Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
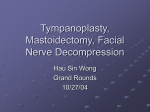
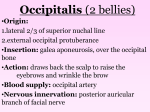
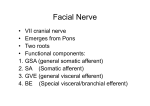
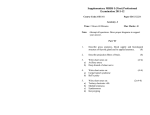
Pathology of the facial nerve: A pictorial review Poster No.: R-0215 Congress: 2014 CSM Type: Scientific Exhibit Authors: P. F. Kwan, R. Thomas; SOUTH YARRA/AU Keywords: Head and neck, Anatomy, CT, MR, Contrast agent-intravenous, Education, Education and training, Pathology DOI: 10.1594/ranzcr2014/R-0215 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply RANZCR/AIR/ACPSEM's endorsement, sponsorship or recommendation of the third party, information, product or service. RANZCR/AIR/ ACPSEM is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold RANZCR/AIR/ACPSEM harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, .ppt slideshows, .doc documents and any other multimedia files are not available in the pdf version of presentations. Page 1 of 18 Aim Introduction: Pathology affecting the facial nerve is often clinically devastating as the facial nerve provides motor innervation to the muscle of facial expression. Imaging plays a crucial role in the diagnosis of facial nerve pathology. However, radiologic diagnosis of facial nerve pathology can be challenging due to meandering and complex anatomy of the facial nerve. Methods and materials Anatomy of the facial nerve: The facial nerve has a motor nucleus and two sensory nuclei (superior salivatory nucleus (1) and solitarius tract nucleus) which are located in the ventrolateral pontine tegmentum. Motor fibers encircle the CN6 nucleus before emerges at the pontomedullary junction. The superior salivatory nucleus sends parasympathetic secretomotor fibers as nervus intermedius to the lacrimal, submandibular and sublingual glands. The solitary tract nucleus receives taste from the anterior two third of the tongue, with fibers travelling within the nervus intermedius. Cisternal segment: The motor nerve root joins the smaller sensory nervus intermedius, then emerges at the root exit zone in pontomedullary juction and travels anterolaterally in the cerebellopontine angle cistern. Internal acoustic canal (IAC) segment: From the porus accousticus, the facial nerve travels to the fundus of the IAC, in the anterior superior quadrant, above crista falciformis and anteriorly to Bill's bar. Labyrinthine segment: Page 2 of 18 This segment of the facial nerve travels anterolaterally from the IAC fundus to the geniculate ganglion (anterior genu). The greater superficial petrosal nerve arises from the geniculate ganglion, carrying parasympathetic fibers to the lacrimal gland. Tympanic segment: From the geniculate ganglion, the tympanic segment travels to the posterior genu, immediately beneath the lateral semicircular canal. Mastoid segment: Just distal to the pyramidal eminence (posterior genu), the nerve passes vertically downwards to the stylomastoid foramen. It has several branches including: 1. 2. Stapedius nerve supplies motor function to stapedius muscle. Chorda tympani carries secretomotor fibers to the submandibular and sublingual glands and taste fibers from anterior two thirds of tongue. Extratemporal segment: After exiting the stylomastoid foramen, this segment of the facial nerve gives off a sensory branch that supplies part of the external accoustic meatus and tympanic membrane. It then enters the parotid gland between the deep and superficial lobes, lateral to the retromandibular vein. This segment of the facial nerve gives off five terminal motor branches: temporal, zygomatic, buccal, mandibular and cervical. Normal enhancement of the facial nerve: The normal facial nerve can demonstrate enhancement along at least one segment (2) in 76% of cases, excluding the distal intrameatal and the labyrinthine segments. The geniculate ganglion, greater superficial petrosal nerve and the proximal tympanic (3) segment generally demonstrate faint enhancement. The cisternal, meatal, labyrinthine, and extracranial segments of the facial nerve do not normally enhance. Enhancement of these segments should raise the possibility of pathological involvement. Asymmetrical enhancement or irregular thickening of the geniculate ganglion, tympanic and mastoid segments should also be considered pathological. Page 3 of 18 Fig. 1: Facial nerve anatomy: Axial MRI images. a: IAC segment. b: labyrinthine segment. c: geniculate ganglion. d: tympanic segment. e: mastoid segment. References: Alfred Health - SOUTH YARRA/AU Fig. 2: Facial nerve anatomy: Coronal CT images. a: IAC segment. b: "snake eyes" appearance as the tympanic segment doubles back next to the labyrinthine segment adjacent to the cochlea. c,d: labyrinthine and tympanic segments converge at the geniculate ganglion. e: mastoid segment below the lateral semicircular canal. e: mastoid segment in the stylomastoid canal. References: Alfred Health - SOUTH YARRA/AU Results Common pathology affecting the facial nerve can be categorised as follow: Page 4 of 18 • • • • • • Neoplasm Infection Inflammation/Idiopathic Vascular Trauma Congenital Neoplasm Neoplastic process involving the facial nerve is rare. Several neoplastic processes which commonly involve the facial nerve include facial nerve schwannoma, hemangioma, perineural tumour spread from primary SCC or parotid gland malignancy, lipoma, glomus tumour and lipoma. Facial nerve schwannoma Facial nerve schwannoma is a rare benign tumour of Schwann cells that can affect anywhere along the facial nerve from its origin to its extracranial ramifications in the parotid space of the extracranial head and neck. It often affects multiple segments of the facial nerve with a predilection for the region around the geniculate ganglion. Patients may present with gradual facial nerve paralysis over many years or sensorineural hearing loss due to local mass effect from the tumour. (4) Imaging features: Enhancing mass in the cerebellopontine angle/internal acoustic canal extending and expanding into the labyrinthine canal ( "labyrinthine tail") and geniculate ganglion ( "icecream on cone" appearance). It is commonly iso to hypointense signal on T1 sequence and high signal on T2 sequence. They frequently enhance homogeneously, if small, and heterogeneously, if large. Large lesions may also demonstrate intramural cystic degeneration. Page 5 of 18 Fig. 3: Facial nerve schwannoma: Axial T1 post contrast images demonstrated an enhancing mass in the internal acoustic canal extending into the labyrinthine canal with an enlarged geniculate ganglion ( ice-cream on cone appearance). References: Alfred Health - SOUTH YARRA/AU Facial nerve haemangioma Facial nerve haemangioma is a rare vascular malfomation, often arising from region around the geniculate ganglion. Patients with hemangiomas that originate in the geniculate fossa most often present with facial nerve paralysis that is slowly progressive (5) over the course of several weeks. Sensorineural hearing loss and pulsatile tinnitus may (6) occur if there is erosion of the cochlear otic capsule. Imaging features: Enhancing mass centred at the geniculate ganglion, with permeative or honeycomb bone matrix on CT. Tumour size ranges from 2mm to 2cm. The lesion may spread along the greater superficial petrosal nerve anteromedially if large. Page 6 of 18 Fig. 4: Facial haemangioma: Enhancing mass centred at the geniculate ganglion on contrast enhanced MRI, with permeative bone matrix on CT. References: Alfred Health - SOUTH YARRA/AU Perineural tumour spread Several malignant tumours of the parotid gland can spread along the facial nerve. These tumours include adenoid cystic carcinoma, mucoepidermoid carcinoma, adenocarcinoma, malignant mixed tumors, acinic cell carcinoma, lymphoma, squamous (7) cell carcinoma and melanoma metastases. Adenoid cystic carcinoma has the highest (8) tendency to cause perineural tumour spread (70 -75%) and it is the most common malignancy to cause perineural spread along the facial nerve. Imaging features: Irregular, tubular enhancement along extracranial and intratemporal segment of the facial nerve , extending from an enhancing intraparotid mass. The perineural tumour spread may be contiguous or skipped and it can extend proximally up to the cisternal segment. Page 7 of 18 Fig. 5: Perineural tumour spread: Enhancing primary skin SCC with parotid nodal metastasis and thickened, nodular perineural tumour spread along the extracranial and mastoid segment of the facial nerve. References: Alfred Health - SOUTH YARRA/AU Glomus tumour Glomus tumour, also known as paraganglioma, is a rare benign vascular tumour that arises from the paraganglia cells. Depending on its location, glomus tumours of the head and neck can be divided into glomus tympanicum, jugulare, vagale and carotid body tumour. Facial nerve paralysis is a rare symptom/complication of glomus tympanicum (5%). More common presentations are pulsatile tinnitus and conductive hearing loss. Imaging features: Glomus tympanicum appears as an enhancing mass on the cochlear promontory with "salt and pepper" appearance on MRI. Salt and pepper appearance refers to punctate hyperintensity (salt) and flow voids (pepper) on T1 weighted images. Small lesions may be difficult to see on CT, but large lesions cause permeative destructive bone changes, with erosion of the middle ear cavity and ossicles. Glomus jugulotympanicum may extend from the cochear promontory to the jugular foramen, with the same imaging appearances described above. Page 8 of 18 Fig. 6: Glomus jugulotympanicum : Enhancing tumour with "salt and pepper" appearance, centred in the jugular foramen with permeative destructive bone changes on CT. The tumour extends laterally involving the mastoid segment and superiorly involving the IAC segment of the facial nerve. References: Alfred Health - SOUTH YARRA/AU Infection Acute or chronic infection of the middle ear and mastoid can spread to the facial nerve due to its course within the temporal bone. Cholesteatoma affecting the middle ear also has the potential to erode into the intratemporal segment of the facial nerve. Otomastoiditis Acute or chronic otomastoiditis is an infection affecting the middle ear and mastoid air cells, usually affecting young children and most commonly due to bacterial infection. Complications of otomastoiditis are rare, as the disease is usually responsive to prompt antibiotic treatment. However, complications of otomastoiditis may occur due to antibiotic resistance, or in immunocompromised patients. The complications include coalescent mastoiditis, petrous apicitis, labyrinthitis, facial nerve paralysis and hearing loss. Page 9 of 18 Imaging features: Middle ear and mastoid opacification on CT. In coalescent mastoiditis, there is erosion of the mastoid septation and cortex. On MRI, there is T1 isointense and T2 hyperintense inflammatory debris, with diffuse enhancement within the middle ear and mastoid. The facial nerve is most commonly affected in its tympanic and upper mastoid segments. In cases of acute otomastoiditis, the lesion is often not destructive (9) and reversible. Fig. 7: Acute otomastoiditis: Enhancing tissue in the middle ear and mastoid air cells. There is also enhancement of the mastoid segment of the facial nerve which lies in the region of the inflammatory phlegmon, in keeping with facial nerve involvement. Soft tissue opacitication in the middle ear and mastoid air cells on CT. No erosion of the mastoid septation and cortex to indicate coalescent mastoiditis. Page 10 of 18 References: Alfred Health - SOUTH YARRA/AU Inflammation/idiopathic Several inflammatory/ idiopathic conditions are known to affect the facial nerve. These conditions are Bell's palsy, Guillain-Barré Syndrome, sarcoidosis, multiple sclerosis and wegener's granulomatosis. Guillain-Barré Syndrome Guillain-Barré Syndrome is an acute inflammatory demyelinating polyradiculopathy of uncertain aetiology. Miller Fisher Syndrome is a variant of Guillain- Barré Syndrome which involves the cranial nerves. Patients may present with the clinical triad of opthalmoplegia, ataxia and areflexia. In most cases, multiple cranial nerves are involved, and the facial nerve can be involved up to 27 - 50% and often bilaterally. usually a history of preceding respiratory or gastrointestinal viral illness. (10) There is Imaging features: Bilateral enhancement of the infratemporal facial nerve, often involving the IAC fundus, labyrinthine segment, geniculate ganglion, tympanic and mastoid segments. Page 11 of 18 Fig. 8: Guillain-Barré Syndrome : Bilateral enhancement of the IAC fundus , labyrinthine segment, geniculate ganglion, tympanic and mastoid segments of the facial nerves. References: Alfred Health - SOUTH YARRA/AU Bell's palsy Bell's palsy is a rapidly progressive facial nerve paralysis. It is thought to be due to reactivation of latent herpes simplex virus in the geniculate ganglion. Imaging features: Vivid asymmetrical enhancement of the facial nerve, commonly on either side of the geniculate ganglion - in the fundal and labyrinthine segments. The infratemporal segment may also be affected. Page 12 of 18 Fig. 9: Bell's palsy: Vivid asymmetrical enhancement of the left IAC fundus, labyrinthine, geniculate ganglion, tympanic and mastoid segments of the facial nerve.. References: Alfred Health - SOUTH YARRA/AU Neurovascular compression The facial nerve may be compressed by a vascular loop, usually at its root exit zone in the cerebellopontine angle cistern, causing hemifacial spasm. The vascular loop may be the anterior inferior cerebellar artery (most common), posterior inferior cerebellar artery or vertebral artery. Less commonly, the facial nerve may be compressed within the internal acoustic canal (11) by a vascular loop. Imaging features: High resolution T2 weighted sequence (FIESTA) demonstrating a serpigenous vascular loop contacting and displacing the facial nerve, most commonly at its root exit zone, but could also be in the internal acoustic canal. Page 13 of 18 Fig. 10: Neurovascular compression: Long slender right AICA (red arrow) contacting and displacing the facial nerve (yellow arrow) in the internal acoustic canal causing hemifacial spasm. A piece of surgical Teflon (blue arrow) has been inserted in between the AICA and the right facial nerve with good post operative outcome. References: Alfred Health - SOUTH YARRA/AU Trauma Temporal bone fracture Temporal bone fracture occurs with severe blunt trauma to the skull. Temporal bone fracture is traditionally described as longitudinal, transverse or mixed type according to radiographic anatomical involvement. However, there is a newer system which classifies the temporal bone fracture according to otic capsule violating or sparing in order to predict clinical sequelae of trauma. Whilst longitudinal fractures (75-80%) are more common than transverse fractures, facial nerve injury is reported to occur in only 25% of longitudinal and 40% to 50% of transverse fractures. (12) Fractures that do not violate the otic capsule are much less likely to damage the cochleovestibular system or the facial nerve, owing to the protective density of the otic (13) capsule bone. In Dahiya and colleagues' study of 55 temporal bone fractures, patients with otic capsule-violating fractures were more than twice as likely to have facial nerve injury, 4 times as likely to have CSF leakage, and 7 times as likely to have SNHL than those with otic capsule-sparing fractures. Imaging features: Longitudinal fracture typically runs parallel to the petrous pyramid through the middle ear. Transverse fractures run perpendicular to the petrous ridge, from the foramen magnum across the petrous pyramid. Transverse fractures often affect the labyrinthine segment, while longitudinal fractures more often affect the geniculate ganglion, tympanic and mastoid segment. Page 14 of 18 Fig. 11: Temporal bone Trauma: Longitudinal temporal bone fracture extending through the geniculate ganglion and tympanic segment of the facial nerve causing facial nerve palsy. References: Alfred Health - SOUTH YARRA/AU Congenital malformations: There are multiple congenital anomalies affecting the facial nerve, including facial nerve canal dehiscences, facial nerve aplasia/hypoplasia, duplicated IAC, and many congenital syndromes such as Möbius, DiGeorge, Goldenhar, CHARGE, trisomy 13, and trisomy 18. Page 15 of 18 Fig. 12: Möbius syndrome : Hypoplastic right facial nerve (yellow arrow) and absent left facial nerve (blue arrow)in a child with bilateral facial and abducens nerves palsy. References: Dr Yune Kwong, Radiopaedia Conclusion Conclusion Page 16 of 18 Understanding of the anatomy and pathology of the facial nerve will improve one's ability to diagnose. This article reviews the radiologic findings of several common pathologies that affect the facial nerve. Personal information Pei Fun Kwan MRI Fellow Alfred Health [email protected] Rosemarie Thomas Body Fellow Alfred Health [email protected] References (1) Sinnatamby CS, Last RJ. Last's anatomy, regional and applied. Churchill Livingstone. (1999) ISBN:0443056110. (2) Gebarski SS, Telian SA, Niparko JK. Enhancement along the normal facial nerve in the facial canal: MR imaging and anatomic correlation. Radiology 1992;183:391-4 (3) Tien R, Dillon WE, Jackler RK. Contrast-enhanced MR imaging of the facial nerve in 11 patients with Bell's palsy. AJNR Am J Neuroradiol 1990;155:573-9 (4) Wiggins RH, Harnsberger HR, Salzman KL et-al. The many faces of facial nerve schwannoma. AJNR Am J Neuroradiol. 2006;27 (3): 694-9. Page 17 of 18 (5) Salib RJ, Tziambazis E, McDermott AL, Chavda SV, Irving RM. The crucial role of imaging in detection of facial nerve haemangiomas. J Laryngol Otol 2001;115(6):510-513. (6) Mangham CA, Carberry JN, Brackmann DE. Management of intratemporal vascular tumors. Laryngoscope 1981;91(6):867-876. (7) Sachin Gupta, Francine Mends, Mari Hagiwara, Girish Fatterpekar, and Pamela C. Roehm, "Imaging the Facial Nerve: A Contemporary Review," Radiology Research and Practice, vol. 2013, Article ID 248039, 14 pages, 2013. doi:10.1155/2013/248039 (8) A. S. Garden, R. S. Weber, W. H. Morrison, K. K. Ang, and L. J. Peters, "The influence of positive margins and nerve invasion in adenoid cystic carcinoma of the head and neck treated with surgery and radiation," International Journal of Radiation Oncology Biology Physics, vol. 32, no. 3, pp. 619-626, 1995. (9) Vazquez E, Castellote A, Piqueras J et-al. RadioGraphics. 2003;23 (2): doi:10.1148/ rg.232025076 (10) Kilic R, Ozdek A, Felek S, Safak MA, Samim E. A case presentation of Bilateral Simultaneous Bell's Palsy. Americal Journal of Otolaryngology. 2003;24:271-273. doi: 10.1016/S0196-0709(03)00050-4. (11) Pego Reigosa R and Pulpeiro Rios JR. Hemifacial spasm. J Neurol Neurosurg Psychiatry 1998 64: 687. doi: 10.1136/jnnp.64.5.687 (12) Little SC, Kesser BW. Radiographic classification of temporal bone fractures: clinical predictability using a new system. Arch. Otolaryngol. Head Neck Surg. 2006;132 (12): 1300-4. doi:10.1001/archotol.132.12.1300 - Pubmed citation (13) Dahiya R Keller JDLitofsky NSBankey PEBonassar LJMegerian CA Temporal bone fractures: otic capsule sparing versus otic capsule violating clinical and radiographic considerations. J Trauma 1999;471079- 1083 Page 18 of 18