimately allows us to walk on the medial (inner) part of our foot, as opposed to other primates o Innervation is via the superficial fibular nerve o Blood supply The lateral compartment leg muscles do NOT have an artery directly supplying them They INDIRECTLY receive blood via perforating arteries derived from the fibular and anterior tibial arteries Common fibular nerve o Because of its superficial location in the leg, it can become easily damaged o It can actually be severed with fibular neck fractures or knee injuries o Common fibular nerve divides into the superficial and deep fibular nerves Superficial fibular nerve innervates the lateral compartment of the leg, which allows for eversion of the foot Deep fibular nerve innervates the anterior compartment of the leg, which allows for dorsiflexion of the foot o Clinical scenario: if you sever the common fibular nerve, you essentially “kill” the nerves distally derived from it, i.e. the superficial and deep fibular nerves w/o this innervation, the anterior and lateral compartment leg muscles will be paralyzed and atrophy, and be accompanied by inability to dorsiflex or evert the foot ultimately results in footdrop w/unopposed inversion; the toes now drag the floor during the swing phase of walking the patient resultantly develops a compensatory gait in which the leg is brought up, swung out and “clops” to the ground “clopping” due to the inability to smoothly lower the foot (b/c of loss of dorsiflexion) Posterior leg o The posterior compartment (the largest) leg muscles are located posterior to the tibia, fibula and interosseous membrane o Posterior compartment leg muscles are responsible for plantarflexion of the foot and toes and inversion o Propulsion during locomotion (walking) is performed mainly by way of the plantarflexors of the leg Greatest amount of energy expenditure during locomotion is in the concentric contraction of these muscles o Posterior compartment leg muscles are divided by the transverse intermuscular septum into Superficial posterior compartment muscles Deep posterior compartment muscles o Superficial posterior compartment leg muscles Form the prominence of the calf 3 muscles Gastrocnemius, soleus, plantaris o Gastrocnemius and soleus form the triceps surae o Gastrocnemius has a medial and lateral head o Soleus and plantaris are deep to the gastrocnemius o Plantaris is superior to soleus o Plantaris is absent in a small percentage of the population o All three muscles come together inferiorly to form the calcaneal tendon o Gastrocnemius Consists of a medial and lateral head Originates on the distal end of the femur and inserts as the calcaneal tendon b/c it crosses the knee and the ankle, it has action at both joints allows for flexion of the knee and plantarflexion of the ankle o note: it cannot exert full power on both @ the same time o checks and balances: if the knee is fully extended, gastrocnemius is not at work on the knee, therefore all of its power can be diverted to plantarflexion of the ankle o however, as the knee approaches full flexion, you are engaging (at least in part) your gastrocnemius, and thus less power is able to be diverted to plantarflexion (b/c the muscle has become too slack) o Soleus Located deep to gastrocnemius Considered the “workhorse” of plantarflexion Can perform plantarflexion of the foot regardless of knee angle Consists mainly of slow-twitch (red, aerobic, myoglobin-rich) fibers Allows for strong, sustained plantarflexion Originates as an inverted “U” on the tibia and fibula Inserts on the calcaneus as the calcaneal tendon o Deep posterior compartment leg muscles 4 muscles Flexor hallucis longus Flexor digitorum longus Tibialis posterior o These first 3 are your plantarflexors Popliteus These muscles are weak contributors to plantar flexion Due to the close proximity of the tendons to the ankle joint They are not able to raise the body in plantarflexion by themselves (require the superficial posterior leg muscles for help) o Absence of plantarflexion If plantarflexion is absent, you have a diminished “push-off” phase during walking Compensatory gait: lower limb is externally rotated and the transversely positioned foot is “rolled-over” during the stance phase Involves extension of the hip via gluteus maximus and hamstrings and extension of the knee via quadriceps o Flexor hallucis longus and flexor digitorum longus Flexor hallucis longus Origin: middle posterior aspect of the fibula Inserts: distal phalanx of digit #1 (big toe) Important to our sense of foot position and leverage Flexor digitorum longus Origin: middle posterior aspect of the tibia Inserts: distal phalanges of digits #2-5 Are crucial in the “toe-off” action near the end of walking and keeping the pads of the toes in contact w/the ground o Tibialis posterior The deepest posterior leg muscle Is located between flexor hallucis longus and flexor digitorum longus Originates on the superior aspect of the tibia, fibula and interosseous membrane Insertion: navicular, cuboid, calcaneous, medial and intermediate cuneiforms, 2nd to 4th metatarsals Supports the medial longitudinal arch of the foot; main invertor muscle of the leg o ALL muscles of the posterior compartment of the leg (superficial and deep) are innervated by the tibial nerve o Blood supply to the posterior compartment leg muscles is via the posterior tibial artery Popliteal artery passes the inferior border of popliteus and splits to form the anterior and posterior tibial arteries Anterior tibial artery supplies the anterior compartment leg muscles Posterior tibial artery supplies the posterior compartment leg muscles The posterior tibial artery branches to form the fibular artery, which runs deep to flexor hallucis longus o Leg cutaneous innervation Derived from the femoral and sciatic nerves Femoral nerve gives rise to the saphenous nerve which provides cutaneous innervation to the anteromedial side of the leg Sciatic nerve gives rise to the tibial and common fibular nerves which both contribute to the lateral and medial sural nerves that provides cutaneous innervation to the posterolateral side of the leg Remember: cutaneous innervation means SENSORY innervation to the SKIN Gluteal Region Pelvis: comprised of multiple bones o Os coxae: 2 each of the ilium, ischium, pubis o Sacrum: consists of 5 fused vertebrae o Coccyx: consists of roughly 3 fused vertebrae o Contains many sites for muscle attachment Offers support in regards to locomotion and posture Keeps you steady and upright Structures of the pelvis are bound to one another by way of ligaments o Anterior and posterior sacroiliac ligaments Attach the upper sacrum to the ilium o Sacrotuberous ligament extends from the sacrum to the ischial tuberosity o Sacrospinous ligament extends from the sacrum to the ischial spine o Ischial spine separates the greater and lesser sciatic notches o Note: the sacrotuberous ligament, the sacrospinous ligament and the ischial spine form the greater and lesser sciatic foramina Greater sciatic foramen o Serves as a passageway into the pelvis o Contains: Piriformis muscle, sciatic nerve, superior and inferior gluteal nerves and arteries, obturator internus nerve, quadratus femoris nerve, pudendal nerve and artery Lesser sciatic foramen o Serves as a passageway into the perineum o Contains: Obturator internus muscle, nerve to obturator internus, pudendal nerve and artery Note: the pudendal artery and nerve come out via the greater sciatic foramen, make a loop around the sacrospinous ligament and enters via the lesser sciatic foramen Gluteus maximus: o Innervation: inferior gluteal nerve o Actions: extends the thigh, lateral rotation, steadies thigh, assists in rising from a seated position Gluteus medius: o Innervation: superior gluteal nerve o Actions: abduct and medially rotate the thigh, keeps pelvis level when ipsilateral limb is weight-bearing, advances leg during swing phase of walking Gluteus minimus: o Innervation: superior gluteal nerve o Actions: abducts and medially rotates the thigh, keep pelvis level when ipsilateral limb is weight-bearing, advances leg during swing phase of walking Tensor of fascia lata o Innervation: superior gluteal nerve o Action: abduct and medially rotate the thigh, keep pelvis level when ipsilateral limb is weight-bearing, advances leg during swing phase of walking Piriformis o Innervation: branches of VENTRAL RAMI of S1, S2 o Actions: laterally rotate and extend thigh, abduct a flexed thigh, steadies femoral head in the acetabulum Obturator internus o Innervation: nerve to obturator internus o Actions: laterally rotate and extend the thigh, abduct a flexed thigh, steadies the femoral head in the acetabulum Superior and inferior gemelli o Innervation: Superior: nerve to obturator internus Inferior: nerve to quadratus femoris o Action: laterally rotate and extend the thigh, abduct a flexed thigh, steadies the femoral head in the acetabulum Quadratus femoris o Innervation: nerve to quadratus femoris o Actions: laterally rotate thigh, steadies the femoral head in the acetabulum Note: there are 6 muscles that serve to laterally rotate the thigh and stabilize the hip joint o Piriformis, obturator internus, superior and inferior gemelli, quadratus femoris, obturator externus Gluteal Region Muscles: Superficial and Deep Layer o Superficial: big gross actions, origin is on external surface/margins of the ala of the ilium Gluteus Maximus Innervation: inferior gluteal nerve Blood supply: superior and inferior gluteal arteries Actions: extension and weak lateral rotation of the thigh o Strongest hip extensor; also used when rising from a seated position, straightening from a bending position, walking uphill/upstairs, running Injury: results in gluteus maximus lurch o Patient extends trunk (leans back) during heel strike on affected side o Done to compensate for weakness in hip extension Gluteus Medius and Minimus Medius is deep to Gluteus Maximus; Minimus is deep to Gluteus Medius Innervation: superior gluteal nerve Blood supply: superior gluteal artery Actions: abduct/stabilize the thigh and medially rotate the thigh; also helps keep pelvis level during gait Tensor Fasciae latae Merges with the IT band which in turn inserts on the anterolateral tubercle of the tibia Innervation: superior gluteal nerve Blood supply: superior gluteal artery Actions: flexor of the thigh; abducts and medially rotates the thigh o Is a synergist muscle (it works in concert w/other muscles to perform these functions) o Works alongside iliopsoas and rectus femoris to perform flexion of the thigh o Works alongside gluteus medius/minimus to perform abduction/medial rotation of the thigh o Deep: smaller more precise actions; they laterally rotate the thigh (duck walk) and stabilize the hip joint (by working alongside the strong hip ligaments to steady the femoral head in the acetabulum) Piriformis Largest of the deep gluteal muscles Innervation: ventral rami of S1 and S2 (nerve to piriformis) Blood supply: variable Actions: laterally rotates, abducts the thigh; stabilizes hip joint Serves as the landmark for the gluteal region b/c the blood vessels/nerves in this area are named in reference to their location to piriformis Sciatic nerve: consists of tibial nerve and common fibular nerve o Normally runs inferior to piriformis o However, it is possible for the common fibular portion of the sciatic nerve to run through or pass over piriformis Piriformis syndrome: o Peripheral neuritis (inflammation/irritation) of the sciatic nerve o Often due to sitting on a wallet o Treatment includes: stretching, NSAIDs, analgesics, OMT (counterstrain), etc. Triceps Coxae: Obturator internus, superior/inferior gemelli Obturator internus is “sandwiched” between the gemelli Innervation: o Obturator internus: nerve to obturator internus o Superior gemellus: nerve to obturator internus o Inferior gemellus: nerve to quadratus femoris Actions: lateral rotation and abduction of the thigh; stabilizes the hip Quadratus femoris: Located inferior to the triceps coxae Is rectangular in shape Innervation: nerve to quadratus femoris Actions: strong lateral rotation of the thigh; stabilizes the hip Roadmap (to get your bearings) Superior to inferior orientation of deep gluteal muscles o Piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris o Obturator externus Is technically a muscle of the medial compartment of the thigh Innervation: obturator nerve Action: lateral rotation of the thigh; stabilizes the hip Gluteal bursae o Synovial fluid sacs that function to reduce friction and permit free movement o Trochanteric bursa: largest; separates the superior fibers of gluteus maximus from the greater trochanter of the femur o Ischial bursa: often absent; separates the inferior part of the gluteus maximus from the ischial tuberosity o Gluteofemoral bursa: separates the IT band from the superior part of the proximal attachment of vastus lateralis Clunial nerves: o Cutaneous nerves that supply the skin of the gluteal region Remember: cutaneous = sensory, skin o Are susceptible to injury during procedures of removing iliac bone for grafting purposes o Superior clunial nerves: Supply skin of superior buttock as far as the tubercle of the iliac crest o Middle clunial nerves: Supply skin over the sacrum and adjacent areas of the buttock o Inferior clunial nerves: Supply skin of inferior half of the buttock as far as the greater trochanter of the femur Femoral nerve o Derived from L2-L4 (lumbar plexus) o Innervates the anterior compartment of the thigh (flexors of the thigh and extensors of the knee) Obturator nerve o Derived from L2-L4 (lumbar plexus) o Passes through obturator foramen to innervate the medial compartment of the thigh (adductors of the thigh) Sciatic nerve o Largest nerve in the body o Derived from L4-S3 o Consists of the tibial nerve and common fibular nerve Tibial nerve: supplies posterior compartment of the thigh (extension of the thigh and flexion of the knee) and posterior compartment of the leg (plantarflexion of foot and flexion of the toes) Common fibular nerve: wraps around the fibular head to branch into a deep fibular nerve (innervates the anterior compartment of the leg (dorsiflexion of the foot and extension of the toes)) and a superficial fibular nerve (innervates lateral compartment of the leg (eversion of the foot)) o Also gives off articular branches that supply the hip and motor branches that supply the foot Gluteal IM injections o Provides a large surface area for absorption of IM medications o Avoid neurovascular damage by injecting in the superolateral quadrant How to find: Open hand and place middle finger on the tubercle of the iliac crest Place forefinger on the ASIS The area in between is considered safe for injection Pudendal nerve o Main nerve of the perineum and chief nerve of the external genitalia o Derived from S2-S4 o Innervation: Sensory innervation to the genitalia Muscular branches to perineal muscles, external urethral sphincter, external anal sphincter Superior gluteal nerve o Derived from L4-S1 o Innervates gluteus medius and gluteus minimus o Trendelenburg Test: Have your patient stand on one leg Normal: the gluteus medius and minimus muscles on the contralateral side should contract, keeping the pelvis level With injury to the superior gluteal nerve, when the patient stands on one leg, the pelvis will “fall” towards the unsupported side Reason: the superior gluteal nerve is injured, which means that gluteus medius/minimus are non-functional (or weak) and can’t contract, resulting in a positive Trendelenburg test Inferior gluteal nerve o Derived from L5-S2 o Innervates gluteus maximus Posterior cutaneous nerve of the thigh o Supplies more skin than any other cutaneous nerve o Derived from S1-S3 Perineal branch (S2-S3) supplies skin of perineum Inferior clunial nerves (S1-S2) supplies skin of inferior buttock Other fibers supply skin of posterior thigh and proximal leg Arteries of the gluteal region o Roadmap: abdominal aorta becomes common iliac artery which splits into external and internal iliac arteries The internal iliac artery gives rise to: Superior gluteal artery, inferior gluteal artery, internal pudendal artery o Superior gluteal artery Largest branch of the internal iliac artery Branches into: Superficial division: supplies gluteus maximus and the skin overlying its origin Deep division: supplies gluteus medius/minimus, tensor fascia latae Forms anastomoses with the inferior gluteal and medial circumflex femoral arteries o Inferior gluteal artery Supplies gluteus maximus, obturator internus, quadratus femoris and the superior portion of the hamstrings (biceps femoris, semitendinosus, semimembranosus) o Internal pudendal artery Supplies the skin, external genitalia and muscles in the perineal region Veins of the gluteal and posterior thigh regions o Roadmap: remember veins take blood UP towards the heart Femoral vein becomes the external iliac vein External iliac vein joins with the internal iliac vein to become the common iliac vein The common iliac veins on either side join to become the inferior vena cava o Gluteal veins (superior and inferior): drain blood form the gluteal region and are considered tributaries of the internal iliac veins o Internal pudendal veins: drain blood from the external genitalia or pudendum and joins up with the internal iliac vein Lymphatic drainage of the gluteal and thigh regions o Deep tissues: lymph travels to the superior and inferior gluteal lymph nodes and then to the internal/external/common iliac lymph nodes and then to the lateral lumbar (aortic) lymph nodes o Superficial tissues: lymph travels to the superficial inguinal lymph nodes and then to the external iliac lymph nodes Posterior Thigh and Popliteal Fossa Thigh has 3 compartments: anterior, posterior, medial o Anterior and posterior compartment separated via lateral intermuscular septum o Anterior and medial compartments separated via medial intermuscular septum o NO TRUE FASCIAL SEPARATION BETWEEN POSTERIOR AND MEDIAL COMPARTMENTS Posterior compartment of thigh: o Actions: extension of the thigh, flexion of the knee o Occupied principally by the hamstrings Lateral to the hamstrings is vastus lateralis Medial to the hamstrings is adductor magnus Hamstring Muscles (lateral to medial) o Biceps Femoris 2 heads: long and short o Semitendinosus Look for the long tendon that attaches to the medial aspect of the tibia o Semimembranosus Deep to semitendinosus The hamstrings all originate on the ischial tuberosity EXCEPT for the short head of biceps femoris (originates on the linea aspera of the femur) Pes anserinus: the location on the medial aspect of the tibia where the tendons of sartorius, gracillus, and semitendinosus all insert Actions of the hamstrings o Designed to extend the thigh and flex the knee o However, they are not able to do both maximally at the same time (just like gastrocnemius) When the knee is flexed, the hamstrings have been shortened such that full thigh extension is not possible When the thigh is extended, the hamstrings have been shortened such that full knee flexion is not possible o If the lower limbs are fixed, hamstring contraction will help to extend the trunk (bend backward) o When the knees are flexed… Semitendinosus and semimembranosus allow medial rotation of the knee while biceps femoris allows lateral rotation of the knee Note: this rotation about the knee is SUBTLE Think skiing motion Hamstrings and gait o Hamstring contraction allows you to remain upright while standing Prevents falling forward o During walking: Hamstring contraction during swing phase allows for the slight knee flexion required to bring your leg up off the ground Also allows for deceleration of thigh flexion and knee extension during the terminal swing phase Hamstrings injury o Hamstrings strains are more common than quadriceps strains o Often occurs in sports with rapid/violent muscle exertion (sprinting) o Most often occur when the hamstrings muscle is in a lengthened position During limb deceleration in the terminal swing phase of walking i.e. when the thigh is flexed and the knee is extended o Reasoning: thigh flexion and knee extension is facilitated by the QUADRICEPS (these muscles contract and therefore are shortened), which means the antagonistic muscle group, the HAMSTRINGS are lengthened o If significant, it may also result in an avulsion fracture at the ischial tuberosity Nerves o All hamstring muscles are innervated by the tibial portion of the sciatic nerve EXCEPTION: the short head of biceps femoris is innervated by the common fibular division of the sciatic nerve o Cutaneous innervation to the posterior thigh is mainly via the posterior femoral cutaneous nerve This nerve is actually located deep to the fascia lata, with only terminal branches extending to the surface However, the lateral femoral cutaneous nerve innervates the skin on the lateral aspect of the posterior thigh Blood supply o The posterior compartment of the thigh has no major artery DIRECTLY supplying it o Instead it receives its blood supply via: Inferior gluteal artery (derived from internal iliac artery) Medial circumflex femoral artery and perforating branches (both derived from the profunda femoris) Profunda femoris = deep artery of the thigh, a branch off the femoral artery Note that the perforating branches run transversely inbetween compartments Most lymphatic drainage of the thigh comes by way of superficial inguinal lymph nodes (which follow the femoral vein) Popliteal fossa o A fat-filled, diamond-shaped intermuscular space on the posterior aspect of the knee o Represents a key transition point between the thigh and the leg o Is where the sciatic nerve branches into the tibial and common fibular nerves, also where the femoral artery becomes the popliteal artery o Is covered by popliteal fascia which serves to protect the contents within o Boundaries: Medial: Upper: semitendinosus and semimembranosus Lower: medial head of gastrocnemius Lateral: Upper: biceps femoris Lower: lateral head of gastrocnemius, plantaris Roof: skin and popliteal fascia Floor: femur, knee join capsule, popliteus muscle o Contents In the popliteal fossa, the sciatic nerve splits into the tibial nerve and the common fibular nerve Note that the common fibular nerve will later split into the deep and superficial fibular nerves Cutaneous nerves: The tibial nerve gives rise to the medial sural cutaneous nerve The common fibular nerve gives rise to the lateral sural cutaneous nerve o The lateral sural cutaneous nerve in turn gives off a branch known as the sural communicating branch o The sural communicating branch joins the lateral and medial sural cutaneous nerves to form the sural nerve The sural nerve provides sensory innervation to the skin of the lateral half of the posterior leg The saphenous nerve provides sensory innervation to the skin of the medial half of the posterior leg The small saphenous vein pierces the popliteal fossa to empty into the popliteal vein Note: the posterior tibial vein becomes the popliteal vein at the inferior border of popliteus The popliteal vein in turn becomes the femoral vein at the adductor hiatus (near the tendinous insertion of adductor magnus) The femoral artery becomes the popliteal artery at the adductor hiatus At the inferior border of popliteus, the popliteal artery splits to become the anterior and posterior tibial arteries Note that the popliteal artery is the deepest structure in the popliteal fossa The popliteal artery gives off multiple muscular and genicular branches The genicular branches supply the capsule and ligaments of the knee joint o Five total: Superior/inferior medial genicular arteries Superior/inferior lateral genicular arteries Middle genicular artery These branches form anastomoses that provide extensive circulation to the knee o Is important b/c when the knee is flexed, the popliteal artery is clamped down, but blood is still able to flow to the knee via the other branches Lymph from popliteal lymph nodes eventually reaches the deep inguinal lymph nodes The popliteal fascia superficial to the fossa is strong and resistant to expansion In the popliteal fossa, since the popliteal artery and vein are in close proximity to one another, it is possible for a fistula to form, compromising blood supply to structures distal to this point (i.e. the leg and foot) Ankle and Foot Ankle (talocrural joint) o Made up of the medial malleolus (from the tibia), the lateral malleolus (from the fibula) and the talus (keystone of the ankle) Foot: the portion of the lower limb distal to the ankle o Includes: tarsal bones, metatarsal bones, phalanges o Designed to support body weight (bipedal stance) and provide leverage for locomotion o Has both a dorsal and plantar surface o Can be classified anatomically or functionally Anatomical classification Tarsus (tarsal bones), metatarsus (metatarsal bones), phalanges Functional classification Hindfoot: talus and calcaneus Midfoot: navicular, cuboid, cuneiforms, metatarsals Forefoot: phalanges o Parts of the foot vary in thickness and texture of the skin, subcutaneous tissue and deep fascia Dependent upon the extent of weight-bearing, distribution, grip and abrasion o Dorsum of foot: superior Features thinner, less sensitive skin alongside loose subcutaneous tissue As a result, swelling of the foot is more prominent on this side o Sole of the foot: plantar surface Features thicker, highly vascularized and sensitive skin alongside strong fibrous connective tissue Makes sense since this is what is in contact with the environment Also contains pressure chambers (fat-filled pockets lined with ligaments) designed to evenly distribute pressure/forces across the foot during standing and walking If these weren’t present, forces and pressures would accumulate more in certain areas than others, resulting in pressure necrosis o The deep fascia of the foot is thicker on the sole rather than the dorsum of the foot The deep fascia on the sole is known as plantar fascia The thickest part of the plantar fascia (located in the middle of the sole of the foot) is known as the plantar aponeurosis Role of the plantar aponeurosis: protects underlying structures, maintains the arch of the foot, offers attachment for skin/subcutaneous tissue, helps create muscular compartments in the foot Plantar fasciitis: inflammation of the plantar fascia Often caused by overuse Creates pain in the plantar and medial aspects of the foot; especially upon extension of big toe and dorsiflexion of foot Repeated tearing of the plantar aponeurosis can generate a bone spur at its proximal attachment to the calcaneal tuberosity o Functions of the foot: support body weight, provide leverage for locomotion The foot has the ability to deform on contact, allowing it to absorb many of the forces that otherwise would be transmitted farther up the skeleton Much of the flexibility of the foot is provided by the numerous bones and joints (alongside the associated muscles and ligaments) contained therein o Arches of the foot Medial/lateral longitudinal arches, transverse arch Formed by the arrangement of the tarsal and metatarsal bones Function to absorb shock and offer a springboard effect for locomotion In addition, they also offer sufficient strength o o o o The arches are supported via: the wedge-shape of the bones, associated ligaments and tendons Joints of the foot Intertarsal joints: between the tarsal bones Tarsometatarsal joints: between the tarsal and metatarsal bones Intermetatarsal joints: between the metatarsal bones Metatarsophalangeal joints: between the metatarsals and phalanges Interphalangeal joints: between the phalanges (think DIP and PIP) Movements at the FOOT joints Inversion/eversion of the foot Inversion: bringing medial malleolus up Eversion: bringing lateral malleolus up Flexion/extension of the toes Flexion: pointing toes down (like your gripping something) Extension: pointing toes up towards your chin NOTE: dorsiflexion and plantarflexion are permitted at the ANKLE (talocrural) joint! When the foot is weight-bearing, the arches of the foot allow transmission of force through the talus to: Calcaneus (heel) Heads of 1st to 5th metatarsals Note that the head of the 1st metatarsal (big toe) is in proximity to two sesamoid bones that are designed to protect the tendon of flexor hallucis longus Foot inversion/eversion These motions are facilitated by the intertarsal and tarsometatarsal joints Subtalar joint: functionally speaking consists of two parts Talocalcaneal joint: articulation between the talus and calcaneus Talocalcaneal portion of the talocalcaneonavicular joint (the articulation amongst the talus, calcaneus and navicular bones) Transverse tarsal joint: also consists of two parts Talonavicular portion of the talocalcaneonavicular joint Calcaneocuboid joint: articulation between the calcaneus and the cuboid The greatest amount of foot movement occurs at this joint o Here you have rotation of the midfoot and forefoot about the hindfoot Often a site of surgical amputation Tarsometatarsal joints Allows for some foot rotation and flexion/extension o This is important in allowing the foot to adapt to uneven surfaces o Flexion/extension of the toes Permitted via the metatarsophalangeal and interphalangeal joints Note: digits 2-5 have BOTH a PIP and DIP joint while digit 1 (big toe) has a single IP joint The metatarsophalangeal joints also allow for abduction/adduction of the toes Abduction: spreading toes apart Adduction: bringing toes together Three main ligaments on the plantar surface of the foot: Long plantar ligament Short plantar ligament (plantar calcaneocuboid) Spring ligament (plantar calcaneonavicular) o Supports the talus All three are involved in supporting the longitudinal arch of the foot o Flatfoot = Pes Planus Is normal before the age of three Different types Flexible flatfeet: feet are normal when not bearing weight o Due to loose or degenerated ligaments Rigid flatfeet: feet are flat in ALL conditions o Due to bone deformity Acquired flatfeet: fallen arches secondary to tibialis posterior dysfunction o Spring ligament is unsupported and fails With loss of the arch(es), the talus will be displaced inferiorly and medially o Muscles of the foot Intrinsic muscles of the foot originate and insert in the foot Grouped into two categories Dorsal extensors and plantar flexors Function: support the arches and assist the long muscles in locomotion o Plantar foot muscles Located under the boney arch between the heel and the toes Organized into 4 layers Layer one: o Deep to plantar aponeurosis but superficial to the neurovasculature o Abductor hallucis: abducts big toe o Flexor digitorum brevis o Abductor digiti minimi: abducts digit 5 Layer two: o Deep to flexor digitorum brevis and abductor hallucis o Quadratus plantae: inserts on the tendon of flexor digitorum longus o Lumbricals: originate on the tendon of flexor digitorum longus Flex proximal phalanges and extend the middle and distal phalanges of digits 2-5 Layer three: o Deep to quadratus plantae and tendon of flexor digitorum longus o Flexor hallucis brevis: contains a channel that allows passage of the tendon of flexor hallucis longus o Adductor hallucis: transverse and oblique head o Flexor digiti minimi brevis Layer four: o NOTE: axis of abduction/adduction of the toes is digit 2 o Plantar interossei (PAD): adduct digits 3-5 o Dorsal interossei (DAB): abduct digits 2-4 Remember digits 1 and 5 have their own separate abductor muscles (abductor hallucis and abductor digiti minimi) o Furthermore, these muscles also flex the metatarsophalangeal and extend the interphalangeal joints Plantar foot muscles are innervated via the medial and lateral plantar nerves (derived from the tibial nerve) Lateral plantar nerve innervates deep and lateral plantar muscles, including all the interossei Medial plantar nerve innervates superficial and medial plantar muscles Plantar foot muscles receive their blood supply from the medial and lateral plantar arteries (derived from the posterior tibial artery) Note: lateral plantar artery gives rise to plantar arch Roadmap: o Posterior tibial artery gives rise to the medial and lateral plantar arteries o Lateral plantar artery gives rise to the plantar arch o Plantar arch gives rise to the plantar metatarsal arteries o Plantar metatarsal arteries give rise to the plantar digital arteries o Dorsal foot muscles Extensor digitorum brevis Assists extensor digitorum longus Extensor hallucis brevis Assists extensor hallucis longus Innervated by the deep fibular nerve Note: the deep fibular nerve also innervates the anterior compartment leg muscles Blood supply: Dorsalis pedis supplies most of the forefoot o Is derived from the anterior tibial artery (which becomes dorsalis pedis at the malleoli) Dorsalis pedis in turn branches to form: o Arcuate and lateral tarsal arteries Both these form anastomoses with one another Dorsalis pedis is a common site in which to take a pulse o Diminished pulse may indicate peripheral artery disease o Cutaneous innervation of the foot Dorsum: deep and superficial fibular nerves and saphenous nerve Sole: medial and lateral plantar nerves o Deep fibular nerve entrapment Also known as “ski boot syndrome” Results in pain in the anterior compartment of the leg, radiating to the web-space between digits 1 and 2