Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
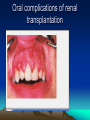
Blood and nutrition, endocrine disturbances, and renal disease Disorders of the blood • It is well known that lesions of the oral mucosa may occur in patients with abnormalities of the blood. In particular, the appearance of glossitis or angular cheilitis in anaemic patients has often been described Anaemias • The characteristic feature of anaemia is a reduction in the level of haemoglobin, which is usually accompanied by a decreased number of erythrocytes. The red cells (erythrocytes) are the circulating cells predominantly concerned with the transport of oxygen to the tissues by means of the iron-containing substance haemoglobin within them Most of the Pt • The great majority of these patients are suffering from anaemias of various kinds and, hence, the major interest is centred on this group of conditions, but it must be borne in mind that abnormalities of the white cell and platelet components of the blood may also be reflected in oral changes. Types of Aneamia • Megaloblastic anaemias • Iron deficiency anaemia • Haemolytic anaemias • SICKLE-CELL DISEASES Megaloblastic anaemias • Vitamin B12 or folic acid deficiency are the most common causes of anaemias with macrocytosis. Pernicious anaemia is an autoimmune condition causing atrophy of the gastric mucosa (atrophic gastritis) and consequent failure to secrete intrinsic factor due to an anti-intrinsic factor antibody. • Therefore, in patients with this condition antibodies to intrinsic factor may be detected in the blood. More complex malabsorption syndromes may also occur, involving failure to absorb not only vitamin B12, but also folic acid and iron compounds. The term megaloblastic anaemia refers to the change in size and structure of the basic marrow cell from which the erythrocytes are derivedâ Iron deficiency anaemia • A much more common cause of anaemia than failure to absorb vitamin B12 or folic acid is iron deficiency, which leads to inadequate haemoglobin synthesis. The deficiency may be due either to inadequate intake of iron or to excessive blood loss as in menstrual abnormality or gastrointestinal bleeding Haemolytic anaemias • There is a further group of anaemias, the haemolytic anaemias, in which the essential abnormality is an increase in the rate of erythrocyte destruction. Under normal conditions, the red cells last for about 100 days, but in haemolytic anaemias their life may be reduced to only a few days. • Haemolytic anaemias may be due to an intrinsic defect or may be acquired—an important, although relatively uncommon, cause of the acquired form being the effect of some drugs • (However, the most important haemolytic anaemia in terms of dental practice is sickle-cell anaemia, although this condition is somewhat different from the others under consideration in that its major significance to the dentist is not in the production of oral lesions. SICKLE-CELL DISEASES • sickling may occur in conditions of low oxygen tension and, if this change does take place, the oxygen-carrying capacity of the blood is greatly reduced with the consequent possibility of anoxia in the patient Oral signs and symptoms of haematinic deficiencies • Glossitis Smooth, depapillated tongue (iron deficiency) Raw, beefy tongue (vitamin B12 and folate deficiencies) Oral candidosis (including angular cheilitis) Exacerbation of RAS Plummer–Vinson syndrome (iron deficiency Orofacial manifestations • Orofacial manifestations of sickle-cell anaemia include prominence of the maxilla and mandible and orofacial pain. These occur as a result of marrow hyperplasia and expansion of the marrow space due to a longstanding haemolytic anaemia. Destructive osteomyelitis is a recognized complication of dental infection in sickle cell disease Oral signs and symptoms in anaemias Management of patients with anaemias and haematinic deficiencies • Ninba waayihiisaa Waala lootumaa Xalka • In the majority of the patients described, treatment of the underlying haematological deficiency leads to a rapid resolution or improvement in the oral symptoms. In patients with longstanding latent iron deficiency, however, the response may be a slow one Leukaemia • Leukaemia represents a malignant proliferation of white cells, replacing their normal development in the bone marrow. This process may affect any of the white cell strains, but the most usual forms are lymphocytic, monocytic, and myeloid, depending on whether lymphocytes, monocytes, or granulocytes are involved. Each of these forms of leukaemia present either in an acute or a chronic form oral signs • It is not uncommon for oral signs and symptoms to be the first indication of the presence of leukaemia, particularly of one of the acute types The gingivae are frequently involved with a hyperplastic gingivitis. The hyperplastic gingivitis results in fragile red spongy gingivae that bleed spontaneously or following slight injury. Orofacial manifestations of acute leukaemia • Spontaneous haemorrhage for gingivae (reduction in platelets) Oral purpura and petechiae Gingival swelling (leukaemic infiltration) Oral ulceration (leukaemic deposits, infections, haematinic deficiencies) Mucosal swelling and loosening (exfoliation) of teeth (leukaemic deposits) Opportunistic infections (e.g. herpes, Candida) Lymph node enlargement *N.B. Chemotherapy to treat leukaemia may also produce oral side-effects Leukaemia haemorragic In more advanced cases • In more advanced cases of leukaemia, oral ulceration is very common. The ulcers, produced by the breakdown of the tissues overlying deposits of leukaemic cells, may be large, painful, and difficult to treat. The maintenance of oral hygiene may be of great help in reducing the distressing oral symptoms in these patients Leukopenia • Leukopenia represents a fall in the white cell content of the blood. This may be a spontaneously arising condition, but may occur also as a response to drug therapy. Carbamazepine has been associated with severe haematological effects, including leukopenia and aplastic anaemia Leukopenia • Leukopenia may also occur as a transient stage in the development of leukaemia and other diseases affecting the bone marrow. It may also result from autoimmune disorders such as systemic lupus erythematosus (SLE) and viral infections; particularly HIV/ infections. clinical presentation • the most usual clinical presentation is of agranulocytosis. This represents a reduction in the number of granulocytes formed in the marrow and circulating in the blood. The effect of this is to increase the susceptibility of the patient to infections of various kinds In the case of the oral mucosa • In the case of the oral mucosa this may lead to widespread infection and ulceration of all parts of the mucosa. These changes may not be dissimilar to those occurring in leukaemia Platelet abnormalities • When the function or the number of the platelets in the circulating blood is reduced, there is a tendency for spontaneous haemorrhage to occur within the tissues. This may well show initially in the form of petechial haemorrhages on the oral mucosa and these are, in fact, a wellknown sign of early immune thrombocytopenia In leukaemias • In leukaemias of various kinds, both platelet function and numbers are greatly reduced, and haemorrhages of mucosa and skin may therefore be an early warning sign. • It is advisable to carry out a full blood screen, including a platelet count, on any patient with otherwise unexplained areas of haemorrhage affecting the oral mucosa. It should be remembered, however, that transient haemorrhages of this kind may occur on the soft palate in patients with a severe cold Oral medicine patients who should be considered for an extended haematological examination • Patients with recurrent aphthous stomatitis (RAS) Patients with a persistently sore and/or dry mouth Patients with oral lesions with an atypical history or unusually resistant to treatment Patients complaining of a sore or burning mouth or tongue, or abnormal taste sensation, even though no mucosal • changes can be seen All patients with persistent oral and orofacial candidosis Patients showing abnormalities following an initial screening Disorders of nutrition • The integrity of the oral mucous membrane is maintained by a wideranging complex of factors, including those dependent on adequate nutrition. The significance of iron metabolism and associated factors Nutritional deficiencies • A wide range of conditions that depend on the absence or reduction of certain specific nutritional factors, particularly vitamins, conditions are now rarely seen under European conditions, although It should be remembered • It should be remembered that a nutritional deficiency may occur in three ways: (1) as a result of reduced intake; (2) as a result of faulty absorption or metabolism; and (3) as a result of increased excretion. The relationship of iron deficiency anaemia to these three factors is a good and simple example. Endocrine disturbances • In general, changes in the oral mucosa dictated by endocrine abnormalities are not common. Perhaps the most frequently cited changes are those due to the endocrine disturbances found in normal life—especially during pregnancy, and at the menopause. It should be remembered • It should be remembered that endocrine disorders are highly complex and often involve a number of systems because of the feedback mechanisms that control the endocrine system as a whole. It is,difficult • It is, therefore, often difficult to determine the exact effect of a single endocrine abnormality on any structure. Endocrine disorders affecting bone and teeth (gigantism, acromegaly, and hyperparathyroidism laakin • Hypoparathyroidism resulting from parathyroid or thyroid surgery has no particular effects on the orofacial tissues but results in a low serum calcium. Tetany is the clinical manifestation of reduced serum calcium. Normal endocrine changes Pregnancy • During pregnancy, the hormonal changes that occur may have the effect of exacerbating a previously existing chronic gingivitis that may have been previously symptom-free and unrecognized Theresulting gingivitis • Theresulting gingivitis is essentially hyperplastic, although there is minimal proliferation of fibroblasts. The most marked proliferation is of capillaries and this leads to the typically purple coloration of the gingival papillae (Fig. 13.4). These papillae tend to be fragile and may bleed at the least injury • Because of the presence of false pocketing and bleeding, stagnation and secondary infection may occur, and may lead to halitosis Pregnancy gingivits Adrenocortical diseases Addison's disease • Addison's disease is the result of lack of function of the adrenal cortex, usually the result of an autoimmune disorder, but with other possible aetiologies • The oral change of significance in Addison's disease is melanotic pigmentation of the oral mucosa, which may include the buccal mucosa, gingivae, and palate Hypothyroidism • Hypothyroidism in adults is often autoimmune but may occur as a consequence of excessive removal of the thyroid gland to treat hyperthyroidism. Acquired hypothyroidism (myxoedema) manifests as weight gain, inability to tolerate cold, dry skin, loss of hair, and a slowing down of activity and mental processes Hypothyroidism • Hypothyroidism is associated with an impaired immune mechanism and oral candidosis may be the result. There is often a relationship between pernicious anaemia and hypothyroidism—possibly in the family if not in the individual. Congenital hypothyroidism • Congenital hypothyroidism (cretinism) is characterized by dwarfism and mental retardation. Orofacial signs include enlargement of the tongue , defective facial development, and delayed eruption of the teeth Diabetes mellitus • Diabetes mellitus is a common endocrine disorder that occurs as a result of a deficiency of insulin or resistance to insulin. Two clinical types are recognized: juvenile onset (insulin-dependent, type 1) and maturity onset diabetes (type 2). Diabetes mellitus has no • Diabetes mellitus has no specific oral signs or symptoms. However, possibly because of the general lack of resistance to infection of the diabetic patient, periodontal disease processes may become exaggerated It is not uncommon to find that an undiagnosed diabetic presents with advanced periodontal disease. , the dental surgeon must always remember • The principles of treatment of this are simply those of periodontal treatment in the nondiabetic patient. However, in this and in all other treatment, the dental surgeon must always remember that the diabetic patient is more than normally susceptible to infection Oral features of diabetes mellitus • Dry mouth Compromised periodontal health* Oral candidosis Glossodynia Lichenoid drug reactions (oral hypoglycaemic drugs • *Depends on oral hygiene. Renal disease • Renal disease is of great significance in oral medicine and general dental practice. Oral changes occur not only as a result of chronic renal failure but also as a consequence of the medical management of renal disease. The dental management of patients with renal disease may also need to be modified to prevent complications. Chronic renal failure • Chronic renal failure (CRF) is irreversible deterioration in renal function. When plasma creatinine persistently exceeds 300 µmol/l (normal range 80–120 µmol/l), there is progressive deterioration in renal function, irrespective of aetiology. glomerular filtration rate When the plasma creatinine reaches 1000 µmol/l, dialysis will be required. The glomerular filtration rate (GFT; normal, 120 ml/min) measures renal function. Progressive impairment in function of the kidneys leads to the development of the clinical syndrome of uraemia Orofacial manifestations of chronic renal failure • Chronic renal failure and its resultant uraemia cause a number of physiological changes that can cause oral symptoms Orofacial manifestations of chronic renal failure • Dry mouth Mucosal ulceration Bacterial and fungal plaques Pallor of the mucosa (anaemia) Oral purpura White plaques (uraemic stomatitis) Giant cell lesions—osteolytic lesions in jaws Giant cell lesions of the jaws • Giant cell lesions of the jaws may occur as a result of hyperparathyroidism secondary to renal failure (or prolonged dialysis) and give rise to oral lesions or osteolytic lesions in the bone. Patients with CRF are now treated with potent alphahydroxylated vitamin D supplements to prevent secondary hyperpathyroidism • Great care must be taken when prescribing drugs for patients with renal failure and the safest drugs to use are those that are metabolized primarily by the liver. Dosages of other drugs need to be adjusted to compensate for decreased renal excretion Renal transplant patients • Renal transplantation, either from a tissuematched cadaver or close relative, offers the best hope of a normal life. However, it is not without problems, mainly due to the side-effects of immunosuppressive regimens given to prevent rejection of the transplanted kidney doses of corticosteroids • In the past large doses of corticosteroids gave rise to considerable short- and longterm problems (see Chapter 3). Renal transplant patients pose a number of dental and medical management problems Oral complications of renal transplantation • Drug-induced gingival overgrowth (hyperplasia) Bacterial and fungal plaques Increased incidence of oral malignancy (reported) Oral candidosis Herpes simplex infections (secondary) Oral complications of renal transplantation Immunodeficiency, hypersensitivity, autoimmunity, and oral reactions to drug therapy • Bacdaa dhuuqsoy • Baalweynta Yaan lagaa boojeynine!!! Immunodeficiency • Immunodeficiencies may be classified as primary or secondary. Primary immunodeficiencies represent an intrinsic failure in development of one or more parts of the immune system and are often genetically based. They can be predominantly B- or T-cell defects, a combination of both, or due to a selective immunodeficiency (for example, IgA deficiency Afew individuals are born • Afew individuals are born with gross primary immunodeficiencies. These may result in life-threatening conditions and the affected individuals tend to die young, often as a result of recurrent infections. Candida infections are often predominant in these patients (see Chapter 4) who suffer from aphthous-like ulceration and herpes infections. They are also more susceptible to periodontal disease. IgA • IgA deficiency is relatively more common than other primary immunodeficiencies—levels of IgA are decreased in both serum and saliva. Secondary immunodeficiency • The immune system is composed of a variety of cells, especially white blood cells, and proteins, for which one of the principal functions is microbial defense. A deficit in the immune system can therefore lead to unusually severe or uncommon recurrent infections. Immune deficits (immunodeficiency) may be primary or secondary.. Secondary immune • Secondary immune deficiencies or acquired deficiencies, more frequent than primary immune deficiencies, are problems of the immune system that are not genetic and which are caused by external factors An example of a secondary immune deficiency: AIDS • The most well-known example of a secondary immune deficiency is the immunodeficiency caused by the human immunodeficiency virus, or HIV. HIV attacks certain cells in the immune system and prevents them from carrying out their proper functions against microbes • . When the immune system is sufficiently weakened, infected people catch atypical and severe infections. This is then called the Acquired Immunodeficiency Syndrome, or AIDS. AIDS at this time is often treated by a specialized multidisciplinary team. What are other causes of secondary immunodeficiency? • Dhantadu Dhimataye • Dhulkey kudhacdee • Dhantada Dhulka maad kaqadaney Other causes • Other causes of secondary immunodeficiency include: severe malnutrition, certain chronic diseases such as diabetes, immunosuppressive medication or chemotherapy, certain cancers such as leukemia, and the absence of the spleen (sometimes the spleen must be removed because of trauma, for example). How are secondary immunodeficiencies treated? The treatment depends on the severity in the deficiency of the immune system. Treatment of the underlying cause often leads to improvement of the condition. Patients are typically followed by their usual physician: the allergist-immunologist may be consulted in certain cases.