Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
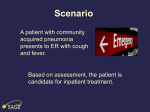
Hospital Documentation H&P Admit Note Admit Orders HISTORY AND PHYSICAL …is the FULL work up • SOAP format • Subjective – What is the patient telling you? • • • • • • • Chief Complaint History of Chief Complaint Review of Systems Past medical history Past surgical history Family history/social history Allergies/meds SOAP format • Objective – what do YOU find? • • • • Physical Lab X-ray Other studies • Assessment • Plan H&P • Chief Complaint • CC • If using patients’ words, use “quotations” • Ok to summarize • History of Chief Complaint • HCC or HxCC or HxPI • “quotations” if using patients’ words • Note if history is coming from someone other than the patient themself H & P cont. • Past medical/surgical history • Review of Systems • ROS • Pertinent positives AND negatives • Get into a “flow” • Is ok to have cheat sheets ROS • • • • • Integument/Skin HEENT CV Pulmonary GI • • • • • GU Neurologic Musc/Skeletal GYN Endocrine H&P cont • Family History/Social History/Job/Religion • Include habits here – smoking, alcohol, drugs • Medications • Don’t forget over the counter, vitamins and herbal supplements • Need to ask – most patients don’t consider these “meds” • Allergies • And what is the actual allergy (so you can distinguish from a side effect) H&P • Physical Exam • Again, use a logical flow • ALWAYS start with vital signs • BP, pulse, resp, temp, height, weight • OK to use cheat sheet here as well • Chart pertinent positives and negatives • Don’t make up acronyms • RRR is standard c/r/g/m/ is NOT H&P • Other – • • • • Lab X-ray Other studies Old record review H&P • Assessment • What does your physical and the lab, etc., lead you to find? • Ok to use symptoms if don’t have full diagnosis • DON’T use the OSCE format • No need to put 4 diagnoses here • If they have a history of something can put it here, but should NOT be the first listed • (and you want to make sure state Hx of..) Assessment, e.g. • Pneumonia • Hypokalemia • Hx HTN (or can say HTN – controlled) Plan – What are you going to do with the patient? • • • • • • Admit Start IV antibiotics Replace electrolytes (correct electrolytes, etc) Consult Pulmonary – anticipate bronchoscopy (ok to write see orders) Ok to write discussed the case with Dr. X (seen with Dr. x present, etc) ADMISSION (ADMIT) NOTE Admit Note • What you put as your first progress note • Abbreviated version of H & P • Can be the full H & P • Entitle “Admit/H &P” • No need to duplicate …MUST contain • • • • • CC Hx cc Pertinent physical (pertinent positives) Assessment Plan ADMISSION ORDERS …Instructions to the Nursing Staff • What do you want done for this patient now that they are coming into the hospital? • Systematic approach Admission Orders • Admit to service of (insert doctor) • Any special floor? (ICU, stepdown, telemetry) • • • • • Condition Allergies Vitals Activity Diet Admission Orders • Medications IV • Medications PO • These include any over the counter as well • • • • Labs X-ray Other studies Other …so for our pneumonia • • • • • ATSO Dr. Gail Feinberg Condition – stable NKDA Vitals (q 4 hours, q shift) Activity – • ABR with BRP (Absolute Bed Rest with Bathroom Privileges) • Ambulation with assistance, no limitations, etc Pneumonia cont • Diet – regular as tolerated (1800 cal ADA, salt restricted, cardiac – check with hospital to see how these are categorized) • Medications • IV – 1000cc D5W.5NS с 40meq KCL/liter @ 75cc/hr • Rocephin 1gm IV daily (DO NOT USE qd) • Xopenex nebs q8 hrs Pneumonia cont • Labs • Blood Culture prior to first dose IV antibiotic, sputum culture, CBC, CMP • CXR – PA and Lateral • Other • Oxygen per protocol (2liters NC, only at hs…) • Chest percussion after neb treatments • Incentive spirometry q shift Questions?