Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Program Of Master of Public Health in Biostatistics
516 705: Statistical Methods in Clinical Trials
Effect of percutaneous transvenous mitral
commissurotomy
on resolution of left atrial thrombus
in mitral stenosis patients
Protocol
January 2001
Advisor: Bandit Thinkhamrop, Ph.D.
Student: Truong Nguyen, MD
Principal investigator: Songkwan Silaruks, MD
Department of Biostatistics and Demography
Faculty of Public Health
Khon Kaen University
1
Table of contents
1.SUMMARY ................................................................................................................................... 2
2.DESCRIPTION OF THE PROJECT ......................................................................................... 3
2.1.INTRODUCTION AND IDENTIFICATION THE PROBLEM .............................................................. 3
2.2.JUSTIFICATION ......................................................................................................................... 3
2.3.GOALS AND OBJECTIVES .......................................................................................................... 3
2.4.HYPOTHESIS ............................................................................................................................. 4
3.STUDY DESIGN ........................................................................................................................... 5
3.1.INTERVENTIONS ....................................................................................................................... 5
3.1.1.Experimental arm: OA and PTMC ................................................................................... 5
3.1.2.Control arm: OA only ....................................................................................................... 5
3.2.METHODOLOGY ....................................................................................................................... 5
3.2.1.Study population:.............................................................................................................. 5
3.2.2.Sample size: ...................................................................................................................... 5
3.2.3.Random allocation technique: .......................................................................................... 6
3.2.4.Blinding: ........................................................................................................................... 6
3.2.5.Outcome and outcome measurement:............................................................................... 7
3.2.6.Follow-up procedures: ..................................................................................................... 7
3.3.DATA ANALYSIS ....................................................................................................................... 9
Interim analysis: ........................................................................................................................ 9
Stopping rules:........................................................................................................................... 9
3.4.ETHICAL CONSIDERATION ...................................................................................................... 10
4.DURATION OF THE TRIAL ................................................................................................... 10
5.EXPECTED OUTCOME OF THE STUDY ............................................................................ 10
6.BUDGET ...................................................................................................................................... 10
7.REFERENCES ............................................................................................................................ 10
8.APPENDICES ............................................................................................................................. 11
APPENDIX 8.1 ............................................................................................................................... 12
Study information .................................................................................................................... 12
Consent form ........................................................................................................................... 14
APPENDIX 8.2 DATA COLLECTION FORM ...................................................................................... 15
APPENDIX 8.3 DUMMY TABLES .................................................................................................... 17
Table 1. Characteristics of patients at trial entry ................................................................... 17
Table 2. The different rate of complete LAT resolution after 4 and 6 months of treatment .... 17
of NYHA functional class and complication between two group ............................................ 17
Table 3. Multivariate logistic regression results: treatment effects on complete LAT ............ 18
resolution adjusted for potential confounding factors............................................................. 18
APPENDIX 8.4 TIMELINE FOR THE TRIAL ...................................................................................... 19
APPENDIX 8.5.ALGORITHM FOR RECORDING ALL PATIENTS DURING THE TRIAL PERIOD ............ 20
APPENDIX 8.6 ............................................................................................................................... 21
Allocation instructions............................................................................................................. 21
Sequence of treatment allocating ............................................................................................ 22
2
1.Summary
Background:
Mitral stenosis (MS) is one of a common life-threatening health problem in the developing
countries. Approximately 25% of MS patients have thrombus in left atrium. This will
frequently lead to systemic embolism. The optimal treatment to remove the thrombus is to
perform surgery. However percutaneous transvenous mitral commissurotomy (PTMC) has
become an effective and safe alternative to surgical treatment of severe MS but the
presence of left atrial thrombus (LAT) is generally considered a contraindication to this
procedure. Additionally, in developing countries, surgical treatment is not only far too
expensive but also can not meet the increasing demand. Patients have to wait for the
surgery for approximately 9 - 15 months. While they were waiting, they must take an oral
anticoagulant (OA) regularly. By this, LAT of some patients were dissolved and thus can
perform PTMC safely. Successful resolution of LAT has been reported in our previous
study. However the duration of LAT to disappear is considerably long, i.e., the mean
duration of LAT resolution was 16 months. This means the MS patients are taking the risk
of embolism during this period. Another study conducted by some of our members showed
that PTMC could be performed safely if thrombus is confined in LA appendage. We belief
that the improvement of hemodynamic status may enhances the resolution of the thrombus.
Thus the combination of PTMC and OA is expected to shorten the duration of LAT
resolution. Therefor, a randomized controlled trial is needed to demonstrate that. Findings
from this trial will contribute enormously to the developing world. Aside from saving life
and improving the quality of life of the patients, replacing surgery with PTMC and OA
combined could save a large amount of money per year.
Objective:
The main objective is to compare the rate of complete LAT resolution between treated by
OA only and the combination PTMC and OA at 4 and 6 months after treatment.
Methods:
This will be a hospital-based, parallel, single blind, randomized controlled trial. Study
subjects refer to MS patients with thrombus confined in LA appendage who do not have
absolute contraindications of performing PTMC, and their hemodynamic status are stable.
We exclude those who have contraindications of performing TEE, or not satisfy the
conditions of performing PTMC right after randomization, or pregnant. The primary
outcome is complete LAT resolution at 4 and 6 months after the treatment. Subjects will be
randomly allocated to be treated by OA only or combination OA and PTMC using block
randomization with varied block size of 2, 4, and 6. The sample size of 115 for each arm
was planned to have the power of 80% to detect 10-20% difference rates of complete LAT
resolution after 4 months of treatment between the two arms, with significance level of
0 . 0 5 ,
t w o - s i d e d
t e s t .
3
2.Description of the project
2.1.Introduction and identification the problem
Rheumatic heart disease, sequelae of rheumatic fever, is more common in developing than
developed countries. As a result, mitral stenosis (MS) is higher in the developing ones.
Approximately 25% of MS patients have thrombus in left atrium. This will frequently lead
to systemic embolism. The optimal treatment to remove the thrombus is to perform
surgery. However percutaneous transvenous mitral commissurotomy (PTMC) has become
an effective and safe alternative to surgical treatment of severe MS, particularly when
regurgitation and valvular calcifications are limited. 1-5 But the presence of left atrial
thrombus (LAT) is generally considered a contraindication to this procedure because of
embolic risk, which may arise when catheters and wires are manipulated in the left
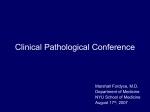
atrium.1-6 Figure 1 presents conceptual framework pathophysiology of LAT and its current
t
r
e
a
t
m
e
n
t
.
In developing countries, surgical treatment is not only far too expensive but also can not
meet the increasing demand. Patients have to wait for the surgery for approximately 9 - 15
months. While they were waiting, they must take an oral anticoagulant (OA) regularly. By
this, LAT of some patients were dissolved and thus can perform PTMC safely. Successful
resolution of LAT has been reported in our previous study. 7 However the duration of LAT
to disappear is considerably long, i.e., the mean duration of LAT resolution was 16
months. This means they are taking the risk of embolism during this period.
Another study conducted by some of our members showed that PTMC can be performed
safely if thrombus is confined in LA appendage.8 We belief that the improvement of
hemodynamic status may enhance the resolution of the thrombus. Thus the combination of
PTMC and OA is expected to shorten the duration of LAT resolution. A randomized
controlled trial is needed to demonstrate that.
Findings from this trial will contribute enormously to the developing world. Aside from
saving life and improving the quality of life of the patients, replacing surgery with PTMC
and OA combined could save a large amount of money per year. Unit cost of an opened
heart surgery is more than triple as much as that of PTMC, i.e., around 2500USD
c o m p a r e d
w i t h
7 0 0 U S D
r e s p e c t i v e l y .
2.2.Justification
Due to the evidence of a high prevalence of MS with LAT and the long waiting list for
mitral valve surgery leading to the risk of systemic embolism of the patients, an alternative
approach is urgently needed. Although there was an evidence that LAT can be dissolved
by OA only and then the PTMC can be performed safely and successfully, the patients are
still at risk of embolism unnecessarily due to the long course of OA. The positive findings
of a randomized controlled trial could strongly effect the current management of MS
patients with LAT locally and other developing countries.
2.3.Goals and objectives
The ultimate goal of this clinical trial is to reduce mortality and morbidity of MS patients
due to systemic embolism and improve their quality of life. At the end of this trial, it will
4
be established whether the combination PTMC and OA can be an alternative treatment for
MS patient having thrombus confined in LA appendage.
The main objective is to compare the rate of complete LAT resolution between treated by
OA only and the combination PTMC and OA at 4 and 6 months after treatment.
2.4.Hypothesis
The hypothesis to be tested in this trial is that, among MS patients, the rate of complete
LAT resolution at 4 and 6 months after treated by combination PTMC and OA is higher
than by OA alone.
Figure 1. Conceptual framework pathophysiology of LAT and current treatment
Dislodge
25%
Mitral stenosis
Systemic embolism
Thrombus in LA
20% among patients
having atrial
fibrillation
Dilated atrium
Atrial fibrillation
Sluggish flow
TREATMENT
Surgery is unavailable
Perform surgery if available
Recover normal hemodynamic status
Remove thrombus
Candidate of PTMC (-)
Oral anticoagulation
Wait for surgery
Candidate of PTMC (+)
Oral anticoagulation (INR = 2.5 to 3.5)
Perform PTMC after thrombus disappears
Change to surgery if hemodynamic is unstable
Conditions of performing PTMC:
Do not have clot in LA, or the clot is small, fixed in LA appendage
Absolute contraindications: thrombus attached to the atrial septum,
thrombus close to the mitral orifice or mobile thrombus
Regurgitation and valvular calcification are limited
5
3.Study design
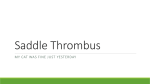
This will be a hospital-based, parallel, single blind, randomized controlled trial. Overview
of the trial is shown in Figure 2.
3.1.Interventions
3.1.1.Experimental arm: OA and PTMC
Patients will be treated by OA. PTMC will be performed as soon as possible by an
experienced operator while the LAT still exists. After the procedure, OA will still be
continued The dose will be adjusted based on the International Normalized Ratio (INR),
preferably, ranges from 2.5 to 3.5 or as high as the patients can tolerate. This range of INR
has been suggested by Songkwan et al (2001).
3.1.2.Control arm: OA only
All patients will be treated by oral anticoagulation with the adjusted dose based on INR
similar to what was described in the experimental arm. PTMC will be performed only after
the thrombus had been disappeared.
3.2.Methodology
3.2.1.Study population:
MS patients have thrombi in left atrial appendage and are candidates for PTMC.
Inclusion criteria:
MS patients with thrombus confined in LA appendage.
Do not have absolute contraindications of performing PTMC
Hemodynamic status is stable
Exclusion criteria:
Have contraindications of performing TEE.
Not satisfy the conditions of performing PTMC right after randomization.
Pregnant women.
3.2.2.Sample size:
From previous study (Silaruks, 1999), among 108 mitral stenosis patients there were 48
patients whose LAT area are smaller 2 cm2. By treating with OA only, the rate of complete
LAT resolution in this group is 68.75% (33 patients) after 6 months of follow-up. In this
trial, all patients will be performed TEE to measure the thrombus at 4 and 6 months after
the beginning of treatment. The combination of OA and PTMC has been expected to gain a
better result. The sample size will be calculated to detect the difference between two
thrombus disappearance rates after 4 months, at significant level of 95% and power of 80%
(two-sided test), using the approach of Lachin that was reviewed in the paper of Donner,
1984.9
n { Z 2 P ( 1 P ) Z PE ( 1 PE ) PC ( 1 PC ) } 2 / 2
Where:
PC = anticipated thrombus disappearance rate among control group patients
PE = anticipated thrombus disappearance rate among experimental group patients
P = (PC + PE)/2
6
= (PE – PC) = the difference in even rates regarded as clinically important to detect
n = the number of patients in per group
Table: Required sample size at different rate of thrombus disappearance
P-control
P-experimental
Alpha level
Power
Patients in one group
0.50
0.58
5%
80%
691.79
0.50
0.60
5%
80%
386.90
0.50
0.63
5%
80%
245.78
0.50
0.70
5%
80%
92.90
0.60
0.69
5%
80%
442.07
0.60
0.72
5%
80%
243.17
0.60
0.75
5%
80%
151.70
0.60
0.80
5%
80%
81.13
The sample size of 93 patients in each group will be chosen because of its feasibility. Such
sample size can detect 20% difference of thrombus disappearance rate between two
groups, at 95% significant level, with the power of 80%.
The anticipated drop out rate is about 10%. Thus, the sample size will be inflated as
following:
n = 93 / (1-0.1)2 = 114.8
Finally, the required number of patients for each group is 115
3.2.3.Random allocation technique:
After signing on the consent form, all eligible patients will be enrolled in the trial and then
randomized to receive the treatment of OA only or OA and PTMC. The method of block
randomization, with block size varies from 2 to 6, will be used to allocate treatments.
The allocation ratio is 1:1. The allocation sequence will be generated by computer, using
STATA software.
Based on the obtained schedule, the number of sealed envelopes, which are equal to the required blocks,
will be prepared and labeled. Each envelope contains the corresponding sealed allocation cards that will
allocate treatments to patients.
The instruction of allocation process is given in appendix 8.6.
The people, who prepare the randomized scheme, will not involve in the trial. The
allocation schedule will be concealed until the end of trial.
3.2.4.Blinding:
Because of the difference between two treatments, only the observers, who measure the
outcome (LAT size), will be blinded from the treatments.
7
The echocardiographers will assess the thrombus through videotape record, which does not
include patient’s name. They will be provided only the picture of left atrial appendage. The
status of mitral valve will be kept secret in order to ensure that the treatment can not be
guessed
3.2.5.Outcome and outcome measurement:
The main outcome is complete LAT resolution. It is measured by TEE. The TEE will be
performed at 4 and 6 months after the treatment.
3.2.6.Follow-up procedures:
Patients will be asked to return for clinical examination, monitoring INR every 3 months or
whenever they experience any discomfort. They will also return at 4 and 6 months to
perform TEE
Drop out could happen in the following manners:
Control arm
Died of complication of MS
Change to surgery because unstable hemodynamic status
Change to PTMC because of preference of patients
Experiment arm
Died of complication of MS
Change to surgery because unstable hemodynamic status
8
Figure 2. Design overview of the study
Mitral stenosis
TEE routinely: 25%MS have LAT
Ideally treated by surgery
LAT (-)
LAT (+)
The present study
Candidate of PTMC (-)
Candidate of PTMC (+)
OA
Wait for surgery
Recruitment eligible patients
Random allocation
OA as usual
PTMC when LAT disappears
New treatment: PTMC + OA
Expected duration is shorter
Measure clot size by TEE, after 4 months of treatment
Repeat TEE 2 months later, if clot still remained at 4 month-TEE
Primary outcome: complete resolution of LAT measured by TEE
9
3.3.Data analysis
There were two main parts of analysis – describing selected characteristics of the study
patients and analysis for answering the research questions. The first part, selected baseline
characteristics of the patients in each treatment were compared i.e. age, sex, underlying
diseases, etc. Comparability of the distribution of those selected characteristics based on
judgment rather than statistical significant tests. In this part, proportion was use for
summarizing categorical data. For continuos data, the statistics include mean, standard
deviation, minimum, maximum, and median.
For the second part, the analysis was based on the group in which the study patients were
randomized (intention-to-treat basis). The different rate of complete resolution between the
two arms of the trial and its 95% confidence interval will be calculated. This will be done
at 4 and 6 months after the treatment. Z-test will be used for testing if such differences are
different from zero. Multiple logistic regression will be used to control effects of some
baseline imbalance, if any.
The statistical analysis of this clinical trial will be performed based on intention to treat
principle. All hypothesis tests are two-tailed at significant level of 0.05. Statistical package
for all analysis is STATA.
Interim analysis:
The necessary duration for recruitment is estimated about 48 months. Interim analyses are
planned to be performed every 10 months, thus, the number of interim analyses will be 4.
The stopping boundaries are constructed based on the approach of O’Brien and Fleming as
the following:
Interim analysis number
1
2
3
4
Zc
4.084
2.888
2.358
2.042
p-value
0.00005
0.0039
0.0184
0.0412
Stopping rules:
Let the thrombus disappearance rates of control and experimental groups, at the first
interim analysis, are pc and pe, respectively. The test statistic of treatment effect is given by
Z = pe - pc / se (pe - pc)
The null hypothesis (pe = pc) will be rejected if Zis larger than the corresponding Zc, that
was specified above.
The above steps will be repeated for each subsequent interim analysis until the trial is
stopped or until it is finished.
Crossed stopping boundary is just the statistical guideline, not the rule, for terminating the
trial early. Making decision of early trial termination should consider other factors rather
than only the statistical guideline.
10
3.4.Ethical consideration
This trial protocol, which includes the study information and consent form (appendix 1),
must be accepted by the Ethical Committee before to start recruiting patients into the
study. The investigator must ensure that all patients will be received adequate verbal and
written information about the purpose, procedures, potential risk and benefit of the study.
The investigator must be responsible to obtain the appropriate consent form from the
patients before to recruit patients into the study.
4.Duration of the trial
A timeline is given in appendix 8.4 to indicate the estimated time that various stages of the
trial will take to complete.
It is anticipated that the whole trial need more than 4 years to complete if this time
schedule is adhered to. The recruitment will begin right after obtaining the approval of
Ethical Committee. Such long duration of recruitment is the limitation of this trial.
5.Expected outcome of the study
It will be established whether the LAT resolution rate is higher among group treated by
combination PTMC and OA, compared to those treated by OA only. If so, the combination
PTMC and OA will become the new approach for mitral stenosis patients having LAT.
The result of this study then will be published and applied not only to the developing
countries, but also to all over the world.
In this study, PTMC will be performed by only one high experience operator. To guarantee
the safety of the procedure if the new treatment has been established, the next necessary
steps is to train the cardiology operators in order to make them have ability to do PTMC
successfully in mitral stenosis patients having LAT.
6.Budget
7.References
1.
2.
3.
4.
5.
Participants NBR. Multicenter experience with balloon mitral commissurotomy.
NHLBI Balloon Valvuloplasty Registry Report on immediate and 30-day follow-up
results. The National Heart, Lung, and Blood Institute Balloon Valvuloplasty Registry
Participants. In: Circulation; 1992:448-61.
Inoue K, Owaki T, Nakamura T, Kitamura F, Miyamoto N. Clinical application of
transvenous mitral commissurotomy by a new balloon catheter. J Thorac Cardiovasc
Surg. 1984; 87:394-402.
Vahanian A, Michel PL, Cormier B, Vitoux B, Michel X, Slama M, Sarano LE,
Trabelsi S, Ben Ismail M, Acar J. Results of percutaneous mitral commissurotomy in
200 patients. Am J Cardiol. 1989; 63:847-52.
Nobuyoshi M, Hamasaki N, Kimura T, Nosaka H, Yokoi H, Yasumoto H, Horiuchi H,
Nakashima H, Shindo T, Mori T, et al. Indications, complications, and short-term
clinical outcome of percutaneous transvenous mitral commissurotomy. Circulation.
1989; 80:782-92.
Hung JS, Chern MS, Wu JJ, Fu M, Yeh KH, Wu YC, Cherng WJ, Chua S, Lee CB.
Short- and long-term results of catheter balloon percutaneous transvenous mitral
commissurotomy. Am J Cardiol. 1991; 67:854-62.
11
6.
7.
8.
9.
Kronzon I, Tunick PA, Glassman E, Slater J, Schwinger M, Freedberg RS.
Transesophageal echocardiography to detect atrial clots in candidates for percutaneous
transseptal mitral balloon valvuloplasty. J Am Coll Cardiol. 1990;16:1320-2.
Silaruks S. Resolution of left atrial thrombi with anticoagulant therapy in candidates
for percutaneous transvenous mitral commissurotomy. Unpublished. 1999.
Tansuphasawadikul S., Silaruk S. Transesophageal echocardiography during
percutaneous mitral commissurotomy in patients with left atrial thrombus. In press.
Donner A. Approaches to sample size estimation in the design of clinical trials - A
review. Statistics in medicine. 1984; 3:199-214.
8.Appendices
8.1.Consent form and statement
8.2.Data collection form
8.3.Dummy tables
8.4.Timeline for the trial
8.5.Algorithm for recording all patients during the trial period
8.6.Allocation instructions
12
Appendix 8.1
STUDY INFORMATION
We would like to know if you would be interested in taking part in an experimental
study being carried out to evaluate the new treatment of mitral stenosis patients in
Thailand. We provide the follow information in order to help you know more about this
study.
General description:
The symptomatic mitral stenosis patients will be treat currently by PTMC. PTMC is an
operation that widens the stenosed mitral valve orifice and make the heart function
recovered. Currently, if patients have clot in left atrium, they must take drug to make clot
disappear before being performed PTMC. The average duration to wait for clot
disappearance is 16 months. We do not know whether performing PTMC while the clot
still does exist will shorten the duration of clot disappearance. The purpose of this study is
to find this out.
The patients entering this study will be followed up 6 months with two times of
ultrasound checking, and then they will be changed to the usual follow-up schedule.
Treatment procedures:
The conventional treatment is taking drug and then performing PTMC after clot
disappears. The test treatment is performing PTMC first and then taking drug. The patients
will randomly receive either conventional or test treatment.
If you do not want to participate in this study, you will receive the conventional treatment.
Risks and discomforts:
PTMC is an operation, so the patient may suffer a complication at a certain level,
however, we confirm that it is very rare. We will let only the operator having high
experience performs PTMC for you. Please note that, even in case you do not participate in
this study, you will receive the conventional treatment for mitral stenosis that will also
include PTMC at finally.
After 4 and 6 months of treatment, you will be checked by ultrasound. We will put a
small probe in your esophagus to examine whether or not the clot has disappeared. It may
cause you a little discomfortable. This feeling will vanish right after the procedure.
Benefit:
The possible benefit, if you randomly receive the test treatment, is your heart function
may improve earlier compared to the conventional treatment. All medications and tests are
of charge. Only examinations and ultrasound checking at 6 months will be provided to you
free. The information obtained from this study will enable us to help other patients with
this disease.
Confidentiality:
Data, including personal information such as name and address, will be stored in a
computer. All personal information is confidential and available only to study personnel.
No report will be presented or published which reveal your identity.
13
Responsibilities of patient:
Participate in this study entirely voluntary. You have the right to withdraw from the
study at any time that will in no way affect to care or treatment you are receiving.
However, anyone who drops out after enrollment reduces the scientific value of the study.
Hence, you should not participate in if you are uncertain about the value of this study or if
you know that you can not fulfill the study requirement. Otherwise, you should be
compliant to your doctor after your participation.
If you are satisfied with the explanation of this study and do decide to participate in it,
p l e a s e
s i g n
t h e
a t t a c h e d
c o n s e n t
f o r m .
If you have any question, please feel free to ask your doctor or nurse.
14
Consent form
Study title
Effect of percutaneous transvenous mitral commissurotomy on resolution of left
atrial thrombus in mitral stenosis patients
Principal investigator:
Purpose of study: To evaluate whether the combination percutaneous transvenous mitral
commissurotomy and oral anticoagulation can be an alternative
treatment of surgery for mitral stenosis patient having left atrial
thrombus.
Consent statement
I have read the foregoing information, or it has been read to me. I have had the opportunity
to ask any question and I have satisfied with all answers. I consent to participate in this
study to evaluate the effect of percutaneous transvenous mitral commissurotomy on
resolution of left atrial thrombus in mitral stenosis patients, as outlined above.
I understand that I am free to withdraw my consent at any time without, in any way,
affecting my current and future care and without losing any benefits.
Signature:………………………………………..
Date: ___/___/___
I, Dr. ____________________, the principle investigator, have explained the purpose,
procedure, potential risk and benefit of this study to __________________
Signature:……………………………………..
Date: ___/___/___
15
Appendix 8.2
DATA COLLECTION FORM
ID:
Effect of percutaneous transvenous mitral commissurotomy on resolution of left
atrial thrombus in mitral stenosis patients
2.7.Diabetus mellitus
1.Yes 2.No
Day/ month/ year
Patient number
2.8.Hypertension
1.Yes 2.No
Name:……………………………………………
Address:…………………………………..……
2.9.Smoking
1.Yes 2.No
1.Status
1.1 Age (years)
2.10.Hemoptysis
1.Yes 2.No
1.2.Sex
1.Male
2.Female
2.11.Dyspnea on exertion
1.Yes 2.No
1.3.Occupation
1.Farmer
3.Commercial
2.Officer
4.Employment
2.12.Admission for CHF
1.Yes 2.No
3.NYHA class
(class I-IV)
2.History
2.1.Duration (months)
(from first symptom to visiting doctor)
2.2.Congestive heart failure
2.2.1.Paroxysmal nocturnal dyspnea
1.Yes 2.No
4.Prothrombin time
4.1.Baseline, INR
4.2.At 3m, INR
2.2.2.Orthopnea
1.Yes 2.No
4.3.At 6m, INR
2.3.Syncope
1.Yes 2.No
2.4.Stroke
1.Yes 2.No
5.EKG
5.1.Atrial fibrillation
1.Yes 2.No
5.2.LA enlarge
1.Yes 2.No
2.5.Peripheral embolism
1.Yes 2.No
5.3.RAE
1.Yes 2.No
2.6.Palpitation
1.Yes 2.No
5.4.RVH
1.Yes 2.No
16
6.ECHO
6.1.MVA (2D)
(cm2)
6.2.Pressure-half time
6.10.LA clot after 6 months
6.10.1.LA clot size at 6m
Width (mm)
Length (mm)
Area (mm2)
6.3.Mitral valve score
(4-16)
6.10.3.Number of LA clot at 6m
(1-5)
6.4.LA diameter
(mm)
6.5.Mitral regurgitation
(grade 1-4)
6.6.Triscupid regurgitation
(m/sec)
6.7.LASEC
(grade 1-4)
6.8.LA clot
6.8.1.LA clot size
Width (mm)
Length (mm)
Area (mm2)
6.8.2.Mobility of clot
1.Mobile 2.Linear 3.Fixed
6.8.3.Number of LA clot
(1-5)
6.9.LA clot after 4 months
6.9.1.LA clot size at 4m
Width (mm)
Length (mm)
Area (mm2)
6.9.2.Number of LA clot at 4m
(1-5)
7.Follow up
7.1.Complication
Stroke
1.Yes 2.No
Peripheral embolism
1.Yes 2.No
Infective endocarditis
1.Yes 2.No
7.2.NYHA class after 6m
(class I-IV)
8.Drop out
1.Yes 2.No
If yes, specify:……………..
17
Appendix 8.3
Dummy tables
Table 1. Characteristics of patients at trial entry
Values refer to number (%) unless indicated otherwise
PTMC and OA
(n= )
Characteristics
OA only
(n= )
Mean age (SD), years
Male : Female
Smoking
Atrial fibrillation
NYHA
Class II
Class III-IV
Mean INR (SD)
LA thrombus
Mean width (SD), cm
Mean length (SD), cm
Mean area (SD), cm2
Mean LA diameter (SD), cm
Mean mitral valve score (SD)
Mitral regurgitation
Grade II
Grade III-IV
Mean MVA (SD), cm2
LASEC on TEE
Grade 2
Grade 3
Grade 4
Table 2. The different rate of complete LAT resolution after 4 and 6 months of treatment
of NYHA functional class and complication between two group
PTMC and OA
(n= ) %
Complete LAT resolution
After 4 months
After 6 months
NYHA after 6 months
Class I
Class II
Class III-IV
Complication
NNTs (95%CI):
OA only
(n= ) %
Different rate
(95%CI)
p-value
18
Table 3. Multivariate logistic regression results: treatment effects on complete LAT
resolution adjusted for potential confounding factors
Treatment
PTMC and OA
OA only
LA area (1cm2 increase)
LASEC on TEE
Grade 1
Grade 2
Grade 3
Grade 4
INR after 3 months
Crude OR
(95%CI)
Adjusted OR
(95%CI)
1
1
1
1
p-value
19
Timeline for the trial
Appendix 8.4
2000
Jan
Feb
2001
Mar
Apr
Protocol development
Ethics application
Recruitment
Interim analysis
Analysis
Reporting
The necessary duration for recruitment is estimated about 48 months.
Feb
Dec
2001
2003
Sep
Jun
2004
Mar
Apr
May
Jun
20
Appendix 8.5. Algorithm for recording all patients during the trial period
Total number of eligible MS patients
(n = …)
Randomization
(n = …)
Not randomized
(n = …)
Reasons
Refused consent
Other, specify
………………………
……………
Received control treatment
as allocated
Did not received control treatment
as allocated
Received test treatment
as allocated
Did not received test treatment
as allocated
Followed up after 4 months
Followed up after 6 months
Followed up after 4 months
Followed up after 6 months
Withdraw
Died of MS complication
Change to surgery
Change to PTMC
Completed trial
(n = …)
Withdraw
Died of MS complication
Change to surgery
Other
Completed trial
(n = …)
n
21
Appendix 8.6
Allocation instructions
Effect of percutaneous transvenous mitral commissurotomy
on resolution of left atrial thrombus
Description of allocation scheme:
The scheme was prepared for allocating a total of 230 patients. These were randomly
divided into 61 blocks with varied block size. One sealed envelope refers to one block. The
block size also randomly varies from 2 to 6, i.e., there are 2, 4 or 6 allocation cards within
each sealed envelope.
Each allocation card was sealed by 3 stickers. In the last sentence of each allocation
card, there is one number corresponding with the sequence of patients within block. Name of
patient and hospital number must be recorded before breaking the seals. There is the code of
treatment inside each allocation card.
How to allocate patients?
When the first eligible patient entry the trial, Block 1 will be opened. Then the
Allocation card within each block will be broken. This has to be done in sequence as specified
in the Allocation number. By this process, the code of treatment will be identified as either
“PTMC and OA” or “OA only”.
The next block then will be opened in sequence as specified in the Block number.
Role of people involving in allocation process:
There should be one nurse in charge in management the allocation process. Once a
patient was enrolled and the doctor asked for the allocation code, she will be the one who
opens the envelope. First, she has to choose the allocation card in the sequence, then
records the patient’s name and the hospital number before breaking the allocation card,
and finally reads the type of treatment to the doctor. She is also the one who keeps all
allocation cards for further reference.
The doctor will know what type of treatment to be provided to a certain patient only after
asking the nurse who is in charge in the allocation process.
The echocardiographers must not aware of what type of treatment was given to a patient
whose image was being measured for the outcome.
22
Sequence of treatment allocating
The first column: code of patients
The second column: code of blocks
The third column: size of blocks
The fourth column: sequence of patient within block
The fifth column: treatments
NOTE: the following sequence is just an example to demonstrate how the sequence of
treatment allocating is. It is different with the true sequence of the clinical trial.
1
1
2
1
PTMC+OA
139
37
6
1
PTMC+OA
2
1
2
2
OA
140
37
6
2
OA
3
2
4
1
OA
141
37
6
3
PTMC+OA
4
2
4
2
PTMC+OA
142
37
6
4
OA
5
2
4
3
PTMC+OA
143
37
6
5
PTMC+OA
6
2
4
4
OA
144
37
6
6
OA
7
3
4
1
OA
145
38
2
1
PTMC+OA
8
3
4
2
OA
146
38
2
2
OA
9
3
4
3
PTMC+OA
147
39
4
1
OA
10
3
4
4
PTMC+OA
148
39
4
2
OA
11
4
4
1
PTMC+OA
149
39
4
3
PTMC+OA
12
4
4
2
PTMC+OA
150
39
4
4
PTMC+OA
13
4
4
3
OA
151
40
2
1
OA
14
4
4
4
OA
152
40
2
2
PTMC+OA
15
5
4
1
PTMC+OA
153
41
6
1
OA
16
5
4
2
PTMC+OA
154
41
6
2
PTMC+OA
17
5
4
3
OA
155
41
6
3
PTMC+OA
18
5
4
4
OA
156
41
6
4
OA
19
6
2
1
OA
157
41
6
5
OA
20
6
2
2
PTMC+OA
158
41
6
6
PTMC+OA
21
7
4
1
OA
159
42
2
1
OA
22
7
4
2
OA
160
42
2
2
PTMC+OA
23
7
4
3
PTMC+OA
161
43
4
1
OA
24
7
4
4
PTMC+OA
162
43
4
2
OA
25
8
2
1
OA
163
43
4
3
PTMC+OA
26
8
2
2
PTMC+OA
164
43
4
4
PTMC+OA
27
9
4
1
PTMC+OA
165
44
2
1
PTMC+OA
28
9
4
2
PTMC+OA
166
44
2
2
OA
29
9
4
3
OA
30
9
4
4
OA