Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
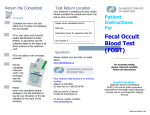
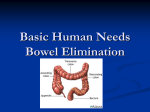
• • • • • • • • • • • • • • • • • • • • • • • • • • • The Large Intestine Primary organ of bowel elimination Extends from the ileocecal valve to the anus Functions – Absorption of water – Formation of feces – Expulsion of feces from the body The Small and Large Intestines Process of Peristalsis Peristalsis is under control of the nervous system. Contractions occur every 3 to 12 minutes. Mass peristalsis sweeps occur one to four times each 24-hour period. One-third to one-half of food waste is excreted in stool within 24 hours. Peristaltic Movements in the Intestine Variables Influencing Bowel Elimination Developmental considerations Daily patterns Food and fluid Activity and muscle tone Lifestyle Psychological variables Pathologic conditions Medications Diagnostic studies Surgery and anesthesia Developmental Considerations Infants: Characteristics of stool and frequency depend on formula or breast feedings. Toddler: Physiologic maturity is the first priority for bowel training. Child, adolescent, adult: Defecation patterns vary in quantity, frequency, and rhythmicity. Older adult: Constipation is often a chronic problem; diarrhea and fecal incontinence may result from physiologic or lifestyle changes. • Question Which food is a recommended for an older adult who is constipated? A. Cheese B. Fruit C. Cabbage D. Eggs • Answer Answer: B. Fruit Rationale: Fruits and vegetables have a laxative effect on the system. Cheese and eggs have a constipating effect and cabbage, although a vegetable, produces gas in the system. • Foods Affecting Bowel Elimination • Constipating foods: cheese, lean meat, eggs, pasta • Foods with laxative effect: fruits and vegetables, bran, chocolate, alcohol, coffee • Gas-producing foods: onions, cabbage, beans, cauliflower • Effect of Medications on Stool • Aspirin, anticoagulants: pink to red to black stool • Iron salts: black stool • Antacids: white discoloration or speckling in stool • Antibiotics: green-gray color • Physical Assessment of the Abdomen • Inspection: observe contour, any masses, scars, or distention • Auscultation: listen for bowel sounds in all quadrants – Note frequency and character, audible clicks, and flatus. – Describe bowel sounds as hypoactive, hyperactive, absent or infrequent. • Percussion and palpations: performed by advanced practice professionals – Physical Assessment of the Anus and Rectum • Inspection and palpation – Lesions, ulcers, fissures (linear break on the margin of the anus), inflammation, and external hemorrhoids – Ask the patient to bear down as though having a bowel movement. Assess for the appearance of internal hemorrhoids or fissures and fecal masses. – Inspect perineal area for skin irritation secondary to diarrhea or fecal incontinence. • Stool Collection • Medical aseptic technique is imperative. • Hand hygiene, before and after glove use, is essential. • Wear disposable gloves. • Do not contaminate outside of container with stool. • Obtain stool and package, label, and transport according to agency policy. • Patient Guidelines for Stool Collection • • • • Void first so that urine is not in stool sample. Defecate into the container rather than toilet bowl. Do not place toilet tissue in the bedpan or specimen container. Notify nurse when specimen is available. • Question Tell whether the following statement is true or false. When collecting stool using the technique “timed specimen,” the nurse should consider the first stool passed by the patient as the start of the collection period. A. True B. False • Answer Answer: A. True Rationale: When collecting stool using the technique “timed specimen,” the nurse should consider the first stool passed by the patient as the start of the collection period. • Types of Direct Visualization Studies (Endoscopy) • Esophagogastroduodenoscopy • Colonoscopy • Sigmoidoscopy • Wireless capsule endoscopy • Question Which of the following direct visualization tests uses a long, flexible, fiberoptic–lighted scope to visualize the rectum, colon, and distal small bowel? A. Esophagogastroduodenoscopy B. Colonoscopy C. Sigmoidoscopy D. UGI series • Answer Answer: B. Colonoscopy Rationale: A colonoscopy visualizes the rectum, colon, and bowel using a lighted scope. An esophagogastroduodenoscopy examines the esophagus, stomach, and upper duodenum through an optic scope. A sigmoidoscopy examines the distal sigmoid colon, rectum, and anal canal through a flexible or rigid sigmoidoscope. UGI series involves fluoroscopic examination of the esophagus, stomach, and small intestine after ingestion of barium sulfate. • Indirect Visualization Studies • Upper gastrointestinal (UGI) • Small bowel series • Barium enema • Abdominal ultrasound • Magnetic resonance imaging (MRI) • Abdominal CT scan • Scheduling Diagnostic Tests • 1: fecal occult blood test • 2: barium studies (should precede UGI) • 3: endoscopic examinations Noninvasive procedures take precedence over invasive procedures • Patient Outcomes for Normal Bowel Elimination • Patient has a soft, formed bowel movement every 1 to 3 days without discomfort. • The relationship between bowel elimination and diet, fluid, and exercise is explained. • Patient should seek medical evaluation if changes in stool color or consistency persist. • Promoting Regular Bowel Habits • Timing • Positioning • Privacy • Nutrition • Exercise – Abdominal settings – Thigh strengthening • Individuals at High Risk for Constipation • Patients on bedrest taking constipating medicines • Patients with reduced fluids or bulk in their diet • Patients who are depressed • Patients with central nervous system disease or local lesions that cause pain while defecating • Nursing Measures for the Patient With Diarrhea • Answer call bells immediately. • Remove the cause of diarrhea whenever possible (e.g., medication). • If there is impaction, obtain physician order for rectal examination. • Give special care to the region around the anus. • Preventing Food Poisoning • Never buy food with damaged packaging. • Take items requiring refrigeration home immediately. • Wash hands and surfaces often. • Use separate cutting boards for foods. • Thoroughly wash all fruits and vegetables before eating. • Do not wash meat, poultry, or eggs to prevent spreading microorganisms to sink and other kitchen surfaces. • Never use raw eggs in any form. • Do not eat seafood raw or if it has an unpleasant odor. • Preventing Food Poisoning (cont.) • Use a food thermometer to ensure cooking food to safe internal temperature. • Keep food hot after cooking; maintain safe temperature of 140°F or above. • Give only pasteurized fruit juices to small children. • Methods of Emptying the Colon of Feces • Enemas • Rectal suppositories • Oral intestinal lavage • Digital removal of stool • Types of Enemas • Cleansing • Retention – Oil – Carminative – Medicated – Anthelmintic • Large volume • Small volume • Question Which enema would be used for a patient with intestinal parasites? A. Oil-retention enema B. Carminative enema C. Nutritive enema D. Anthelmintic enema • Answer Answer: D. Anthelmintic enema Rationale: Antihelmintic enemas destroy intestinal parasites. Oilretention enemas lubricate the stool and intestinal mucosa, making defecation easier. Carminative enemas help expel flatus from the rectum. Nutritive enemas administer fluids and nutrition rectally. • Retention Enemas • Oil-retention: lubricate the stool and intestinal mucosa, easing defecation • Carminative: help expel flatus from the rectum • Medicated: provide medications absorbed through the rectal mucosa • Anthelmintic: destroy intestinal parasites • Bowel-Training Programs • Manipulate factors within the patient’s control. – Food and fluid intake, exercise, and time for defecation – Eliminate a soft, formed stool at regular intervals without laxatives. • When achieved, continue to offer assistance with toileting at the successful time. • Nasogastric Tubes • Inserted to decompress or drain the stomach of fluid or unwanted stomach contents • Used to allow the gastrointestinal tract to rest before or after abdominal surgery to promote healing • Inserted to monitor gastrointestinal bleeding • Types of Ostomies • Sigmoid colostomy • Descending colostomy • Transverse colostomy • Ascending colostomy • Ileostomy • Location of (A) a Sigmoid Colostomy and (B) a Descending Colostomy • Location of (C) a Transverse Colostomy and (D) an Ascending Colostomy • Location of an Ileostomy • Colostomy Care • Keep the patient as free of odors as possible; empty the appliance frequently. • Inspect the patient’s stoma regularly. – Note the size, which should stabilize within 6 to 8 weeks. – Keep the skin around the stoma site clean and dry. • Measure the patient’s fluid intake and output. • Explain each aspect of care to the patient and self-care role. • Encourage patient to care for and look at ostomy. • Comparison of Stomal Appearance • Patient Teaching for Colostomies • Explain the reason for bowel diversion and the rationale for treatment. • Demonstrate self-care behaviors that effectively manage the ostomy. • Describe follow-up care and existing support resources. • Report where supplies may be obtained in the community. • Verbalize related fears and concerns. • Demonstrate a positive body image. • Comfort Measures • Encourage recommended diet and exercise. • Use medications only as needed. • Apply ointments or astringent (witch hazel). • Use suppositories that contain anesthetics.