Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
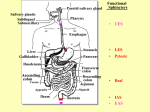
ALIMENTARY SYSTEM 1 (page 1 of 5) THE BURDEN OF GI DISEASE AND INTRO TO GI PHYSIOLOGY. Label a diagram of the alimentary system identifying the following: mouth, oesophagus, salivary glands, stomach, pancreas, liver, gall bladder, duodenum, jejunum, ileum, colon, rectum, and anus; mark on the diagram the position of the sphincters – gastro-oesophageal, pyloric, ileo-caecal, anal and sphincter of Oddi. ⇒ The blue labels indicate the salivary glands ⇒ The green shows the position of the sphincters. ⇒ The sphincter of Oddi is the one guarding the common bile duct) Gastro-oesophageal / Cardiac Pyloric Ileo-caecal Anal ⇒ GI tract is hollow tube from mouth to anus made of smooth muscle and lined by epithelium + associated structures (salivary glands, liver and pancreas): Mouth – oesophagus – stomach – small intestine (duodenum, ileum and jejunum) – colon (ascending, transverse and descending) – rectum - anus ⇒ Flow through tube regulated by activity smooth muscle and 4 sphincters (specialised regions of smooth muscle) – gastro-oesophageal, pyloric, ileo-caecal and anal ⇒ Bile (liver) and pancreatic secretions enter the duodenum via common bile duct and regulated by sphincter of Oddi Label a simple diagram of a typical gut wall section identifying: epithelial lining of gut lumen, mucosa, circular and longitudinal muscle, myenteric and submucosal plexuses and extrinsic nerves GUT EPITHELIUM Typically the gut wall has the epithelial lining (mucosa), 2 layers of smooth muscle (circular and longitudinal) and 2 nerve plexi (sub-mucosal and myenteric) MUCOSA - Lamina Propria (connective tissue) and Muscularis Mucosa SUBMUCOSAL PLEXUS CIRCULAR MUSCLE - Muscularis Mucosa (Smooth Muscle) - part of the Mucosa. MYENTERIC PLEXUS EXTRINSIC NERVES LONGITUDINAL MUSCLE MUSCLE (Muscularis Externa) State that the epithelium may be specialised for secretion or absorption, and invaginations may form glands of specialised cell types (gastric glands, Brunner’s glands), e.g. HCl parietal cells, pepsin chief cells Briefly explain the terms “intrinsic” and “extrinsic” nerve supply to the gut ⇒ Intrinsic the gut has an enteric nervous system comprising a submucosal plexus (containing sensory and motor neurons, and autonomic postganglionic fibres; it regulates movements of the mucosa and the vasculature tone, as well as controlling secretions) and the: myenteric plexus (which contains the same types of nerve fibers but controls mostly the motility of the GI tract, particularly the strength/frequency of contraction); the plexuses communicate with each other, and also within each other. ⇒ Extrinsic nerve supply is the nerve supply to the enteric nervous system; the autonomic innervation comes from the vagus and pelvic nerves, and also the sympathetic ganglia Gut neural plexi have multiple interconnections (“gut brain”) both within/between plexi as well as connections from external nerves of ANS. Both local and “long” (involving brain) reflexes are present. State that these nerves may modify secretion, absorption, motility and blood flow of the gut State that the extrinsic nerve supply has both a parasympathetic (mainly excitatory) and a sympathetic (mainly inhibitory) component State that mechano- and chemoreceptors in the gut wall may invoke both local reflexes involving the intrinsic nerve system and “long” reflexes involving the brain via afferent nerve fibres in the vagus and splanchnic nerves State that blood flow to the gut is about 30% of resting cardiac output and that venous drainage is via the hepatic portal vein which passes through the liver before returning to the heart State that activity of the gut muscles mixes contents with the digestive secretions and also aids efficient absorption of nutrients Describe the blood flow to the gut At rest, about 30% of the cardiac output goes to the gut – which can reduce to 5% in exercise; most blood returns to the vena cava via the liver (the hepatic portal vein) Distinguish between muscle activity involved in “mixing” movements and that involved in “propulsive” (peristalsis) activity Mixing (segmentation activity) is governed by the myenteric plexus, occurring in areas of the intestine with large volumes of chyme; a segmentation is initiated with the contraction of circular muscle which segments the intestine; then the muscle fibers within each segment contract; then the original contraction relaxes, and new contractions form; this creates a “sloshing” effect, occurring most rapidly in the duodenum (12/min); it mixes the food with digestive juices and also aids absorption by presenting “fresh” chyme to the mucosa Propulsive (peristalsis – migrating motility complex) is also governed by the myenteric plexus, and is characterised by a series of progressive contractions beginning in the lower part of the stomach and down to the terminal ileum within 2hrs; it is an organised movement and so requires an intact nervous system The stomach has a third layer of muscle (oblique) to grind the food before entry into the small intestine Describe how the structure of the mucosal lining of the gut leads to a large surface area for absorption There are mucosal folds (x3); the mucosa itself is made of a villus structure (x20); the luminal membrane of the epithelial cells has microvilli (x10) – a brush border; cumulative absorption area ~ tennis court (x600). State that the maximum rates of absorption of fat, protein and carbohydrate are about 10x greater than the normal daily rates ⇒ State that some 7 litres of water + ions are secreted into the lumen of the gut – this is equivalent to 50% of the extracellular volume- together with some 1.5l in the diet. Need to reabsorb most of this – faecal volume normally 100-150ml/day Explain the importance of reabsorption of this secreted fluid The total daily input to the GI tract (diet and secretions) is 9.5l, but you only shit around 100ml/day State that nearly all of the nutrients and most of the fluid secreted by the gut is reabsorbed in the small intestine No absorption occurs in the stomach, and only 1.4l occurs in the colon; reabsorption occurs due to osmosis (water follows the absorption of dietary nutrients) Describe how gut function is regulated by a combination of neural (both central and local), humoral and local paracrine activity; illustrate this with a suitable example Neural input (both extrinsic and intrinsic) controls absorption, blood flow, motility, secretions; humoral control originates from secretions from either the GI system (e.g. pancreas secreting secretin) or other glands (e.g. adrenal cortex secreting aldosterone); an example of local paracrine control is histamine release in the stomach An example of this integrated control is gastric acid secretion: Cephalic phase – neural response to sight, smell and taste of food, preparing the stomach before food actually gets there; this is mediated by ACh receptors on the parietal cells and the parasympathetic nervous system (via the vagus nerve); this stimulation also causes gastrin/histamine secretion Gastric phase – G-cells in the gastric antrum release the hormone gastrin; this is mediated by gastrin receptors on the parietal cells; this also causes histamine secretion - • • • Vagus - direct effect, also stimulates gastrin and histamine release Gastrin - direct effect and release histamine Histamine - direct effect Intestinal phase – digestive products in the lumen modulate local secretion (e.g. histamine producing ECL cells in the gastric mucosa: there are histamine receptors on parietal cells) The response to these stimuli cumulatively is greater than the sum of their action; there are also inhibitory mechanisms, for example somatostatin release from D-cells in the gastric antrum inhibit gastrin release SUMMARY: • Initiation - Vagus reflex starts acid before food enters stomach by both direct and indirect stimulation • Maintenance - Stretch of stomach wall by contents causes further release of gastrin (reflex involving intrinsic nerves) • Termination -Cessation vagal stimulants (food), emptying stomach reduces wall stretch- reflexes decrease. Other inhibitory mechanisms from small intestine State that GI disease is a diverse group of conditions that has a great impact on health and the quality of life and is associated with great economic burden List some common GI diseases Acid-related disease GORD (gastro-oesophageal reflux disease), Barrett’s oesophagus (pre-malignant lesion), peptic ulcer disease (Helicobacter infection, NSAID use) Chronic intestinal disease IBS (irritable bowel syndrome – disorder of motility, more prevalent among women), IBD (inflammatory bowel disease – a group of diseases, including Crohn’s disease, ulcerative colitis – associated with an ↑ risk of bowel cancer), diverticular disease (most commonly in females), and the shits Hepatobiliary disease chronic liver disease (injury to hepatocytes, inflammation for >6mnths, aetiology including viral, immunological and metabolic abnormalities), cirrhosis (permanent non-functioning tissue, hepatitis infection or alcohol most commonly), gallbladder disease (e.g. gallstones) Pancreatic disease acute pancreatitis (mild to life-threatening – blockage of pancreatic ducts, inflammation due to build up of enzymes), chronic pancreatitis (permanent damage usually due to alcohol) Gastrointestinal cancer colorectal (develops slowly and so great potential for medical screening and treatment), liver (difficult to detect at early stage, high metastasis risk), pancreatic (difficult to detect at early stage, with poor survival rate) Infections foodborne illness (>200 possible) and non-foodborne illness Ion transport mechanisms in the gut are important both for secretion and absorption processes – ⇒ Cell Junctions, basolateral K+, luminal Cl - (fluid secretion into intestine) Electro-chem gradient “Tight” - big gradient -stomach “Leaky” -small gradient -small intestine Colon in between ⇒ Ion Channels, ⇒ Ion Exchange Transporters (Na+/H+, Cl-/HCO3 -) Electro-chem gradient Electro-chem gradient Anion or cation - not both Anion or cation Ion specificity Ion specificity Open/closed Electroneutral ⇒ Active Transport Mechanisms using ATP (Basolateral sodium pump (Na+/K+), Proton pump (H+/K+) - gastric acid secretion by parietal cell) Much of the power driving ion movements is derived from the Na-gradient into the epithelial cells which is maintained by the ATP-driven activity of the sodium pump (Primary active transport). This gradient also powers the uptake of amino acids and glucose from the gut lumen into the absorptive cells of the epithelium § § § Movement against electro-chem gradient Uses ATP Ion specificity § § May be electrogenic May establish an electro-chem gradient