Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
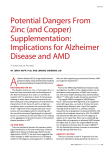
Volume 1, Issue 6 2014 A Learning Resource for Optometrists from the School of Optometry & Vision Science, University of Waterloo, and the School of Optometry, University of Montreal Age-Related Macular Degeneration: From Diagnosis to Treatment By Julie Brûlé, OD, MSc, FAAO, Julie-Andrée Marinier, OD, MSc, and Judith Renaud, OD, PhD Age-related macular degeneration (AMD) is the most common cause of legal blindness in adults living in developed countries. It is associated with significant functional, quality of life, and psychological implications. While the atrophic (“dry”) form is more common, exudative or neovascular (“wet”) AMD is responsible for up to 90% of the cases of significant vision loss related to AMD. This issue of Optometry Rounds outlines the clinical evaluation and management for the patient with AMD, including the latest data on nutritional supplements and pharmacotherapy. Age-related macular degeneration (AMD) is the leading cause of legal blindness (corrected visual acuity [VA] ≤6/60 or greatest diameter of the visual field ≤20° in each eye) among adults in developed countries.1 In Canada, an estimated 1 million adults aged ≥40 years have early AMD and a further 250 000 have more advanced forms.2 These amounts are projected to double by 2030.3 AMD is associated with significant negative functional and psychosocial effects. Social roles and daily activities, particularly those requiring central vision, may be significantly affected.4-7 For example, AMD patients may need to prematurely stop working or modifying their work tasks. They also often have difficulty recognizing faces and facial expressions, which hinders social interactions.8 Many leisure activities can be restricted.6,7 To adapt to these changes, the person will have several significant adjustments to make and will need assistance, technological as well as human.6,9 The traumatic experience of visual loss associated with AMD frequently has significant emotional and psychological consequences. Quality of life in individuals with AMD is comparable to that of those suffering from serious systemic diseases such as cancer, ischemic heart disease, and stroke.10 Fears of going blind and loss of independence often lead to anxiety and depression.11,12 Older individuals with visual disabilities are at particularly high risk for depression; the prevalence of depression in this population is 7%–25%,13,14 and 25%–45% experience depressive symptoms.15-17 Given the increased risk of suicide in the depressed elderly, this mental health problem cannot be overlooked. Clinical Classification AMD is divided into 2 types: atrophic (“dry”) and exudative or neovascular (“wet”). The dry form is the most common, affecting approximately 85% of AMD patients. 18 In its early stages, dry AMD is characterized by the presence of fatty deposits under the retinal pigmented epithelium (RPE), called drusen, as well as regions of irregular RPE pigment (Figures 1A, 1B). Drusen may coalesce and progress towards a detachment of the RPE and, eventually, form atrophic regions. This atrophy can be focal or extensive; the latter, called geographic atrophy, is the advanced form of dry AMD and may cause significant visual loss (Figure 1C).18,19 Some cases of dry AMD may progress to the wet form. Exudative (“wet”) AMD is characterized by the development of neovascular choroidal vessels. These new vessels can leak and cause bleeding or accumulation of intraretinal fluid. Exudative AMD often presents with retinal fibrosis (Figure 1D).18,19 Despite its markedly lower occurrence than the dry form, wet AMD accounts for up to 90% of cases of significant AMD-related vision loss.20-22 Paul Murphy, FCOptom, PhD, FAAO Professor and Director Thomas F. Freddo, OD, PhD, FAAO Professor and Co-Editor, Optometry Rounds Contributing Faculty Authors: Sarah MacIver, OD, FAAO Clinical Lecturer C. Lisa Prokopich, OD, MSc Clinical Lecturer Michelle Steenbakkers, OD, FAAO Clinical Lecturer École d’Optométrie School Administration: Christian Casanova, PhD Director and Professor Neurophysiology and Imaging Danielle de Guise, OD, MSc Associate Director of Cycle 1 Studies Binocular Vision and Orthoptics Jocelyn Faubert, PhD, FAAO Associate Director of Research and Advanced Studies Professor, Psychophysiology and Visual Perception Jacques Gresset, OD, PhD, FAAO Secretary and Professor Epidemiology and Low Vision Editorial Committee: Jean-François Bouchard, BPharm, PhD Associate Professor, Neuropharmacology Pierre Forcier, OD, MSc Associate Professor, Ocular Health Langis Michaud, OD, MSc, FAAO (Dipl.) Associate Professor, Contact Lenses Co-Editor, Optometry Rounds Judith Renaud, OD, PhD Assistant Professor, Low Vision Risk Factors University of Waterloo School of Optometry & Vision Science 200 University Avenue West, Waterloo, ON N2L 3G1 Although the pathological processes leading to the onset and progression of AMD have yet to be fully understood, several risk factors for the disease have been identified. Université de Montréal École d’Optométrie 3744 Jean-Brillant, Montreal, QC H3T 1P1 Available online at www.optometryrounds.ca The editorial content of Optometry Rounds is determined solely by the School of Optometry & Vision Science, University of Waterloo, and the School of Optometry, University of Montreal. Figures 1A-D: Age-Related Eye Disease Study (AREDS) categories for age-related macular degeneration (AMD) 1A. Category 2: intermediate confluent drusen and abnormalities in the retinal pigmented epithelium (RPE) Non-modifiable risk factors Age. Population-based studies indicate that the incidence, prevalence, and severity of AMD increase significantly with age.20-26 Family history. The presence of AMD within the family is associated with an increased risk of its development.24,27 This association is consistent with the increasingly important role of several predisposing genetic factors.19 Ethnicity has long been identified as a major risk factor for AMD. Studies have suggested that Caucasians are more affected by AMD than other races.20,28,29 Despite this fact, a recent meta-analysis attributed a low level of risk to this factor.24 Sex. Women may be at a slightly greater risk than men for developing AMD;20,25 however, this factor remains controversial.21,24 Systemic conditions. AMD appears to be associated with a positive history of cardiovascular disease, hypertension, or diabetes.24,29,30 Ocular risk factors. Patients with lighter iris pigmentation are at a greater risk of developing AMD,24,31 as are those who are hyperopic.20 A history of cataract surgery is also a risk factor for the development of advanced AMD, 24,32 although a randomized, controlled clinical trial did not report any effect of cataract surgery on the course of AMD.33 Modifiable risk factors 1B. Category 3: intermediate and large drusen that coalesce with RPE abnormalities 1C. Category 4: geographic atrophy involving the fovea Smoking (current and ex-smokers) is the most important modifiable risk factor for AMD. It is strongly associated with a markedly increased risk of developing AMD and of evolving towards the more advanced stages.20,21,24,29,34 Alcohol. Moderate daily alcohol consumption (2 standard drinks per day) has been linked to an elevated risk of AMD,35 and high alcohol consumption (>3 drinks per day) is associated with a significantly increased risk of early AMD development.36 Medication. Regular and long-term ingestion of acetylsalicylic acid may raise the risk of developing neovascular AMD, depending on the dose;37 however, it should be noted that the standard dose prescribed for the prevention of cardiovascular disease (81 mg) was not studied. Obesity. Although some data support an association between obesity and AMD,24,38,39 the effect of weight loss in the prevention or slowing down of AMD remains to be determined.40 Sun exposure. The role of sun exposure in the development of AMD is a longstanding controversy.20,22,31,41,42 A recent meta-analysis43 reveals that individuals who had greater exposure to the sun are at an increased risk of developing AMD. The optometric and ophthalmological communities thus consider exposure to sun as a risk factor, especially since it is easily modifiable.44 Clinical Evaluation 1D. Category 4: exudative AMD with retinal fibrosis 2 Clinical examination of patients living with AMD includes the assessment of numerous visual functions as well as a mandatory fundus examination with pupillary dilation. Disease staging (Figure 2) is an essential element for decision making regarding management, including timing of optometric follow-up and determination of whether referral to an ophthalmologist and/or low vision services is indicated. Figure 2: Clinical follow-up of AMD Category 1* Category 2* Category 3* • Management of risk factors • Management of risk factors • Amsler grid (home use) • Follow-up: 1 year • Management of risk factors • Amsler grid (home use) • Follow-up: 6-12 months • Amsler grid (home use) • Nutritional supplements • Follow-up: 6-12 months • Referral as needed to an ophthalmologist or vision rehabilitation Category 4* Dry AMD: geographic atrophy • Management of risk factors • Nutritional supplements • Referral to an ophthalmologist • Vision rehabilitation • Follow-up: 6 months Wet (exudative) AMD • Referral to an ophthalmologist • Vision rehabilitation • Follow-up: 6 months * According to AREDS Management Inform patients about the importance of regular examinations, even in the absence of symptoms, and instruct them to seek prompt consultation with an optometrist or ophthalmologist following the emergence of any new visual symptoms. Patient history should include questions about the known risk factors for AMD, recent visual changes, or symptoms relating to the onset or progression of AMD, such as meta- morphopsia. It is also important to ask patients about the functional impact of AMD on their daily life (Table 1). Measurement of VA is essential to assess the progression of AMD and in order to perform functional vision follow-up. When there is a significant decrease in vision (VA <6/18), lowvision charts are more appropriate. These include the Feinbloom and Early Treatment Diabetic Retinopathy Study Table 1: Examples of activities and roles affected by AMD Nutrition Meal preparation Operating food-preparation appliances (eg, stove, microwave) Reading restaurant menus Personal care Medication identification and dosing Choice of clothing Hair styling, makeup, and shaving Communication Reading and writing Use of computer, telephone, and television Housing Housekeeping Operating appliances (eg, washer, dryer, heating system) Mobility Safe ambulation inside and outside the home Crossing streets Loss of driver’s license (consult provincial/territory laws) Use of public transit Community life Use of public services (bank, post office, library) and shops Responsibilities Payment of accounts Distinguishing money (bills and coins) Use of credit and bank cards Interpersonal relationships Recognition of faces and facial expressions Work Commuting to work Performing job-related responsibilities Leisure Crafts and hobbies (eg, do-it-yourself projects, knitting) Games (eg, bridge, bingo) and sports activities Attending artistic or cultural events (eg, theatre) 3 (ETDRS) charts for distance vision. Options for near vision include the reduced ETDRS and Lighthouse (single letter) charts as well as reading charts such as the Minnesota Reading Test (MNRead Card) or Colenbrander.45 During VA measurement, it is important to verify the presence of binocular summation (improvement) or inhibition (deterioration), especially while measuring reading VA.46 Finally, the evaluation of contrast sensitivity, using specific scales such as PelliRobson for distance vision or the Mars for near vision, can help to understand the patient’s functional complaints.47,48 Considering the modifications of the central visual field, refraction should be tested with trial frames to allow eccentric fixation. 49 In a patient receiving anti-vascular endothelial growth factor (anti-VEGF) injections, it is possible to observe a refraction variation. This underlines the need to verify the prescription should a change in VA occur. Evaluation of the peripheral and central visual fields will determine whether metamorphopsia or a scotoma (relative or absolute) are present. An automated Octopus or Goldmann perimeter with a dome is typically used as a kinetic visual field to measure the functional visual field. The Amsler grid helps to verify the presence of metamorphopsia or central scotomas. Use of reverse polarity, with white lines on a black background with a marked X, is recommended. It should be noted that if the Amsler grid is used by the patient at home (for monitoring purposes), the optometrist cannot rely solely on these results to determine the presence or absence of scotomas. Central visual field testing, such as a 10-2 central field (Humphrey or Octopus), should be included in the evaluation, assuming there is sufficient central vision to maintain fixation.50 The complete eye examination performed under dilation with fundus biomicroscopy and indirect binocular ophthalmoscopy will help to properly establish the stage of AMD (Table 2). Fundus photography will document the progression of AMD and will be useful for interdisciplinary references. Additional assessments, such as optical coherence tomography (OCT) and microperimetry, are used with increasing frequency. OCT identifies, among other things, the presence of neovascularization, subretinal fluid, and retinal tears, helping to specify the stage of AMD (Figures 3A,B). 51 A recent study52 concluded that the best predictor of VA improvement following ranibizumab (anti-VEGF) injections was the pretreatment integrity of the outer retina on OCT. In addition, Table 2: AREDS categories Category Signs 1 None or few small drusen 2 At least 1 of the following: • several small drusen (≤63 µm) • some intermediate drusen (62-124 µm) • RPE anomalies 3 At least 1 of the following: • several intermediate drusen • 1 or more large drusen (≥125 µm)* • geographic atrophy not involving the fovea 4 Geographic atrophy involving the fovea or any sign of exudative AMD and visual loss * 125 µm represents approximately the diameter of the retinal vein near the optic nerve 4 Figures 3A,B: Retinal optical coherence tomography sections 3A. Moderate dry AMD 3B. Wet AMD with intraretinal fluid and neovascularization outer retinal thickness and OCT-determined integrity of the RPE have been shown to be good predictors of AMD progression and central visual field narrowing, as measured by microperimetry. 53 From a functional point of view, vision rehabilitation experts study eccentric fixation with microperimetry and scanning laser ophthalmoscopy (SLO) combined with OCT. Recent studies show that a comprehensive assessment of functional vision allows effective and positive vision rehabilitation for patients receiving anti-VEGF injections.53 New retinal imaging techniques (with the autofluorescence function) have reduced the use of fluorescein angiography in AMD treatment. However, a consensus of Canadian ophthalmologists recently reported that angiography remains important for the clinical monitoring of AMD, in particular to determine the size of the lesion to be treated and to detect geographic atrophy or early choroidal neovascularization.54 Management of AMD Patients Managing risk/aggravating factors The management of risk factors and aggravating factors is essential in all patients with AMD and at all stages of the disease. Optometrists should educate the patient about modifiable risk/aggravating factors related to lifestyle and recommend changes. The effects of smoking, the most important modifiable risk factor, are reversible: the risk begins to decrease as soon as the patient stops smoking.55 It is therefore important to question patients regarding their smoking status and to encourage patients who smoke to begin their cessation attempt and even refer them to specific resources like the panCanadian telephone helpline (iQuitnow 1-866-527-7383). It is also important to advise patients with respect to adequate sun protection, as well as to raise awareness regarding the importance of maintaining a healthy weight and limiting alcohol consumption. Nutritional supplements The prescription of nutritional supplements can be useful in some patients with AMD. The Age-Related Eye Disease Study (AREDS) showed that a combination of high doses of antioxidants and minerals (vitamins C and E, beta carotene, and zinc) could delay the progression of dry AMD in patients with moderate or advanced stages of the disease (ie, AREDS category 3–4; Table 3).56 Patients who smoke or have recently quit should receive formulas without beta-carotene; supplements containing high doses of beta-carotene have been associated with a higher risk of lung cancer in these populations.57 Despite the suggested benefit in some studies of dietary supplementation with antioxidants, minerals, and omega-3 in the delay or prevention of AMD onset,35,58,59 there is insufficient evidence to justify their recommendation to patients with no disease evidence of AMD or only mild disease.35,56,60 Various studies suggest a protective effect of carotenoids (lutein and zeaxanthin) throughout the progression of AMD towards the advanced stages. AREDS-261 explored this question, in addition to the effect of omega-3 alone or in combination with carotenoids on a randomized, controlled sample. There was no statistically significant effect of adding omega-3 or carotenoids to the original AREDS formula, whether on AMD progression to advanced stages or on improvement of VA. particular challenges faced with their social roles and activities is of paramount importance (Table 1). It is important to maximize their independence and safety in their daily life. It is also important to discuss the patient’s expectations and to ensure that they are realistic. The patient’s goals should guide the examination. It is essential to recognize that patients’ psychological or cognitive state may create a dichotomy between their daily functioning and objective measures. For example, a depressive state is associated with a reduced perception of functional capacity, sometimes resulting in an inequality between measured visual functions and functioning in everyday life.62 Furthermore, studies have identified an association between the signs of AMD and cognitive deficits.63,64 Conversely, cognitive problems may affect visual skills.65 The optometrist must be vigilant to these potential health problems and refer patients to their family physicians or other healthcare professionals (geriatricians, neuropsychologists, psychiatrists, psychologists) for appropriate treatment. It is also important to discuss potential functional and psychosocial issues with the patient’s relatives. Consideration of functional and psychosocial impacts Patient resources The functional impacts of AMD sometimes require multiple adjustments to ensure that patients can perform their daily activities and social roles: adaptation to their environments, compensatory strategies, use of assistive devices (optic and nonoptic; Table 4), and human assistance. In assessing the needs of the individual, identification of the A wide array of interventions exists to help AMD patients in their adaptation process. In Canada, many resources are available, varying from timely services to national programs.66 Specialized readaptation services exist through hospitals, optometric/ophthalmological clinics, provincial government centres, or organizations such as the Canadian National Institute for the Blind (www.cnib.ca). Some provinces reimburse specialized examinations for low vision and offer loans or grants for technical aids. Several community organizations and associations provide both general assistance to the elderly and more specific services for those with visual impairment, including AMD; eg, disease information, support groups, psychological support, cleaning services, and home meals. Optometrists should be aware of the different resources in their community to better inform their patients. In addition, the federal and some provincial governments provide a tax credit for people with legal blindness. For the federal tax statement, this credit can be claimed under the Disability Tax Credit Certificate (form T2201, http://www. cra-arc.gc.ca/E/pbg/tf/t2201); optometrists are authorized to fill out this form. Carotenoids Table 3: AREDS-recommended dose of nutritional supplements to delay the progression of AMD according to AREDS Ingredients Original AREDS Recommended formula AREDS-2* formula Beta-carotene (mg) 15 0 Omega-3 (ester/ triglycerides; mg) 0 0 Vitamin C (mg) 500 500 Vitamin E (UI) 400 400 Copper (mg) 2 2 80 (O) 80 (O) Lutein (mg) 0 10 Zeaxanthin (mg) 0 2 Moderate AMD: prescribe the formula without betacarotene (formula "S") for smokers and ex-smokers Moderate AMD Zinc (oxide or gluconate; mg) When should they be recommended? (clinical target) Medical Treatments * The AREDS-2 formula is characterized by the absence of beta-carotene. According to the results of the study, the combination of lutein and zeaxanthin replaces beta-carotene while reducing the risk of side effects in smokers, ex-smokers or those who have been exposed to second-hand smoke. Since the advent of anti-VEGF agents for the treatment of wet AMD, such as bevacizumab and ranibizumab, numerous clinical trials have attempted to specify the efficacy and dosage of these therapeutic agents. Ranibizumab, a humanized monoclonal antibody fragment that binds with high affinity to all types of VEGF antigen isoforms (VEGF-A) and their associated degenerative products, is approved by Health Canada for the treatment of exudative AMD, as well as for the treatment of visual impairment due to diabetic macular edema and macular edema secondary to retinal vein occlusion. 67 The MARINA 68 and ANCHOR69,70 studies have shown significantly greater efficacy of ranibizumab compared to sham injection and verteporfin 5 Table 4: Activities, adaptation, and technical aids Activities Target VA according to activity Suggested adaptation and technical aids Reading prices in stores and medication names, using postal and bank services For decoding, should see 1M (use near VA cards such as reduced ETDRS or Lighthouse charts) llluminated hand-held magnifier, high-add eyeglasses (>4.00D), microscopic eyeglasses Reading, managing finances, and mail For reading, should see 0.8M (use reading charts such as MNRead or Colenbrander) Adjust lighting, large-print materials, high-add eyeglasses (>4.00D), microscopic eyeglasses, illuminated stand magnifier, electro-optical magnifying device, closed-circuit television (CCTV) Reading street names, addresses, and notice boards At distance, target VA of 6/12 Terrestrial telescopes, binoculars Use of electronics, appliances, remote controls, and telephone Device labeling with contrasting or textured tags, large-print devices VA = visual acuity; ETDRS = Early Treatment Diabetic Retinopathy Study therapy, respectively, over a period of 2 years. Improvements in the best corrected VA were significantly higher than results obtained with previous therapies used for AMD treatment. For the first time, a treatment managed to maintain and even significantly improve the VA in the treatment group in comparison with the control group. In addition to greater visual function, monthly injections of ranibizumab also resulted in an improvement of the retina’s anatomical architecture as observed with angiography and OCT over a period of 24 months.71,72 A recent consensus among Canadian ophthalmologists recommended that an initial monthly intravitreal injection dose for the first 3 months be continued with monthly injections until the neovascularization has stabilized.54 Bevacizumab, also administered by monthly intravitreal injection, was studied for the treatment of exudative AMD. This human monoclonal antibody binds and blocks the action of all vascularization isotypes, similar to those covered by ranibizumab. Several retrospective and prospective studies have shown its efficacy for the treatment of exudative AMD, with a low risk of complications.73-76 It is important to note, however, that bevacizumab is not approved by Health Canada for ocular use.77 In light of persistent clinical questions regarding whether ranibizumab or bevacizumab is more effective for the treatment of exudative AMD, the National Eye Institute of the United States (US) from the National Institutes of Health (NIH) organized the multicentre, prospective, randomized, controlled clinical Comparison of Age-related Macular Degeneration Treatments Trials (CATT).78 In 2011, the CATT group published that bevacizumab was not inferior to ranibizumab for the treatment of wet AMD. As well, the rates of adverse events such as bacterial endophthalmitis, increased intraocular pressure, uveitis, and retinal detachment were similar between the 2 agents in all of the groups. However, patients receiving bevacizumab experienced significantly more serious systemic adverse events and hospitalizations (risk ratio 1.29; 95% confidence interval 1.01 to 1.66). Finally, on the same monthly injection basis over the period of 1 year, bevacizumab was much less costly than ranibizumab. These results were supported by the 2-year CATT results.79 It is ultimately up to the ophthalmologist to weigh the clinical risks versus the benefits for each patient treated. 6 The most recent treatment for exudative AMD is intravitreal aflibercept, which recently received approval from Health Canada. 80 In 2012, the VIEW 1 and VIEW 2 81 randomized clinical trials showed that aflibercept, when administered monthly or every 2 months following the first 3 initial monthly injections, proved to be as effective and safe as ranibizumab for the treatment of exudative AMD. The administration of aflibercept every 2 months could reduce the risks associated with monthly intravitreal injections. Finally, collaboration between the optometrist and ophthalmologist is essential for preservation of vision for patients receiving intravitreal treatment. Proper disease staging and appropriate treatment will result in stabilization or even improvement of the patient’s vision. Emerging therapies New therapies are emerging for the treatment of AMD, particularly gene therapy and stem cell (RPE) transplantation therapy. Knowing the genotype of the patient with AMD will eventually make it possible to intervene and treat earlier in the disease, especially in the first stage of atrophic AMD.82 Stem cell transplantation therapy involves the replacement of damaged retinal cells with embryonic stem cells.83 Conclusion Optometrists, as primary eye care professionals, regularly encounter individuals with AMD in their practice. AMD is classified under 2 forms: atrophic (dry) and exudative (wet). The evolution and the complications associated with these 2 forms differ, requiring each a specific follow-up. Fundus examination performed under pupil dilation as well as other complementary tests, such as OCT, will help the optometrist to determine the stage of AMD. Given that there are numerous risk factors and treatment options for this disease, the optometrist must be familiar with them in order to educate and counsel patients. Finally, AMD can impact on both functional and psychosocial levels. Vision rehabil itation services can minimize these impacts on patients’ daily activities and social roles. Actively collaborating with AMD patients, the optometrist plays a key role in oculo visual health. Dr. Brûlé is an Assistant Professor at the School of Optometry, University of Montreal. Dr. Marinier is an Assistant Professor at the School of Optometry, University of Montreal, and an Optometrist at the Institut Nazareth et Louis-Braille. Dr. Renaud is an Assistant Professor at the School of Optometry, University of Montreal, and an Optometrist at the Institut Nazareth et Louis-Braille. These authors contributed equally to this article. References 1. Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82(11):844-851. 2. Burhmann R, Hodge W, Beardmore J, et al. Foundations for a Canadian Vision Health Strategy. Toronto (ON). Prepared for the National Coalition for Vision Health, January 2007. 3. Buhrmann R, Hodge WG, Gold D. Forecasting the vision loss epidemic in Canada: current and projected estimates of age-related eye disease. Report submitted to the National Coalition for Vision Health. 2006 September 23, 2006. 4. Hassell JB, Lamoureux EL, Keeffe JE. Impact of age related macular degeneration on quality of life. Br J Ophthalmol. 2006;90(5):593-596. 5. Lamoureux EL, Pallant JF, Pesudovs K, et al. Assessing participation in daily living and the effectiveness of rehabiliation in age related macular degeneration patients using the impact of vision impairment scale. Ophthalmic Epidemiol. 2008;15(2):105-113. 6. Desrosiers J, Wanet-Defalque M-C, Temisjian K, et al. Participation in daily activities and social roles of older adults with visual impairment. Disabil Rehabil. 2009;31(15):1227-1234. 7. Alma MA, van der Mei SF, Melis-Dankers BJM, van Tilburg TG, Groothoff JW, Suurmeijer TPBM. Participation of the elderly after vision loss. Disabil Rehabil. 2011;33(1):63-72. 8. Wong EYH, Guymer RH, Hassell JB, Keeffe JE. The experience of agerelated macular degeneration. J Vis Impair Blind. 2004;98(10):1-30. 9. Good GA, LaGrow S, Alpass F. An age-cohort study of older adults with and without visual impairments: activity, independence, and life satisfaction. J Vis Impair Blind. 2008;102(9):517-527. 10. Yuzawa M, Fujita K, Tanaka E, Wang EC. Assessing quality of life in the treatment of patients with age-related macular degeneration: clinical research findings and recommendations for clinical practice. Clin Ophthalmol. 2013;7:1325-32. 11. Casten R, Rovner B. Depression in age-related macular degeneration. J Vis Impair Blind. 2008;102(10):591-599. 12. Berman K, Brodaty H. Psychosocial effects of age-related macular degeneration. Int Psychogeriatr. 2006;18(3):415-428. 13. Brody BL, Gamst AC, Williams RA, et al. Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology. 2001;108(10):1893-1900. 14. Horowitz A, Reinhardt JP, Kennedy GJ. Major and subthreshold depression among older adults seeking vision rehabilitation services. Am J Geriatr Psychiatry. 2005;13(3):180-187. 15. Burmedi D, Becker S, Heyl V, Wahl H-W, Himmelsbach I. Emotional and social consequences of age-related low vision. Vis Impair Res. 2002;4(1):4771. 16. Hayman KJ, Kerse NM, La Grow SJ, Wouldes T, Robertson MC, Campbell AJ. Depression in older people: visual impairment and subjective ratings of health. Optom Vis Sci. 2007;84(11):1024-1030. 17. Mathew RS, Delbaere K, Lord SR, Beaumont P, Vaegan, Madigan MC. Depressive symptoms and quality of life in people with age-related macular degeneration. Ophthalmic Physiol Opt. 2011;31(4):375-380. 18. Haddad S, Chen CA, Santangelo SL, Seddon JM. The genetics of age-related macular degeneration: a review of progress to date. Surv Ophthalmol. 2006;51(4):316-363. 19. Lim LS, Mitchell P, Seddon JM, Holz FG, Wong TY. Age-related macular degeneration. Lancet. 2012;379(9827):1728-1738. 20. Age-Related Eye Disease Study Research Group. Risk factors associated with age-related macular degeneration. A case-control study in the age-related eye disease study: Age-Related Eye Disease Study Report Number 3. Ophthalmology. 2000;107(12):2224-2232. 21. Smith W, Assink J, Klein R, et al. Risk factors for age-related macular degeneration: Pooled findings from three continents. Ophthalmology. 2001; 108(4):697-704. 22. Hyman LG, Lilienfeld AM, Ferris FL 3rd, Fine SL. Senile macular degeneration: a case-control study. Am J Epidemiol. 1983;118(2):213-227. 23. Klein R, Klein BE, Knudtson MD, Meuer SM, Swift M, Gangnon RE. Fifteen-year cumulative incidence of age-related macular degeneration: the Beaver Dam Eye Study. Ophthalmology. 2007;114(2):253-262. 24. Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factors for agerelated macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10:31. 25. Rudnicka AR, Jarrar Z, Wormald R, Cook DG, Fletcher A, Owen CG. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: a meta-analysis. Ophthalmology. 2012; 119(3):571-580. 26. Sin HP, Liu DT, Lam DS. Lifestyle modification, nutritional and vitamins supplements for age-related macular degeneration. Acta Ophthalmol. 2013;91(1):6-11. 27. Shahid H, Khan JC, Cipriani V, et al; Genetic Factors in AMD Study Group. Age-related macular degeneration: the importance of family history as a risk factor. Br J Ophthalmol. 2012;96(3):427-431. 28. Friedman DS, Katz J, Bressler NM, Rahmani B, Tielsch JM. Racial differences in the prevalence of age-related macular degeneration: the Baltimore Eye Survey. Ophthalmology. 1999;106(6):1049-1055. 29. Clemons TE, Milton RC, Klein R, Seddon JM, Ferris FL 3rd. Age-Related Eye Disease Study Research G. Risk factors for the incidence of Advanced AgeRelated Macular Degeneration in the Age-Related Eye Disease Study (AREDS) AREDS report no. 19. Ophthalmology. 2005;112(4):533-539. 30. Reynolds R, Rosner B, Seddon JM. Serum lipid biomarkers and hepatic lipase gene associations with age-related macular degeneration. Ophthalmology. 2010;117(10):1989-1995. 31. Mitchell P, Smith W, Wang JJ. Iris color, skin sun sensitivity, and age-related maculopathy. The Blue Mountains Eye Study. Ophthalmology. 1998;105(8): 1359-1363. 32. Cugati S, Mitchell P, Rochtchina E, Tan AG, Smith W, Wang JJ. Cataract surgery and the 10-year incidence of age-related maculopathy: the Blue Mountains Eye Study. Ophthalmology. 2006;113(11):2020-2025. 33. Chew EY, Sperduto RD, Milton RC, et al. Risk of advanced age-related macular degeneration after cataract surgery in the Age-Related Eye Disease Study: AREDS report 25. Ophthalmology. 2009;116(2):297-303. 34. McCarty CA, Mukesh BN, Fu CL, Mitchell P, Wang JJ, Taylor HR. Risk factors for age-related maculopathy: the Visual Impairment Project. Arch Ophthalmol. 2001;119(10):1455-1462. 35. Adams MK, Chong EW, Williamson E, et al. 20/20 – Alcohol and agerelated macular degeneration: the Melbourne Collaborative Cohort Study. Am J Epidemiol. 2012;176(4):289-298. 36. Chong EW, Kreis AJ, Wong TY, Simpson JA, Guymer RH. Alcohol consumption and the risk of age-related macular degeneration: a systematic review and meta-analysis. Am J Ophthalmol. 2008;145(4):707-715. 37. Liew G, Mitchell P, Wong TY, Rochtchina E, Wang JJ. The association of aspirin use with age-related macular degeneration. JAMA Intern Med. 2013;173(4):258-264. 38. Schaumberg DA, Christen WG, Hankinson SE, Glynn RJ. Body mass index and the incidence of visually significant age-related maculopathy in men. Arch Ophthalmol. 2001;119(9):1259-1265. 39. Seddon JM, Cote J, Davis N, Rosner B. Progression of age-related macular degeneration: association with body mass index, waist circumference, and waist-hip ratio. Arch Ophthalmol. 2003;121(6):785-792. 40. Cheung N, Wong TY. Obesity and eye diseases. Surv Ophthalmol. 2007; 52(2):180-195. 41. Cruickshanks KJ, Klein R, Klein BE. Sunlight and age-related macular degeneration. The Beaver Dam Eye Study. Arch Ophthalmol. 1993;111(4):514-518. 42. Delcourt C, Carriere I, Ponton-Sanchez A, Fourrey S, Lacroux A, Papoz L, POLA Study Group. Light exposure and the risk of age-related macular degeneration: the Pathologies Oculaires Liées à l’Age (POLA) study. Arch Ophthalmol. 2001;119(10):1463-1468. 43. Sui GY, Liu GC, Liu GY, et al. Is sunlight exposure a risk factor for agerelated macular degeneration? A systematic review and meta-analysis. Br J Ophthalmol. 2013;97(4):389-394. 44. Somani S, Hoskin-Mott A, Mishra A, et al. Managing patients at risk for age-related macular degeneration: a Canadian strategy. Can J Optom. 2009;71(2):14-20. 45. Patel PJ, Chen FK, Da Cruz L, Rubin GS, Tufail A. Test-retest variability of reading performance metrics using MNREAD in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52(6):3854-3859. 46. Tarita-Nistor L, Gonzalez EG, Markowitz SN, Steinbach MJ. Binocular interactions in patients with age-related macular degeneration: acuity summation and rivalry. Vision Res. 2006;46(16):2487-2498. 47. Thayaparan K, Crossland MD, Rubin GS. Clinical assessment of two new contrast sensitivity charts. Br J Ophthalmol. 2007;91(6):749-752. 48. Dougherty BE, Flom RE, Bullimore MA. An evaluation of the Mars Letter Contrast Sensitivity Test. Optom Vis Sci. 2005;82(11):970-975. 7 49. DeCarlo DK, McGwin G Jr, Searcey K, et al. Trial frame refraction versus autorefraction among new patients in a low-vision clinic. Invest Ophthalmol Vis Sci. 2013;54(1):19-24. 50. Fletcher DC, Schuchard RA, Renninger LW. Patient awareness of binocular central scotoma in age-related macular degeneration. Optom Vis Sci. 2012;89(9):1395-1398. 51. Sulzbacher F, Kiss C, Kaider A, et al. Correlation of SD-OCT features and retinal sensitivity in neovascular age-related macular degeneration. Invest Ophthalmol Vis Sci. 2012;53(10):6448-6455. 52. Mathew R, Richardson M, Sivaprasad S. Predictive value of spectraldomain optical coherence tomography features in assessment of visual prognosis in eyes with neovascular age-related macular degeneration treated with ranibizumab. Am J Ophthalmol. 2013;155(4):720-726. 53. Acton JH, Smith RT, Hood DC, Greenstein VC. Relationship between retinal layer thickness and the visual field in early age-related macular degeneration. Invest Ophthalmol Vis Sci. 2012;53(12):7618-7624. 54. Cruess AF, Berger A, Colleaux K, et al. Canadian expert consensus: optimal treatment of neovascular age-related macular degeneration. Can J Ophthalmol. 2012;47(3):227-235. 55. Neuner B, Komm A, Wellmann J, et al. Smoking history and the incidence of age-related macular degeneration – results from the Muenster Aging and Retina Study (MARS) cohort and systematic review and meta-analysis of observational longitudinal studies. Addict Behav. 2009;34(11): 938-947. 56. Age-Related Eye Disease Study Research Group. A randomized, placebocontrolled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119(10):1417-1436. 57. Evans JR, Lawrenson JG. Antioxidant vitamin and mineral supplements for slowing the progression of age-related macular degeneration. Cochrane Database Syst Rev. 2012;11:CD000254. 58. van Leeuwen R, Boekhoorn S, Vingerling JR, et al. Dietary intake of antioxidants and risk of age-related macular degeneration. JAMA. 2005;294(24): 3101-3107. 59. Tan JS, Wang JJ, Flood V, Mitchell P. Dietary fatty acids and the 10-year incidence of age-related macular degeneration: the Blue Mountains Eye Study. Arch Ophthalmol. 2009;127(5):656-665. 60. Evans JR, Lawrenson JG. Antioxidant vitamin and mineral supplements for preventing age-related macular degeneration. Cochrane Database Syst Rev. 2012;6:CD000253. 61. Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: The Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 2013; 309(19):2005-2015. 62. Renaud J, Bedard E. Depression in the elderly with visual impairment and its association with quality of life. Clin Interv Aging. 2013;8:931-943. 63. Clemons TE, Rankin MW, McBee WL; Age-Related Eye Disease Study Research Group. Cognitive impairment in the Age-Related Eye Disease Study: AREDS report no. 16. Arch Ophthalmol. 2006;124(4):537-543. 64. Baker ML, Wang JJ, Rogers S, et al. Early age-related macular degeneration, cognitive function, and dementia: the Cardiovascular Health Study. Arch Ophthalmol. 2009;127(5):667-673. 65. Rovner BW, Casten RJ, Massof RW, Leiby BE, Tasman WS; Wills Eye AMD Study. Psychological and cognitive determinants of vision function in agerelated macular degeneration. Arch Ophthalmol. 2011;129(7):885-890. 66. Robillard N, Overbury O. Quebec model for low vision rehabilitation. Can J Ophthalmol. 2006;41(3):362-366. 67. Novartis Pharmaceuticals Canada Inc. Lucentis® (ranibizumab injection) Product Monograph. Date of authorization: December 13, 2011. 68. Rosenfeld PJ, Brown DM, Heier JS, et al; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419-1431. 69. Brown DM, Kaiser PK, Michels M, et al; ANCHOR Study Group. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432-1444. 70. Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T; ANCHOR Study Group. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57-65. 71. Kaiser PK, Blodi BA, Shapiro H, Acharya NR; MARINA Study Group. Angiographic and optical coherence tomographic results of the MARINA study of ranibizumab in neovascular age-related macular degeneration. Ophthalmology. 2007;114(10):1868-1875. 72. Sadda SR, Stoller G, Boyer DS, Blodi BA, Shapiro H, Ianchulev T. Anatomical benefit from ranibizumab treatment of predominantly classic neovascular age-related macular degeneration in the 2-year ANCHOR study. Retina. 2010;30(9):1390-1399. 73. Spaide RF, Laud K, Fine HF, et al. Intravitreal bevacizumab treatment of choroidal neovascularization secondary to age-related macular degeneration. Retina. 2006;26(4):383-390. 74. Emerson MV, Lauer AK, Flaxel CJ, et al. Intravitreal bevacizumab (Avastin) treatment of neovascular age-related macular degeneration. Retina. 2007; 27(4):439-444. 75. Pedersen R, Soliman W, Lund-Andersen H, Larsen M. Treatment of choroidal neovascularization using intravitreal bevacizumab. Acta Ophthalmol Scand. 2007;85(5):526-533. 76. Aggio FB, Farah ME, Silva WC, Melo GB. Intravitreal bevacizumab for exudative age-related macular degeneration after multiple treatments. Graefes Arch Clin Exp Ophthalmol. 2007;245(2):215-220. 77. Hoffmann-La Roche Ltd. Avastin® (bevacizumab for injection) Product Monograph. Date of authorization: February 23, 2012. 78. CATT Research Group; Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ. Ranibizumab and bevacizumab for neovascular agerelated macular degeneration. N Engl J Med. 2011;364(20):1897-1908. 79. Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group; Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119(7): 13881398. 80. Bayer Inc. Eylea® (aflibercept) Product Monograph. Date of approval: November 8, 2013. 81. Heier JS, Brown DM, Chong V, et al; VIEW 1 and VIEW 2 Study Groups. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537-2548. 82. Priya RR, Chew EY, Swaroop A. Genetic studies of age-related macular degeneration: lessons, challenges, and opportunities for disease management. Ophthalmology. 2012;119(12):2526-2536. 83. Schwartz SD, Hubschman JP, Heilwell G, et al. Embryonic stem cell trials for macular degeneration: a preliminary report. Lancet. 2012;379(9817): 713720. The authors stated that they have no disclosures to report in association with the contents of this issue. Change of address notices and requests for subscriptions for Optometry Rounds are to be sent by mail to P.O. Box 310, Station H, Montreal, Quebec H3G 2K8 or by fax to (514) 932-5114 or by e-mail to [email protected]. Please reference Optometry Rounds in your correspondence. Undeliverable copies are to be sent to the address above. Publications Post #40032303 A Partnership for Excellence in Continuing Optometry Education Optometry Rounds is made possible through independent sponsorships from Alcon Canada and Novartis Pharmaceuticals Canada Inc. © 2014 School of Optometry & Vision Science, University of Waterloo, and School of Optometry, University of Montreal, which are solely responsible for the contents. The opinions expressed in this publication do not necessarily reflect those of the publisher or sponsor, but rather are those of the authoring institution based on the available scientific literature. Publisher: SNELL Medical Communication Inc. in cooperation with the School of Optometry & Vision Science, University of Waterloo, and School of Optometry, University of Montreal. All rights reserved. The administration of any therapies discussed or referred to in Optometry Rounds should always be consistent with the approved prescribing information Canada. 149-006E