Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
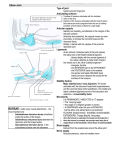
Normal and injured elbow: A pictorial review of MRI findings Poster No.: C-2227 Congress: ECR 2010 Type: Educational Exhibit Topic: Musculoskeletal Authors: C. H. Kim, M. H. Lee, E. C. Chung; Seoul/KR Keywords: elbow joint, MR imaging, anatomy and injury DOI: 10.1594/ecr2010/C-2227 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 29 Learning objectives To review the MR imaging of the elbow which includes the complex anatomy, normal variants of this joint with schematic illustrations, as well as commonly encountered traumatic and overuse injuries. Background The elbow joint has complex constituents which are three components of the humeroradial, humeroulnar and proximal radioulnar articulations with surrounding soft tissue structures. It is one of the commonly injured joints. Injuries of the elbow can occur from acute trauma or chronic overuse of the joint. MR imaging is the best diagnostic modality for evaluation of this complex joint, particularly of soft tissue constraints. Imaging findings OR Procedure details ANATOMY Osseous structures The elbow is composed of the ulnohumeral, radiocapitellar, and proximal radioulnar joints (Fig. 1). This allows the elbow two degrees of freedom: flexion-extension and pronationsupination. The most important bony stabilizer in extension is the articulation between the trochlea and the sigmoid notch of the olecranon. Osseous stability is enhanced in extension when the tip of the olecranon rotates into the olecranon fossa, and in flexion when the coronoid process locks into the coronoid fossa of the distal humerus and the radial head is contained in the radial fossa of the distal humerus. There are several commonly encountered ''pseudolesions'' on MR imaging of the elbow by normal anatomic variants. The olecranon and the coracoid process form the trochlear groove which is divided by a nonarticulated ridge. These groove and ridge may cause a misinterpretation on MR imaging of the elbow: pseudodefect of the trochlear groove, Page 2 of 29 transverse trochlear ridge, pseudodefect of the capitellum (Fig. 2 A-D). A prominent synovial fold also may simulate intraarticular disease (Fig. 2 E). Ligamentous structures - Medial (Ulnar) Collateral Ligament Complex The medial collateral ligament (MCL) complex consists of three parts: the anterior, posterior, and transverse or oblique bundles (Fig. 3). The anterior bundle (A-MCL) is the most discrete and strong structure accounting for the largest component of the medial collateral ligament complex and is best seen on coronal MR images. The posterior bundle of the MCL is more a thickening of the posterior capsule rather than a distinct ligament. The posterior bundle is a secondary stabilizer of the elbow joint against valgus and internal rotatory stress. The oblique (transverse) ligament runs between the coronoid and the tip of the olecranon. Because it is believed that the transverse ligament does not contribute significantly to joint, this one is not routinely evaluated on MR imaging. - Lateral (Radial) Collateral Ligament Complex The lateral collateral ligament (LCL) complex consists of four components, including the lateral ulnar collateral, annular, and radial collateral ligaments (Fig. 4). The lateral ulnar collateral ligament (LUCL) is one of the primary elbow constraints against varus and rotatory stress. The annular ligament encircles the radial head and stabilizes the proximal radioulnar joint. The radial collateral ligament (RCL) inserts into the annular ligament and stabilizes the radial head. Although the role of the RCL, LUCL, and annular ligaments in varus stability remains contentious, the more functionally important part is the proximal section, so demonstration of the humeral attachment is important in lateral ligament imaging. Muscular and Tendinous Structures The musculature of the elbow is divided into medial, lateral, anterior, and posterior compartments. The common flexor and extensor tendons are responsible for most musculotendinous pathology of the elbow and are best assessed on coronal MR images. The medial muscle group includes the pronator teres and the four superficial flexors: the flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and flexor digitorum superficialis. These muscles function to flex the wrist and pronate the forearm (Fig. 5 B, C-E). The lateral muscle group consists of three components: the superficial group, the common extensors, and the supinator muscle. The common extensor group is composed of the extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum and extensor digiti minimi. These muscles arise from the lateral epicondyle by way of the Page 3 of 29 common extensor tendon (Fig. 5 A, C-E). The extensor carpi radialis brevis is the most frequently involved tendon in common extensor pathology. The anterior compartment is comprised of the brachialis and biceps muscles, which flex the elbow (Fig. 6 A, C-E). The bicipitoradial bursa separates the distal biceps tendon from the anterior aspect of the radial tuberosity. The distal biceps tendon and the brachialis tendon is best evaluated on axial images or on the flexed abducted supinated (FABS) view. The posterior compartment is composed of the triceps, anconeus, and variably present anconeus epitrochlearis muscles (Fig. 6 B, C-E). The medial, lateral, and long heads of triceps blend to form a single musculotendinous unit that inserts into the tip of the olecranon and is separated from the olecranon by the deep olecranon bursa. The triceps tendon is best assessed on sagittal MR images. Nerves Around the Elbow At the elbow, the ulnar nerve runs within the cubital tunnel, where it lies in the posterior aspect of the medial epicondyle, then passes between the humeral and ulnar heads of flexor carpi ulnaris to enter the anterior compartment of the forearm. The radial nerve travels along the lateral aspect of the elbow joint, and divides into its motor branch, the posterior interosseous nerve (PIN), and its sensory branch, the superficial radial nerve at the level of the radiocapitellar joint. The PIN passes inferiorly within the radial tunnel between the two heads of supinator to the posterior forearm. The median nerve passes anterior to the elbow joint and lies medial to the biceps tendon and brachial artery. It enters the forearm between the two heads of pronator teres. OSTEOCHONDRAL INJURIES Osteochondritis Dissecans of the Capitellum Osteochondral abnormalities most commonly occur at the capitellum impacts on the radius, which are Osteochondrosis (Panner's disease) and osteochondritis dissecans. Osteochondrosis (Panner's disease) is characterized by irregularity and fragmentation of the capitellar epiphysis in adolescents, with subsequent remodeling with conservative management. Osteochondritis dissecans is a more focal abnormality, classically involves the anterior aspect of the capitellum, consisting of a separated osteochondral articular fragment that may separate from the native bone. Both are probably represent different stages of the same process, seen in different age groups. These entities usually occur in men between Page 4 of 29 the ages of 12 and 15 years when the capitellar epiphysis is almost completely ossified. Most patients have a history of repetitive overuse of the elbow, such as baseball players or gymnasts. Initially, excessive valgus stresses to the elbow cause a subchondral bony infarction with preservation of articular cartilage. Continued microtrauma cause bony necrosis and softening, resulting in separation of articular cartilage and secondary chondral injury. More progressive and severe conditions show osteoarthritis, intraarticular loose bodies, and locking. Sagittal MR images tend to show flattening of the anterior capitellum or irregularities of the radial head and T2-weighted or STIR images may show the extent of subchondral necrosis (Fig. 7). This pattern of injury should not be confused with the ''pseudodefect'' of the capitellum. LIGAMENTOUS INJURIES AND INSTABILITY Medial Collateral Ligament Injury and Medial Elbow Instability The MCL is the primary stabilizer against valgus stress and the most commonly injured ligament in the elbow. MCL tears may occur after acute valgus stress or dislocation. More commonly, however, MCL injury is due to repetitive valgus overload that results in microtrauma to the ligament by the act of throwing in baseball or tennis players. Continued overuse may lead to weakening and laxity of the ligament and eventually to complete ligamentous detachment or rupture. The anterior bundle and the humeral and ulnar insertions of the MCL are poorly visualized at arthroscopy, further emphasizing the important role of MR imaging in diagnosing ligament injury. Acute injury to the A-MCL most commonly involves the humeral insertion with an avulsion fracture of the medial epicondyle. An acute tear is seen as high-signal intensity and discontinuity of ligamentous fibers. In the case of complete rupture, total discontinuity of fibers with or without ligamentous retraction occurs (Fig. 8). A partial-thickness undersurface tear of the A-MCL with avulsion of the ulnar attachment of the deep fibers has been described as a T sign on MR or CT arthrography, because of tracking of fluid beneath the deep portion of the A-MCL. In chronic injury, diffuse increase in signal intensity and thickening of the ligament may occur from micro tears and remodeling. Concomitant flexor tendinopathy is common. Lateral Collateral Ligament Injury and Posterolateral Rotatory Instability LCL is the primary stabilizer of the elbow against varus stress. LCL injury is important in the development of posterolateral rotatory instability (PLRI) (Fig. 9). This condition usually follows an elbow dislocation in young patients, but in older patients the LUCL can be torn by a varus hyperextension stress without dislocation, such as after a fall upon Page 5 of 29 an outstretched hand with the forearm supinated, with a resultant axial and valgus load causing injury to the LUCL. TENDON INJURIES Lateral Epicondylitis Lateral epicondylitis is a tendinosis of the common extensor origin, associated with repetitive and excessive use of the wrist extensor muscles. Although commonly known as "tennis elbow" because of the high prevalence in tennis players, lateral epicondylitis also is commonly seen in golfers, carpenters, and in other workers whose job require repetitive rotatory motions of the forearm. The role of MRI is to exclude other causes of lateral elbow pain and to establish the therapeutic plan. On T2 weighted images, the common extensor tendon is thickened and showed high signal intensity at its insertion on the lateral epicondyle (Fig. 10). These changes involve the extensor carpi radialis brevis (ECRB) tendon in nearly all cases. Dystrophic calcifications may arise adjacent to the lateral epicondyle. Most patients who have moderate to severe lateral epicondylitis show partial- or fullthickness tears of the LUCL. Although osseous changes are rare, avulsion injury may occur. Medial Epicondylitis Medial epicondylitis is a tendinosis of the common flexor tendon origin. It is much less common than lateral epicondylitis. It is almost exclusively seen in athletes, such as golfers, tennis players, swimmers, pitchers, and javelin throwers who perform repetitive activities causing valgus and flexion forces to the elbow. MR imaging may diagnose the medial epicondylitis and assess for associated MCL injury. MRI shows thickening and increased signal intensity at the origin of the common flexor tendon (Fig. 11). The origins of the flexor carpi radialis and pronator teres are most commonly involved. Ulnar neuropathy is commonly associated. Biceps Tendinopathy and Biceps Tendon Injuries The distal biceps tendinopathy is usually caused by forced muscular flexion against strong resistance, such as weightlifting. The tendon shows increased signal intensity with or without tendon tear. Associated bicipitoradial bursa distension may compress the radial nerve. Rupture of the distal biceps tendon is rare and it is the result of a sudden extension force to the arm with the elbow in mid flexion. The findings of an empty distal tendon sheath filled with high-signal-intensity fluid, of tendon retraction are suggestive of complete tendon rupture (Fig. 12). Partial tears show hypersignal intensity within an abnormally thick or Page 6 of 29 thin biceps tendon, but no tendinous discontinuity. Secondary findings of tendon rupture including bone marrow edema of the radial tuberosity, soft tissue edema in the antecubital fossa and fluid in the bicipitoradial bursa may be present. Triceps Tendinopathy and Triceps Rupture Triceps tendinosis is an uncommon, but may be seen in sports that involve rapid or forceful extension of the triceps, such as javelin throwing, baseball, bench pressing, and gymnastics. Abnormal signal intensity presents at the insertion of the triceps tendon, with or without thickening of the tendon. Other chronic posterior elbow disorders, such as stress reaction of the olecranon process, olecranon osteophytes, loose bodies, and olecranon bursitis may be recognized. Triceps tendon rupture is a rare, but usually occurs at the insertion site. Partial ruptures are characterized by a small fluid-filled defect within the distal triceps tendon. Complete rupture shows a large fluid-filled gap between the distal triceps tendon and the olecranon process, with variable tendon retraction (Fig. 13). NEUROPATHIES Ulnar Nerve and Cubital Tunnel Syndrome The ulnar nerve may be injured by fibrous entrapment, compression, or subluxation of the nerve. Ulnar neuropathy can occur as an isolated problem or as the result of other medial elbow disorder including MCL injury, medial epicondylitis, and flexor-pronator strain. Cubital tunnel syndrome which is defined as compression of the ulnar nerve at the elbow is due to various casuses, such as cubitus valgus deformity, synovitis, osteophytes, hematoma results from MCL rupture, ganglia, loose bodies, muscle hypertrophy, or thickened retinaculum (Fig. 14). Radial Nerve and Radial Tunnel Syndrome Compression of the radial nerve has been referred to as radial tunnel syndrome (Fig. 15). Because this condition frequently has been misdiagnosed and unsuccessfully treated for lateral epicondylitis, it is also called as "resistant tennis elbow". It is mostly seen in activities requiring repetitive rotation of the forearm. Radial tunnel syndrome may be caused by radial head subluxation or a Monteggia fracture, synovitis, or thickening of the anterior capsule, and compression by the branches of the radial recurrent artery, or by space occupying lesions such as ganglia. Compression of the posterior interosseous nerve (PIN) a different clinical entity from radial tunnel syndrome in that muscle weakness accompanies the former (Fig. 16). The posterior interosseous nerve is compressed under a fibrous band known as the arcade Page 7 of 29 of Frohse at the proximal edge of the supinator muscle. It is referred to as deep radial nerve syndrome or supinator syndrome. Median Nerve and Pronator Syndrome Pronator syndrome is caused by entrapment of the median nerve at the elbow. It is usually associated with sports that involve repetitive pronation and supination of the forearm. Compression of the median nerve can occur at multiple sites by one of several different anatomic structures. Most commonly median nerve compressed by a fibrous band which runs between the superficial and deep heads of the pronator teres muscle. SYNOVIAL INFLAMMATION Bursa is a small fluid filled sac lined by synovial membrane. The bicipitoradial bursa is placed at the distal insertion of the biceps tendon in the cubital fossa. The bursa reduces friction between the biceps tendon and the tuberosity of the radius. When inflamed, bicipitoradial bursa shows distension and produces symptoms, such as mass in the cubital fossa, and neurologic symptoms by nerve compression. It is a rare condition, but mostly results from repetitive mechanical trauma (Fig. 17). The olecranon bursa is located superficial to the olecranon process between the ulna and the overlying skin. The olecranon bursa helps that the skin can slide over the olecranon process without friction. Because it is located superficially, the olecranon bursa is vulnerable to inflammation. It is presented as demarcated painful swelling over the olecranon process (Fig. 18). Images for this section: Page 8 of 29 Fig. 1: Schema of normal elbow joint The elbow joint consists of the ulnohemeral joint (arrow), the radiocapitellar (dashed arrow) joint and the proximal radioulnar joint (dashed circle). Page 9 of 29 Fig. 2: Normal variations of the elbow mimicking a disease. A. On T2-weighted sagittal MR image, pseudodefect of the trochlear groove (arrow) is seen as small, midline, cortical interruptions of the surface of the trochlear groove, simulating a cartilage defect. B. T2-weighted sagittal MR image shows transverse trochlear ridge (arrow) dividing the trochlear groove into the olecranon and coronoid process. This can mimic intraarticular osteophyte or healed ulnar fracture. C, D. T2-weighted coronal, sagittal MR images demonstrate pseudodefect of the capitellum (arrow). The junction between the smooth capitellum and the rough, nonarticular surface of the lateral epicondyle is abrupt and is accentuated with a trough-like undermining. The lateral capitellar margins overhang this trough. Thus, the capitellar overhanging edge with its groove beneath appears as a defect or notch. E. STIR coronal MR image shows lateral synovial fringe (arrow), which is a particular plica located between the capitellium and radial head. Page 10 of 29 Fig. 3: Normal anatomy of medial collateral ligament complex A. 3- dimensional schema demonstrates medial collateral ligament complex, composed of anterior (dashed arrow), posterior (arrow), and oblique (transverse, arrow head) bands. B. On T1-weighted coronal MR image, anterior band of medial collateral ligament is identified. Page 11 of 29 Fig. 4: Normal anatomy of lateral collateral ligament complex A-D. 3- dimensional schema (A) and T1-weighted coronal (B, C), axial (D) MR images demonstrate four components of lateral collateral ligament (LCL) complex, which are the lateral ulnar collateral (arrow heads), annular (dotted arrow), and radial collateral ligaments (arrow). Page 12 of 29 Fig. 5: 3- dimensional schema and T1-weighted coronal and axial MR images of normal elbow. A, C-E. The lateral muscle compartment includes four superficial extensor muscles in the forearm (extensor carpi ulnaris, extensor digiti minimi, extensor digitorum, and extensor carpi radialis brevis) which share a common tendinous attachment to the lateral epicondyle of the humerus. Extension of all joints crossed by the tendons. Extensor carpi radialis longus (ECRL), Extensor carpi radialis brevis (ECRB), Extensor digitorum (ED), Extensor carpi ulnaris (ECU). B, C-E. The medial muscle compartment includes the pronator teres and the four superficial flexors: the flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and flexor digitorum superficialis. Flexor digitorum superficialis (FDS), Flexor carpi ulnaris (FCU), Pronator teres (PT), Flexor carpi radialis (FCR). Page 13 of 29 Fig. 6: Normal anatomy of the elbow A. 3- dimensional schema demonstrates the anterior muscle compartment, comprised of the brachialis (asterisk) and biceps muscles (tendon, arrow), which flex the elbow. B. 3-dimensional schema shows the posterior muscle compartment, composed of the triceps, anconeus, and variably present anconeus epitrochlearis muscles. Tendon of triceps brachii is a powerful extensor of the elbow. The olecranon bursa lies between the olecranon and skin. C-E. T1-weighted sagittal and axial images show brachialis (asterisk), tendon of biceps muscles (arrow) and tendon of triceps brachii (arrowhead). Page 14 of 29 Fig. 7: Osteochondritis dissecans in a 14-year-old girl. She is an elite table tennis player with pain of the right elbow. Coronal T1-weighted images show an irregular subchondral bony lesion (A, arrow) with thin sclerotic rim in the anterolateral aspect of the capitellium. On fat suppressed T2-weighted images, thin hypersignal rim is seen between the seperated osteochondral fragment and parent bone. Mild bone marrow edema around the lesion is accompanied (B). Gd-enhanced fat suppressed T1 coronal and sagittal images show enhancement of the lesion (C, D). Page 15 of 29 Fig. 8: Medial collateral ligament tear. STIR coronal MR images revealed discontinuity with focal hypersignal intensity at the humeral attachment site of medial collateral ligament (arrow). Lateral collateral ligament (arrowheads) are intact. Page 16 of 29 Fig. 9: A 40-year-old man complained the elbow instability on hyperextension and varus stress after trauma. A, B. Proton density-weighted coronal MR images of right elbow show non-visualization of radial collateral ligament with widening of radio-capitellar joint space, indicating a complete tear. A small intraarticular body is seen. Medial collateral ligament (arrowheads) are intact. C. On STIR coronal MR image, bone marrow edema is prominent in the radial head and lateral epicondyle of the humerus. Page 17 of 29 Fig. 10: Lateral epicondylitis. A 52-year-old woman who had a chronic left elbow pain. Fat suppressed proton density-weighted coronal images revealed focal irregular hypersignal intensity lesion in the humeral attachment site of common extensor tendon (arrow). Page 18 of 29 Fig. 11: Medial epicondylitis in a 55-year-old woman with chronic left elbow pain. Gd-enhanced axial and coronal images show ill-defined enhancement at the humeral epicondyle insertion site of common flexor tendon (arrow) . Page 19 of 29 Fig. 12: Rupture of distal biceps tendon. Non-visualization of distal tendon with tendon retraction on T1-weighted sagittal and axial images (between the two pink lines in A), suggesting complete rupture of the distal biceps tendon. Page 20 of 29 Fig. 13: Triceps tendon rupture in a 52-year-old man presented posterior elbow pain. Gdenhanced fat saturated T1 sagittal images demonstrate discontinuity of triceps tendon at the olecranon insertion site and bone marrow edema with a possible small bony avulsion of the olecranon. Page 21 of 29 Fig. 14: Ulnar neuropathy in a 38-year-old man presented numbness on the left 4th and 5th fingers. Coronal T2-weighted images show mild swelling and increased signal of the ulnar nerve (A, arrow). Gd-enhanced coronal and axial T1-weighted images (B, C) show enhancement of the ulnar nerve is seen. On electromyogram and nerve conduction studies, ulnar neuropathy at the elbow level was confirmed. Page 22 of 29 Fig. 15: Radial neuropathy in a 38-year-old woman who had right wrist weakness. Axial T2-weighted images show high signal intensity at the brachialis (B), extensor carpi radialis (ECR), and extensor (Ex) muscles. Images by courtesy of Hong SH, MD. Fig. 16: Posterior interosseous neuropathy in a 29-year-old man presented right forearm weakness. T2 and contrast enhanced fat suppressed T1-weighted axial images reveal abnormal high signal intensity and mild enhancement of supinator (S), and extensor (Ex) muscles. Accompanied muscle atrophy is also noted. Images by courtesy of Hong SH, MD. Page 23 of 29 Fig. 17: Bicipitoradial bursitis in a 76-year-old woman presented a painful soft tissue mass in the anterior aspect of the right forearm during 1 month. T2-weighted axial (A) and Gd-enhanced T1-weighted axial and sagittal images (B, C) show fluid collection (arrow head) around the biceps tendon (arrow) with rim enhancement. Mild swelling of the biceps tendon is also noted. Page 24 of 29 Fig. 18: Olecranon bursitis in a 37-year-old man with painful swelling of the posterior elbow. He had a history of soft tissue scratch in the posterior aspect of the elbow 10 days ago. On T2-weighted axial images and contrast enhanced T1-weighted axial and sagittal images a loculated fluid collection in the overlying soft tissue of the ulnar olecranon is seen with rim enhancement. Adjacent soft tissue swelling is associated. Page 25 of 29 Conclusion MR imaging of the elbow is a useful and superior modality in evaluation of the elbow injuries. The accurate diagnosis of the injured elbow is based on a general consideration of the anatomy and biomechanics of this complex joint. A comprehensive knowledge of the normal and injured elbow can facilitate an accurate MR imaging diagnosis. Personal Information References 1. Regan WD, Korinek SL, Morrey BF, et al. Biomechanical study of ligaments around the elbow joint. Clin Orthop Rel Res 1991;271:170-9. 2. Zehava S. Rosenberg, Javier Beltran, MD Yvonne Yee Cheung. Pseudodefect ofthe Capitellum: Potential MR Imaging Pitfall Radiology 1994; 191:821-823. 3. O'Driscoll SW, Morrey BF, Korinek S, et al. Elbow subluxation and dislocation-a spectrum of instability. Clin Orthop Rel Res 1992;280:186-97. 4. Callaway GH, Field LD, Deng XH, et al. Biomechanical evaluation of the medial collateral ligament of the elbow. J Bone Joint Surg Am 1997;79A:1223-31. 5. O'Driscoll SW, Bell DF, Morrey BF. Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73A:440-6. 6. Olsen BS, Vaesel MT, Sojbjerg JO, et al. Lateral collateral ligament of the elbow joint: anatomy and kinematics. J Shoulder Elbow Surg 1996;5:103-12. 7. Dunning CE, Zarzour ZDS, Patterson SD, et al. Ligamentous stabilizers against posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 2001;83A:1823-8. 8. Giuffre BM, Moss MJ. Optimal positioning for MR imaging of the distal biceps brachii tendon: flexed abducted supinated view. Am J Roentgenol 2004; 182:944-6. 9. Belentani C, Pastore D, Wangwinyuvirat M, et al. Triceps brachii tendon: anatomicMR imaging study in cadavers with histologic correlation. Skeletal Radiol 2009;38:171-5. Page 26 of 29 10. Catherine L. Hayter, BrunoM. Giuffre. Overuse and traumatic injuries of the elbow. Magn Reson Imaging Clin N Am 2009;17:617-638. 11. Randall M. Patten. Overuse Syndromes and Injuries Involving the Elbow: MR Imaging Findings. Am J Roentgenol 1995;164:1205-1211. 12. Mitsunaga MM, Adishian DA, Bianco AJ Jr. Osteochondritis dissecans of the capitellum. J Trauma 1982;22:53-55. 13. Andrew H. Sonin, Steven W. Fitzgerald. MR imaging of sports injuries in the adult elbow: A tailored approach. Am J Roentgenol 1996;167:325-331. 14. Timmerman LA, Schwartz ML, Andrews JR. Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography. Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-31. 15. Field LD, Savoie FH. The arthroscopic evaluation and management of elbow trauma and instability. Oper Tech Sports Med 1998;6:22-8. 16. Bennett J, Tullos H. Acute injuries to the elbow. In: Nicholas J, Hershman E, editors. The upper extremity in sports medicine. St Louis (MO): Mosby; 1990. p. 326-7. 17. Schwartz ML, Alzahrani S, Morwessel RM, et al. Ulnar collateral ligament injury in the throwing athlete-evaluation with saline-enhanced MR arthrography. Radiology 1995;197:297-9. 18. Gaary EA, Potter HG, Altchek DW. Medial elbow pain the throwing athlete: MR imaging evaluation. Am J Roentgenol 1997;168:795-800 19. Nestor BJ, Odriscoll SW, Morrey BF. Ligamentous reconstruction for posoterolateral rotatory instability of the elbow. J Bone Joint SurgAm1992;74A:1235-41. 20. Coonrad RW, Hooper WR. Tennis elbow: its course, natural history, conservative and surgical management. J Bone Joint Surg Am 973;55:1177-82. 21. Morris M, Jobe FW, Perry J, et al. Electromyographic analysis of elbow function in tennis players. Am J Sports Med 1989;17:241-7. 22. Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am 1979;61:832-9. 23. Bredella MA, Tirman PFJ, Fritz RC, et al. MR imaging findings of lateral ulnar collateral ligament abnormalities in patients with lateral epicondylitis. Am J Roentgenol 1999;173:1379-82. Page 27 of 29 24. Stoller DW. The elbow. In: Stoller DW, ed. Magnetic resonance in orthopedics and sports medicine. Philadelphia: Lippincott, 1993:633-682. Skaf AY, Boutin RD, Dantas RWM, et al. Bicipitoradial bursitis: MR imaging findings in eight patients and anatomic data from contrast material opacification of bursae followed by routine radiography and MR imaging in cadavers. Radiology 1999;212:111-6. 37. Friedmann E. Rupture of distal biceps brachii tendon-report on 13 cases. JAMA 1963;184:60-3. 25. Campbell WW, Pridgeon RM, Sahni SK. Entrapment neuropathy of the ulnar nerve at its point of exit from the flexor carpi ulnaris muscle. Muscle Nerve 1988;11:467-70. 26. Martin CE, Schweitzer ME. MR imaging of epicondylitis. Skeletal Radiol 1998;27:133-8. 26. Nirschl RP. Elbow tendinosis/tennis elbow. Clin Sports Med 1992;11:851-27. Skaf AY, Boutin RD, Dantas RWM, et al. Bicipitoradial bursitis: MR imaging findings in eight patients and anatomic data from contrast material opacification of bursae followed by routine radiography and MR imaging in cadavers. Radiology 1999;212:111-6. 28. Friedmann E. Rupture of distal biceps brachii tendon-report on 13 cases. JAMA 1963;184:60-3. 29. Falchook FS, Zlatkin MB, Erbacher GE, et al. Rupture of the distal biceps tendonevaluation with MR imaging. Radiology 1994;190:659-63. 30. Williams BD, Schweitzer ME, Weishaupt D, et al. Partial tears of the distal biceps tendon: MR appearance and associated clinical findings. Skeletal Radiol 2001;30:560-4. 31. Safran MR. Elbow injuries in athletes-a review. Clin Orthop Rel Res 1995;310:257-77. 32. Herzog RJ. Magnetic Resonance Imaging of the elbow. Magn Reson Q 1993;9:188-210. 33. Gaines ST, Durbin RA, resonanceimaginginthediagnosis of 1990;20:607-11. Marsalka DS. The use of magnetic triceps tendon ruptures. Contemp Orthop 34. Kijowski R, Tuite M, Sanford M. Magnetic resonance imaging of the elbow. Part II: abnormalities of the ligaments, tendons, and nerves. Skeletal Radiol 2005;34:1-18. 35. Posner MA. Compressive neuropathies of the median and radial nerves at the elbow. Clin Sports Med 1990;9:343-63. Page 28 of 29 36. Lister GD, Belsole RB, Kleinert HE. The radial tunnel syndrome. J Hand Surg Am 1979;4:52-9. 37. Spinner M. The arcade of Frohse and its relationship to posterior interosseous nerve paralysis. J Bone Joint Surg Br 1968;50:809-12. 38. Andreisek G, Crook DW, Burg D, et al. Peripheral neuropathies of the median, radial, and ulnar nerves: MR imaging features. Radiographics 2006; 26:1267-87. 39. Abdalla Y. Skaf, Robert D. Boutin, Robert Weiber M. Dantas. BR bursitis. Radiolgy 1999;212:111-6. Page 29 of 29