Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
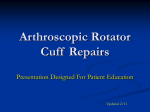
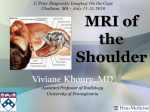
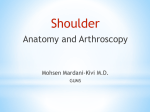
■ tips & techniques The Abduction External Rotation (ABER) View for MRI of the Shoulder Jaideep J. Iyengar, MD; Keith R. Burnett, MD; Wesley M. Nottage, MD The ABER view is an excellent tool for detecting subtle soft tissue pathology of the anteroinferior labrum and rotator cuff and is strongly advocated for all contrastenhanced imaging of the shoulder. S houlder magnetic resonance imaging (MRI) is the gold standard imaging modality for evaluating soft tissue in the shoulder joint. The abduction external rotation (ABER) view has been discussed in the literature as an excellent tool beyond the conventional 3 sequences (coronal, sagittal, and axial) for accurately assessing anteroinferior labral detachment and both partial- and fullthickness tears of the rotator cuff tendons.1-5 Placing the arm in an abducted and externally rotated position tensions the anteroinferior glenohumeral ligament and labrum. If a labral detachment is present, contrast solution defines the defect. Likewise, abduction and external rotation of the arm releases tension on the cuff relative to the normal coronal view obtained with the arm in adduction. As a result, subtle articular-sided partial thickness flap tears will not lie Drs Iyengar and Nottage are from The Sports Clinic Orthopaedic Medical Associates, Inc, Laguna Hills, and Dr Burnett is from Laguna Niguel MRI, Inc, Laguna Niguel, California. Drs Iyengar, Burnett, and Nottage have no relevant financial relationships to disclose. The authors thank Arif Ali, MD, Eric M. Price, MD, Gen Marayama, MD, and Anthony Stauffer, MD, for their preliminary work on this article, and Phil Pador, MRI technician, for his assistance in providing the images for the article. Correspondence should be addressed to: Keith R. Burnett, MD, Laguna Niguel MRI, Inc, 25500 Rancho Niguel Rd, Ste 140, Laguna Niguel, CA 92677 ([email protected]). doi: 10.3928/01477447-20100625-17 562 ORTHO0810Iyengar.indd 562 apposed to the adjacent intact fibers of the remaining rotator cuff nor be effaced against the humeral head, and intra-articular or intravenous contrast can enhance visualization of the tear.6 In addition, tears with a horizontal component are identified and characterized with increased sensitivity with the ABER view.4 The ABER view is a modified axial view. Because the orientation of the ABER view differs from the traditional images that orthopedists are accustomed to viewing, its interpretation can be confusing for those with limited or no experience. Furthermore, the execution of the ABER view can be a challenge for the technologist unfamiliar with its use. This article addresses the method by which the ABER technique is performed and the regional anatomy that can be seen on these MRI scans. TECHNIQUE Orthopedists consider 90⬚ of abduction and 90⬚ of external rotation the position of apprehension. However, most 1 Figure 1: ABER positioning. Note that the classically used ABER position for arthrography is not the true 90⬚90⬚ position that orthopedists would typically consider to be the position of abduction and external rotation. conventional bore-style MRI scanners do not allow for the shoulder to be placed in this position. The narrow confines of a closed tube usually necessitate use of the more commonly performed position for the ABER view with the arm abducted and the hand tucked beneath the patient’s head, so as to lessen the mediolateral dimension of the patient’s upper torso (Figure 1). Settings The ABER scout views are first obtained by acquiring images along a plane parallel to the long axis of the humerus ORTHOPEDICS | ORTHOSuperSite.com 7/29/2010 11:15:25 AM ■ tips & techniques 2 3 4A Figure 2: ABER scout view. Note the orientation is parallel to the humeral shaft and perpendicular to the glenohumeral articulation. Figure 3: Classic ABER view of a normal shoulder. Because the arm is externally rotated, the expanse of the supraspinatus footprint insertion assumes a posterior position (white arrow). Abbreviations: G, glenoid; H, humerus; L, labrum. Figure 4: Saline arthrogram ABER view with T2 fat-saturation technique. The appearance is similar to a T1-weighted image with contrast (A). A low-field MRI ABER view with no fat separation. Note the rotator cable, seen on this image as the lump in the center of the rotator cuff undersurface (B). Figure 5: ABER is a modified axial view. It is important to realize that anterior structures (ie, coracoid process) are in the lower left quadrant and posterior structures are in the upper right quadrant. Note the long head of the biceps tendon (white arrow) posteriorly as it traverses down the humerus. Abbreviations: C, coracoid; G, glenoid; H, humerus. (Figure 2). Once the orientation is set with respect to the shaft of the humerus, the plane with respect to the scapula is determined. The position of the patient’s arm can vary based on size, flexibility, and comfort. The ABER plane is chosen so that a stack of images are obtained at right angles to the glenohumeral articulation, extending between the supraglenoid tubercle and axillary recess. If the patient assumed a 90⬚-90⬚ position of the arm, as might be obtained in a vertical field open-sided scanner, the images of the glenoid and scapula would be much the same as those seen in true axial imaging. However, most ABER views result in unique representations of scapular bony landmarks, each of which is a variation of a true axial image of the scapula. This occurs because the orientation is based on the humeral shaft rather than the scapula. The ABER sequence, like all magnetic resonance arthrographic sequences, is gener- ally obtained as T1-weighted to enhance the definition of injected contrast, which appears white (Figure 3). Further definition is provided by the use of a method that includes suppression of fat signal in the bone marrow and soft tissue around the joint. At magnetic fields ⬎1 T, this requires spectral fat saturation; at magnetic fields ⬍1 T, a special form of fat separation is used. Typically, both of these techniques are lumped together under the rubric of fat suppression. Acquisition parameters for both high and low field are relatively similar with the exception of applying either fat saturation or fat separation techniques as appropriate based on the magnet strength. Although technically different approaches, the output is nearly equivalent. Should the patient be allergic to gadolinium or suffer from renal failure, one may alternatively achieve capsular distention and sufficient fluid contrast with intra-articular saline solution. If so, the ABER view is not precluded and im- AUGUST 2010 | Volume 33 • Number 8 ORTHO0810Iyengar.indd 563 ages can be obtained with a T2-weighted sequence and fat saturation (Figure 4). Interpretation Conventional axial MRIs are oriented such that posterior structures are displayed toward the lower edge of the frame, and anterior structures are in the superior margin of the frame, irrespective of which shoulder is scanned. However, the ABER view rotates the image 90⬚. The ABER view is a glenohumeral view that is essentially axial to the scapula but coronal to the humerus. Therefore, the anterior structures of the humerus (ie, long head of the biceps tendon) are rotated to the superior glenoid and the cuff is rotated posteriorly, adjacent to the scapular spine (Figure 5). To avoid confusion and enhance ease of interpretation, we recommend adoption of the following convention for display of all ABER sequences. The scapular spine is always displayed to the viewer’s right, placing the rotator cuff also on 4B 5 the right, the anterior glenoid on the left, and the shaft of the humerus toward the top. This display protocol will maximize consistent recognition of anatomic structures and pathological lesions, especially of the rotator cuff and labrum, independent of which side is imaged. The ABER view can enhance interpretive and diagnostic accuracy for several types of pathology in the shoulder. The ABER series can be a useful adjunct in the diagnosis of articular-sided partial thickness and full thickness rotator cuff tears (Figure 6A). A recent meta-analysis comparing the relative accuracies of magnetic resonance arthrography, conventional MRI, and ultrasound in diagnosing rotator cuff tears concluded that magnetic resonance arthrography had superior sensitivity and specificity in diagnosing both full- and partial-thickness tears than the other 2 modalities.7 Similarly, labral pathology can be difficult to assess on physical examination and/or 563 7/29/2010 11:15:28 AM ■ tips & techniques 6A 8A conventional MRI sequences. The ABER series improves visualization of labral tears in younger patients, especially of the posterior superior labrum and superior labral anterior posterior (SLAP) tears in throwing athletes, as well as Bankart lesions associated with shoulder dislocations or instability events (Figure 6B). In many cases, lesions found on the ABER views are not present on conventional coronal or axial MRI sequences and would have otherwise been missed (Figure 7). The ABER sequence is particularly useful in the case of partial-thickness rotator cuff tears, where diagnostic accuracy continues to present a challenge for conventional MRI or even ultrasound (Figure 8). DISCUSSION Despite the clear diagnostic advantages of the ABER sequence, adoption has not been 564 ORTHO0810Iyengar.indd 564 6B 8B ubiquitous.8,9 This fact is confirmed by the informal polling of our sports medicine fellows and the attendees and faculty at a yearly international conference exclusively devoted to shoulder surgery (K. Burnett, oral communication, 20052008). While the issue has not been systematically investigated, we postulate several responsible factors. Adding the sequence prolongs examination time by approximately 25% (including positioning), potentially detracting from time available to other patient needs and decreasing efficient use of limited scanner resources. Also, the ABER positioning is uncomfortable for some patients and can detract from the patient’s perception of the testing experience. For a few patients, typically those with a history of multiple shoulder dislocations, the positioning itself may be intolerable due to apprehension. Nevertheless, 7A 7B Figure 6: Undersurface partial-thickness tears and full-thickness supraspinatus tears are well visualized with an image in the middle of the ABER series (contrast extending into the tendon defect, white arrow) (A). Inferior image in the ABER series is useful for visualizing any labral pathology (depicting a posterior labral lesion, white arrow), including Bankart lesions when present (B). Figure 7: Conventional axial MRI shows only a poorly defined anterior labral abnormality (A). ABER view clearly demonstrates the labral pathology that otherwise could have been easily missed (white arrow) (B). Figure 8: Conventional coronal MRI in this patient demonstrated no evidence of rotator cuff tear (A). However, ABER view showed a typical partial-thickness rotator cuff tear with articular-sided flap and delamination propagation that otherwise would have been overlooked (white arrow) (B). the ABER noncompliance rate for all MRI remains low, but is likely between 1% and 3% (K. Burnett, oral communication, 2003-2009). Busy departments may not wish to add time to their scans, and low-volume facilities may not be able to cope with the complexities required to perform, display, or interpret the images with care and competence. Recent publications have highlighted circumstances that favor either adding the ABER sequence or even substituting the ABER sequence for a conventional series. There are advocates for the indirect magnetic resonance arthrogram (intravenous as opposed to intra-articular injection).6 Although this examination has its own limitations and interpretive pitfalls, adding the ABER sequence has been reported to enhance sensitivity and specificity for the diagnosis of partial- and full-thickness cuff tears. The ABER view should be considered mandatory when indirect magnetic resonance arthrograms are used.6 There may also be situations where patients cannot tolerate much imaging time (eg, claustrophobia, restless leg syndrome, or mild dementia) and a full conventional arthrogram is out of the question. For these patients, a recent article has highlighted the feasibility and accuracy of substituting 1 ABER sequence for the entire conventional arthrogram as a reasonable and accurate alternative for the diagnosis of rotator cuff tears.8 CONCLUSION The ABER view is an excellent tool for detecting subtle soft tissue pathology of the anteroinferior labrum and rotator cuff. A standard display format enhances anatomical understanding and facilitates the teaching of interpretative principles and pit- ORTHOPEDICS | ORTHOSuperSite.com 7/29/2010 11:15:32 AM ■ tips & techniques falls. The ABER sequence is strongly advocated for all contrast-enhanced imaging of the shoulder, whether it is intra-articularly or intravenously administered. Surprisingly, the inherent sensitivity and specificity of ABER qualifies it as a standin for the entire conventional 3plane examination, should circumstances require. REFERENCES 1. Cvitanic O, Tirman PF, Feller JF, Bost FW, Minter J, Carroll KW. Using abduction and external rotation of the shoulder to increase the sensitivity of MR arthrography in revealing tears of the anterior glenoid labrum. AJR Am J Roentgenol. 1997; 169(3):837-844. 2. Wintzell G, Larsson H, Larsson S. Indirect MR arthrography of anterior shoulder instability in the ABER and the apprehension test positions: a prospective comparative study of two different shoulder positions during MRI using intravenous gadodiamide contrast for enhancement of the joint fluid. Skeletal Radiol. 1998; 27(9):488-494. 3. Tirman PF, Bost FW, Steinbach LS, et al. MR arthrographic depiction of tears of the rotator cuff: benefit of abduction and external rotation of the arm. Radiology. 1994; 192(3):851-856. 4. Lee SY, Lee JK. Horizontal component of partial-thickness tears of rotator cuff: imaging characteristics and comparison of ABER view with oblique coronal view at MR arthrography initial results. Radiology. 2002; 224(2):470-476. 7. de Jesus JO, Parker L, Frangos AJ, Nazarian LN. Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: a meta-analysis. AJR Am J Roentgenol. 2009; 192(6):1701-1707. 5. Choi JA, Suh SI, Kim BH, et al. Comparison between conventional MR arthrography and abduction and external rotation MR arthrography in revealing tears of the antero-inferior glenoid labrum. Korean J Radiol. 2001; 2(4):216-221. 8. Schreinemachers SA, van der Hulst VP, Willems WJ, Bipat S, van der Woude HJ. Detection of partial-thickness supraspinatus tendon tears: is a single direct MR arthrography series in ABER position as accurate as conventional MR arthrography? Skeletal Radiol. 2009; 38(10):967-975. 6. Herold T, Bachthaler M, Hamer OW, et al. Indirect MR arthrography of the shoulder: use of abduction and external rotation to detect full- and partial-thickness tears of the supraspinatus tendon. Radiology. 2006; 240(1):152-160. 9. Saleem AM, Lee JK, Novak LM. Usefulness of the abduction and external rotation views in shoulder MR arthrography. AJR Am J Roentgenol. 2008; 191(4):1024-1030. Section Editor: Steven F. Harwin, MD AUGUST 2010 | Volume 33 • Number 8 ORTHO0810Iyengar.indd 565 565 7/29/2010 11:15:36 AM