Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
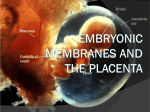
Foundation Year 2 Embryology Placenta and fetal membranes (ID#7104) Dr. Narayana Kilarkaje Figures or photographs used in this presentation are originally reproduced from Langman’s Medical Embryology by T. W. Sadler, 12th Edition, Lippincott Williams & Wilkins, for teaching purpose only. Objectives • Describe the formation of placenta • Describe structural and functional components of placenta • Describe the placental circulation • Describe structure of the placental barrier • Describe types of abnormal placenta • Describe fetal membranes- umbilical cord, amnion, chorion and allantois Fetal membranes Fetal membranes are: Amnion; chorion; yolk sac; allantois These develop from the zygote Amnion & chorion do not participate in the formation of the embryo or fetus Amnion and amniotic fluid is essential for fetal development Yolk sac is incorporated as primordium of gut • • Transfer of nutrients during 2nd and 3rd weeks of development Blood cells primordial germ cells develop in it Allantois has little function in humans Fetal membranes Functions of fetal membranes Protection Functions of placenta Exchange of metabolic & gaseous products between maternal & fetal bloodstreams Nutrtients & electrolytes Oxygen, carbon dioxide and carbon monoxide Maternal immunoglobulin G Production of hormones Human chorionic gonadotrophin Progesterone Estriol Somatomammotropin Formation of placenta Secondary villi Trophoblastic lacunae • Maternal sinusoid Connecting stalk • Primary villi Chorionic plate Chorionic Cavity 13-day-old embryo The placenta is formed by trophoblasts and chorion (from fetal side) and decidua (endomentrium) from maternal side Trophoblast forms an inner cytotrophoblast (CYT) and an outer syncytiotro-phoblast (SYN) layer • In SYN, lacunae appear, which establish contact with maternal sinusoids • Beginning of 3rd week- trophoblast forms primary villi (CYT covered by SYN) • Later, the extra-embryonic mesoderm grows into the CYT corethe villus is now called secondary villus Formation of placenta Tertiary villi Intervillous space SYN • End of 3rd week- somatic extraembryonic mesoderm (chorionic plate) cells transform into blood Cytotrophoblastic vessels (tertiary villus- functional shell villus) Connecting stalk Chorionic Plate Chorionic cavity 21-day-old embryo • The blood vessels in the villi establish contact with those in the chorionic plate and connecting stalk, through them with the blood vessels of the fetus • The CYT continues to grow until it reaches the endometrium forming an outer cellular covering known as cytotrophoblast shell (it attaches the embryo to the endometrium) Functional villi Maternal blood vessels Decidua basalis Anchoring villus Decidual septa Free villi Umbilical arteries 4-week-old placenta Umbilical vein Umbilical cord Covered with amnion • Villi are the finger-like projections, which freely bathe in intervillous spaces • Some villi from the chorionic plate reach the decidua basalis and attach-anchoring villi • From the anchoring villi, many finger-like free villi project into the intervillous space • In all tertiary villi branches of umbilical vein and umbilical arteries are present Different types of villi The villi are formed in 3 steps• Primary villi- CYT covered by SYN. • Secondary villi-extraembryonic mesoderm covered by CYT, in turn covered by SYN. • Tertiary villi- the blood vessels (fetal) grow into mesoderm. Structure of villi at various stages of development of placenta Cytotrophoblast shell Decidua • Spiral artery Intervillous space Cytotro phoblast Extraembryonic mesoderm Fetal blood vessel Chorionic plate Barrier formed by All 4 structures labeled Extraembryonic mesoderm Erosion of spiral arteries by cytotrophoblast cells results in entry of blood into intervillous spaces Barrier formed by 1. 2. Syncytiotrophoblast Endothelium Cytotrophoblast Syncytiotrophoblast A&C-4-week B&D-4-month • The CYT cells replace endothelial cells in spiral arteries making them large diameterlow resistance vessels The fate of cavities as fetus and placenta grow Myometrium Endometrium UTERUS Placenta Decidua Amnion Trophoblast And chorion Chorionic cavity Amniotic cavity Umbilical cord Amnion and chorion fuse; thus, chorionic cavity disappears Chorion Amniotic cavity Uterine cavity largely disappears due to chorion coming in contact with the uterine wall Placenta in the second half of pregnancy Junctional zone • The fetal side of placenta has chorionic plate and the maternal side has decidual (basal) plate • In between these 2 regions lie the villi and intervillous spaces • The decidual septa incompletely divide the intervillous space • Spiral arteries bring blood to intervillous spaces and endometrial veins drain the intervillous spaces into maternal system Full-term placenta • The full-term placenta weighs around 500-600g and measures 15-25 cm in diameter • It’s discoid-shaped • From maternal side, the placenta is divided into (by the septa) smaller lobules called cotyledons • Fetal side of the placenta is covered by chorionic plate, which is covered by amnion (not a part of placenta) • Umbilical cord is attached to the fetal surface, but the point of attachment varies Amnion and Umbilical cord • Connecting stalk transforms into umbilical cord • Amnion is formed by wall of amniotic cavity and extraembryonic mesoderm • Usually the cord has two umbilical arteries and one umbilical vein Fetal membranes in twins-Dizygotic (fraternal) • The frequency of twin births has been increasing in recent years due to late maternal age and assisted reproductive technologies (3.26% in US) 2-cell-stage zygote Amniotic cavity Yolk sac Chorionic cavity Fused placentas Chorionic cavity Separate placenta And chorion Fusion of placenta and chorion FIG. DIZYGOTC TWINS • 90% of twins are dizygotic • Due to 2 oocytes fertilized by 2 separate sperm • They are non-identical, may be of same or different sex • Generally, each zygote implants separately in the uterus, therefore, they have their own placenta, amnion and chorionic sac (A) • Sometimes, placentas and walls of chorionic sacs are fused (B) Fetal membranes in twins-monozygotic-identical 2-cell-stage zygote Inner cell mass Amniotic cavity Yolk sac Common placenta Blastocyst cavity Amniotic cavity Common CC Common AC CC- Chorionic cavity; AC-Amniotic cavity Develop from one fertilized ovum (34/1000) The zygote splits at various stages of development 1) At 2-cell stage (A):- Each embryo has its own placenta and chorionic sac -They are of same sex, have similar finger prints and external appearance 2) At early blastocyst stage (B): -Inner cell mas splits within same blastocyst cavity -They have common placenta and chorionic cavity but separate amniotic cavity 3) At bilaminar germ disc stage (C):Rare, they have single placenta, common chorionic cavity and amniotic cavity Abnormalities associated with twins • High incidence of mortality • Increased risk for preterm delivery • Low birth weight • Only 30% pregnant women with twin pregnancy give birth to two infants • Vanishing twin (fetus papyraceus): one fetus dies and resorbs during either first or second trimester Fetus papyraceus Twin transfusion syndrome Twin-Twin transfusion syndrome: • Occurs in monozygotic twins with single chorionic cavity • Placental vascular anastomosis occurs and only one fetus receives blood • One twin is smaller than the other; death occurs of both in 50-70% of cases Conjoined twins Conjoined twins: • Reason: Partial splitting of primitive node or primitive streak or mis-expression of certain genes such as Goosecoid • They are anatomically united but classified based on degree of fusion • Some of them are connected only by a skin bridge or liver bridge • Many of them survive; they can be surgically separated if they do not share any vital organs such as brain Reference reading TW Sadler. Langman’s Medical Embryology, 12th Edition, pages 100115.