Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
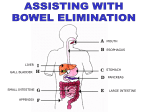
Bowel Elimination Scientific Knowledge Base Mouth Esophagus Digestion begins with mastication. Peristalsis moves food into the stomach. Stomach Small intestine Stores food; mixes food, liquid, and digestive juices; moves food into small intestines Duodenum, jejunum, and ileum Large intestine Anus The primary organ of bowel elimination Expels feces and flatus from the rectum Nursing Knowledge Base: Factors Affecting Bowel Elimination Age Fluid intake Diet Physical activity Psychological factors Personal habits Position during defecation Pain Pregnancy Surgery and anesthesia Medications, laxatives, and cathartics Diagnostic tests Bristol Stool Form Scale Common Bowel Elimination Problems Constipation Impaction A symptom, not a disease; infrequent stool and/or hard, dry, small stools that are difficult to eliminate Results from unrelieved constipation; a collection of hardened feces wedged in the rectum that a person cannot expel Diarrhea Incontinence an increase in the number of stools and the passage of liquid, unformed feces Inability to control passage of feces and gas to the anus Flatulence Hemorrhoids Accumulation of gas in the intestines causing the walls to stretch Dilated, engorged veins in the lining of the rectum Common Bowel Elimination Problems Constipation A symptom, not a disease; infrequent stool and/or hard, dry, small stools that are difficult to eliminate Signs of constipation • infrequent bowel movements (less often than every 3 days) • difficulty passing stools • excessive straining • inability to defecate at will • hard feces. Nursing Diagnosis • (Risk for) Constipation R/T – Opiate containing meds – Decreased fiber intake – Decreased fluid intake – Recent anesthesia – Stress – Inactivity (immobility) – Eating a large amount of dairy products AEB no stool in 3 days • Outcome: Pt will have a soft, formed stool in 24 hours. 7 Assessments • Assess for s/s of constipation – Decrease in frequency of bowel movements – Consistency of stool – Anorexia – Abdominal distention and pain – Feeling of fullness or pressure in rectum – Straining during defecation • Assess bowel sounds 8 Therapeutic Interventions • Encourage fluid intake of at least 1500 ml/24hr • Encourage activity: walk pt in hallway 4 times a day • Encourage to defect whenever urge is felt • Assist to BR, BSC or bedpan (put pt in high Fowlers) • Provide for privacy • Encourage to drink hot liquids in AM • Administer laxatives or enemas as ordered • Consult with HCP to check for impaction 9 Teaching • Teach to increase intake of foods high in fiber • Teach importance of activity • Teach reasons for changing opioid medication to a non-opioid medication 10 Common Bowel Elimination Problems Impaction Digital removal of stool Results from unrelieved constipation; a collection of hardened feces wedged in the rectum that a person cannot expel A health care provider’s order is necessary to remove an impaction. Digital removal of stool 11 Common Bowel Elimination Problems Diarrhea an increase in the number of stools and the passage of liquid, unformed feces 12 Nursing Diagnoses • • • • • Diarrhea Risk for impaired skin integrity Risk for Electrolyte imbalance Risk for imbalanced fluid volume Risk for falls 13 Common Bowel Elimination Problems Incontinence Inability to control passage of feces and gas to the anus Nursing Diagnosis Impaired Body Image Impaired Social Interaction • Common causes of fecal incontinence include diarrhea, constipation, and muscle or nerve damage. – – – – – Spinal cord injury Multiple Sclerosis Stroke Intestinal obstruction Seizures 14 Common Bowel Elimination Problems Flatulence Accumulation of gas in the intestines causing the walls to stretch Causes • Swallowed air • Foods and beverages • Medicines or nutritional supplements • Bowel obstruction • Nursing Diagnoses – Pain – Impaired body image 15 Common Bowel Elimination Problems Hemorrhoids Dilated, engorged veins in the lining of the rectum Causes • • • • Diarrhea Constipation Pregnancy Cirrhosis of the Liver • Nursing Diagnosis – Pain 16 Bowel Diversion • Temporary or permanent artificial opening in the abdominal wall – Stoma • Surgical opening in the ileum or colon – Ileostomy or colostomy • The standard bowel diversion creates a stoma. End Colostomy Double-Barrel Colostomy Ostomies • End ileostomy • End colostomy – Proximal end forms stoma, and distal end is removed or sewn closed. • Double-barrel colostomy – Bowel is surgically cut, and both ends are brought through the abdomen. Psychological Considerations • Nursing Diagnosis: –Disturbed body image Continuing and Restorative Care • Irrigating a Colostomy Continuing and Restorative Care • Pouching ostomies – An effective pouching system protects the skin, contains fecal material, remains odor free, and is comfortable and inconspicuous. 23 Continuing and Restorative Care • Nutritional considerations – Consume low fiber for the first weeks. – Eat slowly and chew food completely. – Drink 10 to 12 glasses of water daily. – Patient may choose to avoid gassy foods. Implementations: Acute Care • Health promotion – Promotion of normal defecation • Establish a routine an hour after a meal, or maintain the patient’s routine. – Sitting position – Privacy – Positioning on bedpan Fecal Occult Blood Testing 26 Acute Care: Medications • Cathartics and laxatives – Bulk Forming • Psyllium (Metamucil) – Emollient or Wetting • Docusate Sodium (Colace) – Saline • Magnesium Hydroxide (Milk of Magnesia) • Sodium phosphate (Fleet enema) – Stimulant • Bisacodyl (Dulcolax) • Casanthranol (Peri-Colace) Implementations: Acute Care • Health promotion – Promotion of normal defecation • Establish a routine an hour after a meal, or maintain the patient’s routine. – Sitting position – Privacy – Positioning on bedpan Acute Care: Medications • Cathartics and laxatives – Bulk Forming • Psyllium (Metamucil) – Emollient or Wetting • Docusate Sodium (Colace) – Saline • Magnesium Hydroxide (Milk of Magnesia) • Sodium phosphate (Fleet enema) – Stimulant • Bisacodyl (Dulcolax) • Casanthranol (Peri-Colace) Acute Care: Medications • Antidiarrheal agents – Diphenoxylate (Lomotil) – Over the counter (Imodium) – Opiates used with caution Enemas • Enema administration – Sterile technique is unnecessary. – Wear gloves. – Explain the procedure, precautions to avoid discomfort, and length of time necessary to retain the solution before defecation. Enemas Cleansing Enemas Tap water •is hypotonic and exerts an osmotic pressure lower than fluid in interstitial spaces. After infusion into the colon, tap water escapes from the bowel lumen into interstitial spaces. The net movement of water is low. The infused volume stimulates defecation before large amounts of water leave the bowel. Do not repeat tap water enemas because water toxicity or circulatory overload develops if the body absorbs large amounts of water. Normal saline safest solution to use because it exerts the same osmotic pressure as fluids in interstitial spaces surrounding the bowel. The volume of infused saline stimulates peristalsis. Giving saline enemas does not create the danger of excess fluid absorption 32 Enemas Cleansing Enemas Hypertonic solution •infused into the bowel exert osmotic pressure that pulls fluids out of interstitial spaces. The colon fills with fluid, and the resultant distention promotes defecation. Patients unable to tolerate large volumes of fluid benefit most from this type of enema, which is by design low volume. This type of enema is contraindicated for patients who are dehydrated and for young infants. A hypertonic solution of 120 to 180 mL (4 to 6 oz) is usually effective. The commercially prepared Fleet enema is the most common. Soapsuds •to create the effect of intestinal irritation to stimulate peristalsis. Use only pure castile soap that comes in liquid form and is included in most soapsuds enema kits. Use soapsuds enemas with caution in pregnant women and older adults because they cause electrolyte imbalance or damage to the intestinal mucosa. 33 Enemas Oil Retention Enemas •lubricate the rectum and colon. The feces absorb the oil and become softer and easier to pass. To enhance the action of the oil, the patient retains the enema for several hours if possible. Carminative Enema provide relief from gaseous distention Medication enemas Kayexalate Neomycin Lactolosis An example is sodium polystyrene sulfonate (Kayexalate), which is used to treat patients with dangerously high serum potassium levels. This drug contains a resin that exchanges sodium ions for potassium ions in the large intestine. Another medicated enema is neomycin solution, an antibiotic that is used to reduce bacteria in the colon before bowel surgery. 34 Continuing and Restorative Care • Bowel training – Training program – Diet – Promotion of regular exercise – Management of hemorrhoids • Skin integrity