Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
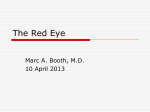
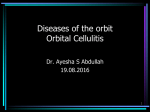
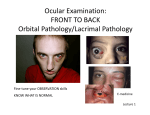
Table of Contents 1 Orbital and lid disorders o 1.1 Preseptal (Periorbital) Cellulitis o 1.2 Orbital Cellulitis o 1.3 Ptosis o 1.4 Proptosis 2 Disorders of the Lacrimal System o 2.1 Treatment of blocked tear ducts o 2.2 Amnniotocele (mucocele) of the lacrimal sac 3 Serious Early Childhood Eye Conditions o 3.1 Leukocoria (white pupil) o 3.2 Retinoblastoma o 3.3 Congenital Cataract o 3.4 Congenital and Infantile Glaucoma References 1 Orbital and lid disorders The orbit is the focus point for many ocular conditions and due attention should be given to the investigation of the orbit and periorbital tissue in an eye examination. The following section provides some information about relatively common (and serious) disorders of the orbit and lid. [ top ] 1.1 Preseptal (Periorbital) Cellulitis Illustration: Preseptal cellulitis in a young boy Definition! Preseptal cellulitis is an infection in the space between the orbital septum and the skin of the eyelid. This is a not uncommon entity usually seen in the under five year old. There is often an antecedent respiratory tract infection. Spread to the preseptal space (ie on front of the orbital septum but behind the skin of the eyelid) is usually haematogenous, but infection in this space following trauma or complicating external ocular infection can occur. There is a well-demarcated pink or purplish swelling of the lids which are very oedematous. There are no signs, such as proptosis or reduced ocular motility, indicating involvement of intra orbital structures. Affected children are usually febrile and may be severely ill. The pathogens are usually Staph aureus or respiratory pathogens such as Haemophilus influenzae or Strep pyogenes. Blood cultures should always be obtained before starting treatment with intravenous antibiotics. HiB vaccination is reducing the incidence and severity of this disorder. [ top ] 1.2 Orbital Cellulitis Orbital cellulitis refers to severe inflammation (usually due to infection) within the orbit. True orbital cellulitis is less common than preseptal cellulitis and is usually seen in children older than five years. The onset is acute with signs of orbital soft tissue involvement such as proptosis, chemosis and limited ocular motility. Most cases are caused by spreading from infected sinuses. Vision may be lost due to optic neuritis. Culture from the conjunctiva is often misleading. Blood cultures should always be taken. CT scanning of the orbit and sinuses should be undertaken in all cases of orbital cellulitis and in cases of preseptal cellulitis where there is doubt whether infection is contained in the preseptal space. Caution! Children with orbital cellulitis run the risk of developing cavernous sinus thrombosis, meningitis, brain abscess or septicaemia. Both preseptal and orbital cellulitis are potentially life threatening and parenteral antibiotics are strongly recommended. Topical antibiotics are useless as they do not penetrate into the soft tissue spaces involved. [ top ] 1.3 Ptosis Ptosis in children is most commonly caused by a maldevelopment of the levator muscle of the upper lid (congenital ptosis). Other causes can be classified under myogenic (eg myasthenia gravis), neurogenic (eg third nerve palsy) or mechanical (eg plexiform neuroma). Congenital ptosis is usually a cosmetic problem and is usually corrected surgically before entry into preschool. The ptotic lid can, however, induce astigmatism which often produces amblyopia so ophthalmic assessment is recommended when the diagnosis is made in infancy. If the lid is so ptotic that it covers the pupil urgent surgery is indicated. [ top ] 1.4 Proptosis Proptosis in children is rare. Overall, the majority of cases of slowly developing proptosis are due to an intraorbital dermoid cyst. Illustration: Proptosis in a young girl Caution! Rapidly developing proptosis in a child should always raise the possibility of rhabdomyosarcoma although acute bleeding into a lymphangioma (chocolate cyst) is also a common cause. There is a large differential diagnosis of orbital tumours in children. The removal of all but superficial orbital tumours such as external angular dermoids is now usually undertaken by ophthalmologists with subspecialty training in orbital surgery. Complex cases may require a combined approach involving, for instance, ophthalmologists, neurosurgeons and craniofacial surgeons. [ top ] 2 Disorders of the Lacrimal System Blockage of the naso-lacrimal duct usually presents in the first few months of life with epiphora (watering eyes) or as mild recurrent conjunctivitis. The nasolacrimal duct, which connects the lacrimal sac to the nasal cavity begins to form by about the sixth week of gestation and canalises from the sixth month. About two per cent of babies will have symptomatic blockage of the nasolacrimal duct. Caution! Blockage of the nasolacrimal duct is not the only cause of watering eyes in infancy. Do not forget to exclude corneal disease such as a corneal foreign body or ulcer. Congenital glaucoma also occasionally presents as a watering eye, often associated with photophobia, often has an enlarged cornea with a ground glass appearance. The possibility of ophthalmia neonatorum should be considered in any neonate with a purulent discharge from the eyes. [ top ] 2.1 Treatment of blocked tear ducts The usual treatment in cases which are not infected is to massage the lacrimal sac (see below). Massage of the lacrimal sac has been shown to result in a higher rate of spontaneous cure when compared to "masterly inactivity". It is not necessary to treat all cases of blocked tear ducts with antibiotics. Frank purulent conjunctivitis should be treated with a short course of antibiotic drops second hourly for three days. Caution! Chloramphenicol drops should not be used as a long term treatment due to the risk of bone marrow suppression. Most cases of nasolacrimal duct obstruction resolve spontaneously by six to nine months of age. In a child with recurrent infections or where epiphora is particularly troublesome, probing is indicated, usually after the age of six months. If the child's eyes are still watering after twelve months of age, probing is almost always necessary as there is almost no spontaneous resolution after age one year. Teaching the Technique of Lacrimal Sac Massage to the Parent The technique of lacrimal sac massage should be taught to the parent for several reasons: the spontaneous regression rate is higher when massage is used, the likelihood of infection in the tear sac is probably reduced if the sac is periodically emptied and lastly it gives the mother something to do as the doctor demonstrates `masterly inactivity' while awaiting a spontaneous cure. The mother should be shown (on herself), where to find the lacrimal crest (the sharp edged buttress of bone at the nasal end of the inferior orbital margin) behind which is found the lacrimal sac. Make sure that the mother's fingernail is short. The index finger is passed posteriorly over the lacrimal crest. Pressure is then applied nasally and inferiorly with a sideways rocking motion. The sac itself is not normally palpable. If the sac is full of mucopus, the contents will be regurgitated back into the conjunctival sac where they can be wiped away. Massage once or twice a day is all that is necessary. Practice Tip! Make sure that the mother's fingernail is short. Advise the parent to wash the finger carefully after massaging the lacrimal sac to avoid the development of paronychia. [ top ] 2.2 Amnniotocele (mucocele) of the lacrimal sac This is an uncommon condition which presents in the neonatal period with a blue swelling of the lacrimal sac often extending onto the side of the nose. This condition is always associated with blockage of the nasolacrimal duct and the mucocele may extend down into the nasal cavity and produce nasal obstruction. Simple massage again may cure this condition but dacryocystitis quite commonly develops and requires surgical drainage. Probing then becomes necessary once the infection has settled down. [ top ] 3 Serious Early Childhood Eye Conditions There are several very serious ocular conditions in childhood that may present to the GP. While conclusive diagnosis of these conditions may be difficult and beyond the scope of the primary practitioner, it is absolutely imperative not to miss the cardinal signs of these diseases. Delay in referral may lead to permanent irreversible blindness. Caution! RARE DISEASES PRESENT TO COMMON DOCTORS [ top ] 3.1 Leukocoria (white pupil) Mothers frequently notice an `abnormal' appearance to the pupil or eye before a white pupil is obvious to the doctor. Ignore this complaint at your peril. Leukocoria is an uncommon condition, with a large differential diagnosis, which almost always indicates severe eye disease. The general practitioner has a crucial role in obtaining an early diagnosis which may, in some cases, prove to be life saving. [ top ] 3.2 Retinoblastoma This is the commonest intraocular malignancy in childhood. It usually presents within the first three years of life with a white pupil or 'cats eye' reflex. The tumour assumes several forms within the eye but it usually looks like a whitish mass on the retina. The other common presenting sign is a squint, caused by loss of the fixation reflex when the macula is involved by the tumour. Illustration: Retinoblastoma in an infant (Photo courtesy of John Crompton, Department of Ophthalmology, Royal Adelaide Hospital) Most cases arise as new mutations. If both eyes are involved or if the disease is multifocal in one eye, it may be assumed that the disease has arisen as a result of a germinal mutation. In these cases, the tumour will be subsequently transmitted as an autosomal dominant condition with greater than 80% penetrance to the patient's children. In 6 - 8% of patients there will be a positive family history. Advances in the understanding of the molecular biology of the retinoblastoma gene are presently at the forefront of genetic research. Within affected families, the identification of carriers of the gene in utero is likely in the near future. In carriers of the gene, there is a long term risk of a second malignancy such as an osteogenic sarcoma. Illustration: Retinoblastoma in an infant (Photo courtesy of John Crompton, Department of Ophthalmology, Royal Adelaide Hospital) Golden Rule! If the diagnosis of retinoblastoma is suspected, urgent referral to an ophthalmologist versed in the management of retinoblastoma is indicated. Treatment undertaken at an early stage is life saving. After confirmation of the diagnosis, management usually involves enucleation of the affected eye if the sight cannot be saved or, if there is visual potential, chemotherapy to shrink the tumour followed by laser or cryotherapy to the residual tumour. Local irradiation may also be used. Laser or cryotherapy alone can be used for small tumours or local recurrences. [ top ] 3.3 Congenital Cataract This is the most common cause of leukocoria. It may be unilateral or bilateral. The aetiology of congenital cataracts can be either hereditary, infectious (eg rubella), metabolic (eg galactosaemia) or associated with a syndrome (eg Down syndrome). The trend towards early diagnosis and treatment in paediatric ophthalmology is nowhere better illustrated than in the case of congenital cataract. The prevention of the tragedy of the congenital rubella syndrome by immunisation lies firmly within the province of the family doctor. Golden Rule! Congenital cataract should be excluded in all newborn children by confirming the presence of a normal red fundus reflex in both eyes (use a direct ophthalmoscope at arms length in a darkened room) prior to discharge home. Early treatment (before three months of age) of congenital cataract gets results - late treatment is doomed to failure because of the development of deprivation amblyopia and sensory deprivation nystagmus. Golden Rule! Any child who has had cataract surgery in infancy must have whole of life follow-up because of the long term risk of glaucoma (30%) and retinal detachment. [ top ] 3.4 Congenital and Infantile Glaucoma This is a form of glaucoma which usually has its onset in the first three years of life. It may be present at birth and can involve one or both eyes. The presenting symptoms are epiphora (tearing) and photophobia. Because the infant eye is distensible, the corneal diameter increases giving the 'ox-eye' appearance (buphthalmos). Any child with a corneal diameter greater than 12mm has glaucoma until proven otherwise. As a result of corneal enlargement, tears may develop in Descemet's membrane, leading to corneal oedema which produces a `ground glass' appearance. The disease may occur in isolation or as part of a syndrome eg Sturge-Weber syndrome. The treatment of congenital glaucoma is almost always surgical, usually by opening an abnormal trabecular meshwork by goniotomy or trabeculotomy. Approximately 80% of patients will be cured by surgery. [ top ] References 1. Gole, G.A. May 2001, PAEDIATRIC OPHTHALMOLOGY NOTES 2001, Dept of Ophthalmology, Royal Children's Hospital, Brisbane. 2. Simon, J.W., Kaw, P. Aug 2001, 'Commonly Missed Diagnosis in the Childhood Eye Examination', American Family Physician,vol. 64, no. 4,pp. 623-8