Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
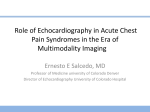
Acute Aortic Dissection: Clinician Update Alan C. Braverman Circulation 2010;122;184-188 DOI: 10.1161/CIRCULATIONAHA.110.958975 Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX 72514 Copyright © 2010 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/cgi/content/full/122/2/184 Data Supplement (unedited) at: http://circ.ahajournals.org/cgi/content/full/122/2/184/DC1 Subscriptions: Information about subscribing to Circulation is online at http://circ.ahajournals.org/subscriptions/ Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Fax: 410-528-8550. E-mail: [email protected] Reprints: Information about reprints can be found online at http://www.lww.com/reprints Downloaded from circ.ahajournals.org by on July 19, 2010 CLINICIAN UPDATE Acute Aortic Dissection Clinician Update Alan C. Braverman, MD A 27-year-old previously healthy woman presented to the emergency room after the sudden onset of severe chest pain and shortness of breath during the 37th week of pregnancy. Her examination was remarkable for a blood pressure of 118/ 70 mm Hg, heart rate of 100 bpm, and respiratory rate of 24 breaths per minute. The cardiovascular examination was notable for a soft systolic ejection murmur, and the pulmonary and general examinations were unremarkable. ECG demonstrated sinus tachycardia, and her chest x-ray was normal. A D-dimer level was elevated. She underwent a spiral computed tomography scan to evaluate for pulmonary embolism, which instead demonstrated an acute type A aortic dissection and a very small patent ductus arteriosus. The patient underwent emergency cesarean section, which delivered a viable baby, and repair of the type A dissection. Her aortic valve was trileaflet. She had no features on examination to suggest Marfan syndrome or Loeys-Dietz aneurysm syndrome. Her father had died suddenly at 31 years of age of a “presumed heart attack,” and her paternal uncle had undergone ascending aortic aneurysm resection at 42 years of age. Mutation analysis in this woman detected a heterozygous mutation in MYH11, confirming familial thoracic aortic aneurysm/dissection (TAA/D). Acute aortic dissection is the most common life-threatening disorder affecting the aorta.1 The immediate mortality rate in aortic dissection is as high as 1% per hour over the first several hours, making early diagnosis and treatment critical for survival. Classification schemes for aortic dissection are based on anatomic involvement of the aortic dissection (Figure 1).2 In the DeBakey classification, type I dissections originate in the ascending aorta and extend to at least the aortic arch; type II dissections involve the ascending aorta only; and type III dissections begin in the descending aorta, usually just distal to the left subclavian artery. In the Stanford classification, type A dissections involve the ascending aorta, and type B dissections are those that do not involve the ascending aorta. Ascending dissections require emergency surgical repair, whereas medical therapy is usually the initial strategy for acute type B dissections. Ascending aortic dissection is most common in the 50- to 60-year age range, whereas descending dissections occur more commonly in older individuals. Because acute aortic dissection is much less common than other conditions associated with chest or back pain, a high index of suspicion is important in making this diagnosis. Many conditions are associated with aortic dissection (the Table).2 Hypertension is present in ⬇75% of individuals with aortic dissection. Genetically triggered disorders affecting the aorta are an important and often underrecognized cause of aortic dissection. Marfan syndrome, Loeys-Dietz aneurysm syndrome, vascular EhlersDanlos syndrome, bicuspid aortic valve, Turner syndrome, and familial TAA/D syndrome are all genetic conditions associated with thoracic aortic aneurysm and/or dissection. Prior cardiac surgery, especially aortic valve replacement and aortic manipulation (including angiography and stenting), are risk factors for aortic dissection. Acute hemodynamic stress such as that From the Cardiovascular Division, Department of Medicine, Washington University School of Medicine, St Louis, Mo. The online-only Data Supplement is available with this article at http://circ.ahajournals.org/cgi/content/full/122/2/184/DC1. Correspondence to Alan C. Braverman, MD, FACC, Alumni Endowed Professor of Cardiovascular Diseases, Cardiovascular Division, Department of Medicine, Washington University School of Medicine, 660 S Euclid Ave, Box 8086, St. Louis, MO 63110. E-mail [email protected] (Circulation. 2010;122:184-188.) © 2010 American Heart Association, Inc. Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.110.958975 184 Downloaded from circ.ahajournals.org by on July 19, 2010 Braverman Acute Aortic Dissection 185 Table. Risk Factors for Aortic Dissection Hypertension Genetically triggered thoracic aortic disease Marfan syndrome Bicuspid aortic valve Loeys-Dietz syndrome Hereditary TAA/D Vascular Ehlers-Danlos syndrome Congenital diseases/syndromes Coarctation of the aorta Turner syndrome Tetralogy of Fallot Atherosclerosis Penetrating atherosclerotic ulcer Trauma, blunt, or iatrogenic Catheter/stent Intraaortic balloon pump Aortic/vascular surgery Motor vehicle accident Coronary artery bypass surgery/aortic valve replacement Figure 1. Classification schemes of acute aortic dissection. Reprinted with permission from Braverman et al.2© Elsevier. In press. Cocaine use Inflammatory/infectious diseases Giant cell arteritis encountered with cocaine use, pheochromocytoma, and heavy weightlifting has been associated with aortic dissection. Aortic dissection may complicate aortitis, most commonly giant cell arteritis. Acute aortic dissection complicating pregnancy is uncommon. It usually occurs during labor and delivery or in the early postpartum period. Although hormonal changes in the aortic wall have been theorized as potentially playing a role, an underlying genetic disorder associated with abnormalities of the aortic wall such as that present in familial TAA/D, Marfan syndrome, Loeys-Dietz aneurysm syndrome, vascular Ehlers-Danlos syndrome, bicuspid aortic valve, Turner syndrome, or other genetic disorder is the most likely underlying cause for aortic dissection complicating pregnancy. Cystic medial degeneration is the pathology underlying many thoracic aortic aneurysms and dissections. Abnormalities in the transforming growth factor- pathway and abnormalities in smooth muscle cell contractile element function may underlie certain aortic dissections.3 Patients with thoracic aortic aneurysms from any cause are at risk for aortic dissection, with absolute size (especially ⬎5 to 6 cm), age, body surface area, sex, rate of growth, and specific genetic disorder all modulating risk of dissection. Clinical Manifestations The symptoms of aortic dissection may be highly variable and may mimic much more common conditions. Thus, a high index of suspicion must be maintained, especially when risk factors for dissection are present or signs and symptoms suggest this possibility. The vast majority of patients with acute dissection have sudden, severe chest, back, or abdominal pain, which may be maximal at its onset. The pain may be migratory or may radiate from chest or back to the abdomen or to the lower extremities. However, in some instances, the pain resolves and symptoms may be referable to other com- Takayasu arteritis Behȩt disease Aortitis Syphilis Pregnancy Reprinted with permission from Braverman et al.2 © Elsevier. In press. plications such as heart failure from acute aortic regurgitation, neurological deficits, syncope, or vascular insufficiency. Although most patients with type B dissections are hypertensive, many patients with type A dissections are normotensive or hypotensive on presentation.1 Hypotension complicating acute aortic dissection is usually related to cardiac tamponade, aortic rupture, or heart failure associated with severe aortic regurgitation. Sudden chest or back pain accompanied by pulse deficits, aortic regurgitation, or neurological manifestations should alert the clinician to the diagnosis of acute aortic dissection. However, pulse deficits were present in only 19% of type A Downloaded from circ.ahajournals.org by on July 19, 2010 186 Circulation July 13, 2010 dissection and 9% of type B dissection.1 The murmur of aortic regurgitation was present in 44% of type A dissections and 12% of type B dissections in the International Registry of Acute Aortic Dissection series.1 There are several mechanisms for acute aortic regurgitation in type A dissection, with aortic leaflet prolapse or distortion of leaflet alignment by the dissection flap being most common. Neurological complications of dissection are more common in type A dissections and include stroke, spinal cord ischemia, ischemic neuropathy, and hypoxic encephalopathy. Syncope occurs in 9% of acute dissection and may be caused by cardiac tamponade, aortic rupture, cerebral vessel obstruction, or activation of cerebral baroreceptors. A particularly dangerous complication of dissection is acute myocardial infarction or coronary ischemia related to the dissection flap obstructing coronary flow because it may mask the diagnosis of dissection or lead to inadvertent use of antiplatelet and anticoagulant therapy and delay recognition and treatment of the dissection. Vascular complications involving branch vessels may lead to malperfusion, which may lead to mesenteric or limb ischemia. Renal ischemia or renovascular hypertension may be a result of the dissection process. Leftsided pleural effusions are common with acute dissection and are usually sympathetic effusions, whereas acute hemothorax signals acute aortic rupture or leaking dissection. Laboratory Features The chest x-ray may be the first clue to the diagnosis of aortic dissection, with abnormal aortic contour or widening of the aortic silhouette being present in ⬎80% of acute dissection.1 However, 12% to 15% of patients with acute aortic dissection will have a normal chest x-ray. Thus, it is important to remember that a normal chest x-ray cannot exclude the presence of aortic dissection. The ECG changes in aortic dissection are usually nonspecific, but 1% to 2% of patients have acute ST elevation. Tremendous interest exists in the development of biomarkers that can reliably diagnose or exclude acute aortic dissection. Release of smooth muscle proteins, soluble elastin fragments, myosin heavy chain, and creatine kinase-BB isoform has been reported after aortic dissection, but none are currently available for clinical use.4 As is the case in pulmonary embolism, D-dimer levels are elevated in acute aortic dissection.4 Additionally, in patients presenting within the first 24 hours of symptom onset, a D-dimer level ⬍500 ng/mL had a negative likelihood ratio of 0.07 and a negative predictive value of 95%.4 However, the patency of the true lumen affects D-dimer levels in acute dissection. Dissection variants such as intramural hematoma and penetrating atherosclerotic ulcer may not have elevated D-dimer levels. More studies are required to determine the accuracy of D-dimer assays in acute aortic syndromes and how to best use D-dimer testing in aortic dissection. Diagnostic Techniques Multidetector computed tomography, transesophageal echocardiogram, and magnetic resonance imaging are highly accurate in the diagnosis of aortic dissection (Figure 2).2 In addition to making the diagnosis of aortic dissection or its variants (intramural hematoma and penetrating atherosclerotic ulcer), the imaging must confirm whether the ascending aorta is involved. Other useful information includes anatomic features and complications of the dissection, including entry and reentry sites, extent of dissection, branch vessel involvement, aortic regurgitation, pericardial effusion or hemopericardium, and any signs of rupture. The selection of a specific imaging modality is influenced by individual patient characteristics and variables and institutional capabilities and expertise.5 Contrast computed tomography is the most commonly used modality in diagnos- ing aortic dissection and is readily available in most emergency rooms. Because magnetic resonance imaging takes longer for image acquisition and leaves the patient relatively unmonitored, it is usually not the procedure of first choice. Transesophageal echocardiogram has an advantage in being portable and able to be performed at the bedside for the unstable patient (Movies I and II in the online-only Data Supplement). Although aortic dissection may be diagnosed by transthoracic echocardiogram, the sensitivity and specificity are much lower than with the other diagnostic modalities; thus, this technique is not the first choice for diagnosing dissection. Management Immediate management of aortic dissection includes stabilizing the patient with prompt attention to blood pressure reduction. -Blockers are the first drugs of choice because of their mechanism of lowering the rate of rise of ventricular force (dP/dt) and stress on the aorta. Intravenous agents are chosen for rapid onset. In many instances, multiple blood pressure agents are required. In patients in whom refractory hypertension exists, renovascular hypertension related to the dissection flap must be considered. All patients with acute aortic dissection should undergo multidisciplinary evaluation that includes cardiothoracic and/or vascular surgical consultation. Emergency surgery is recommended for acute type A dissection; initial medical management is recommended for uncomplicated type B dissection. In the International Registry of Acute Aortic Dissection, the mortality rate of patients undergoing surgery for type A dissection was 26% and for those treated medically was 58%.1 Patients with low-risk features have a significantly lower mortality rate than those with malperfusion, shock, or cardiac tamponade. Uncomplicated type B dissection has an in-hospital mortality rate of ⬇10%. Most series of acute type B dissection have reported a mortality rate between Downloaded from circ.ahajournals.org by on July 19, 2010 Braverman Figure 2. Contrast computed tomography scan demonstrating acute type A aortic dissection with enlargement of the ascending aorta and intimal flap (arrow) in the ascending and descending aorta. Both the true lumen (TL) and false lumen are opacified with contrast in this example. Reprinted with permission from Braverman et al.2© Elsevier. In press. 25% and 50% for those requiring emergency surgery. Surgical management of type A dissection involves excision of the intimal tear when possible, obliteration of entry into the false lumen proximally and distally, and interposition graft replacement of the ascending aorta. The aortic valve may need to be replaced, depending on the underlying pathology of the valve and aortic root. Complicated type B dissections may require repair of conditions such as aortic rupture, visceral, or branch vessel ischemia. Endovascular grafts have the potential to treat many complications of type B dissections with relatively low short-term morbidity and mortality rates. Trials are underway to prospectively evaluate endovascular graft therapy in acute complicated type B dissection. Long-Term Management Short- and long-term survival in acute type A dissection has ranged between 52% and 94% at 1 year and 45% and 88% at 5 years.6 The 10-year actuarial survival rate of patients with acute dissection who survive initial hospitalization is reported as 30% to 60% in various studies. One recent study reported a 10-year survival of 55% and 20-year survival of 30% after type A dissection.7 -Blocker– based therapy is the foundation of long-term medical management. Drugs such as angiotensin receptor blockers, by antagonizing transforming growth factor-, may be beneficial in certain genetically triggered disorders, but prospective data after aortic dissection are lacking. Lifelong imaging of the entire aorta at regular intervals is important to survey for aneurysmal enlargement or other complications. Lifestyle modifications, including limitations on physical activity and certain types of employment, are important tenets of management. Although most patients with dissection have underlying hypertension, only a tiny fraction of all hypertensive individuals ever have a dissection. It is imperative that one consider an underlying genetic disorder in the individual with acute aortic dissection and that a comprehensive family history be obtained. Some patients will have syndromic features such as those characteristic of Marfan syndrome or Loeys-Dietz syndrome. The presence of dural ectasia in the lumbosacral spine on the computed tomography or magnetic resonance imaging will often provide a clue to such genetically Acute Aortic Dissection 187 triggered disorders. Bicuspid aortic valve is associated with ascending thoracic aortic aneurysm and risk of aortic dissection and may be familial in ⬇10% of cases.8 As detailed in the case presentation above, familial thoracic aortic aneurysm syndromes are an everexpanding cause of aortic dissection. Comprehensive family studies have recognized that ⬇20% of individuals with a thoracic aortic aneurysm or dissection will have another firstdegree relative with thoracic aortic disease.9 Screening first-degree relatives of the patient with acute aortic dissection for thoracic aortic disease is important. This involves a clinical history, physical examination, and imaging for appropriate candidates. In most patients with familial TAA/D, the disorder is autosomal dominant with decreased penetrance and variable expression. 3 Several genes have been identified in families with thoracic aortic disease, including FBN1, TGFBR1 and 2, ACTA2, and MYH11. ACTA2 mutations have been identified in ⬇14% of TAA/D and have been associated with livedo reticularis, patent ductus arteriosus, and bicuspid aortic valve.3 If a specific gene mutation is determined in a family, all first-degree relatives may be screened for the same mutation. Recognition of individuals at risk for thoracic aortic disease allows prophylactic surgery and lessens risk of aortic dissection. One year has passed since the acute dissection in the patient presented above. Imaging studies have demonstrated no change in the residual aortic dissection. She has been maintained on -blocker and angiotensin receptor blocker therapy. It is likely that her late father’s death was related to an acute aortic dissection instead of a “myocardial infarction.” The patient’s 5 children have undergone evaluation; two, including the one born during the acute aortic dissection, harbor the same mutation in MYH11. It is important to consider genetically triggered disorders in patients with aortic dissection Downloaded from circ.ahajournals.org by on July 19, 2010 188 Circulation July 13, 2010 and to evaluate their first-degree relatives for thoracic aortic disease. Disclosures Dr Braverman is a member of the Professional Advisory Board of the National Marfan Foundation. Dr Braverman has served as an expert witness in cases of aortic dissection with a “modest” relationship. References 1. Hagan PG, Nienaber CA, Isselbacher EM, Bruckman D, Karavite DJ, Russman PL, Evangelista A, Fattori R, Suzuki T, Oh JK, Moore AG, Malouf JF, Pape LA, Gaca C, Sechtem U, Lenferink S, Deutsch HJ, Diedrichs H, Marcos y Robles J, Llovet A, Gilon D, Das SK, Armstrong WF, Deeb GM, Eagle KA. International Registry of Acute Aortic Dissection (IRAD): new insights from an old disease. JAMA. 2000;283:897–903. 2. Braverman AC, Thompson R, Sanchez L. Diseases of the aorta. In: Bonow RO, Mann DL, Zipes DP, Libby P, eds. Braunwald’s Heart Disease. 9th ed. Philadelphia, Pa: Elsevier. In press. 3. Milewicz DM, Guo DC, Tran-Fadulu V, Lafont AL, Papke CL, Inamoto S, Kwartler CS, Pannu H. Genetic basis of thoracic aortic aneurysms and dissections: focus on smooth muscle cell contractile dysfunction. Annu Rev Genomics Hum Genet. 2008;9:283–302. 4. Suzuki T, Distante A, Zizza A, Trimarchi S, Villani M, Salerno Uriarte JA, De Luca Tupputi Schinosa L, Renzulli A, Sabino F, Nowak R, Birkhahn R, Hollander JE, Counselman F, Vijayendran R, Bossone E, Eagle K, for the IRAD-Bio Investigators. Diagnosis of acute aortic dissection by D-dimer: the International Registry of Acute Aortic Dissection Substudy on Biomarkers (IRAD-bio) experience. Circulation. 2009;119:2702–2707. 5. Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE Jr, Eagle KA, Hermann LK, Isselbacher EM, Kazerooni EA, Kouchoukos NT, Lytle BW, Milewicz DM, Reich DL, Sen S, Shinn JA, Svensson LG, Williams DM, for the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; American College of Radiology; American Stroke Association; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society of Thoracic Surgeons; Society for Vascular Medicine. 2010 ACCF/AHA/AATS/ACR/ ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force 6. 7. 8. 9. Downloaded from circ.ahajournals.org by on July 19, 2010 on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010; 121(13):e266 – e369. Tsai TT, Fattori R, Trimarchi S, Isselbacher E, Myrmel T, Evangelista A, Hutchison S, Sechtem U, Cooper JV, Smith DE, Pape L, Froehlich J, Raghupathy A, Januzzi JL, Eagle KA, Nienaber CA. International Registry of Acute Aortic Dissection. Circulation. 2006;114:2226 –2231. Stevens LM, Madsen JC, Isselbacher EM, Khairy P, MacGillivray TE, Hilgenberg AD, Agnihotri AK. Surgical management and long-term outcomes of acute ascending aortic dissection. J Thorac Cardiovasc Surg. 2009;138:1349 –1357. Braverman AC, Beardslee MA. The bicuspid aortic valve. In: Otto C, Bonow R, eds. Valvular Heart Disease: A Companion to Braunwald’s Heart Disease. Philadelphia, Pa: Saunders/Elsevier; 2009;169 –186. Albornoz G, Coady MA, Roberts M, Davies RR, Tranquilli M, Rizzo JA, Elefteriades JA. Familial thoracic aortic aneurysms and dissections: incidence, modes of inheritance, and phenotypic patterns. Ann Thorac Surg. 2006;82:1400 –1405.