Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Transtheoretical model wikipedia , lookup
Medical ethics wikipedia , lookup
Preventive healthcare wikipedia , lookup
Health equity wikipedia , lookup
Rhetoric of health and medicine wikipedia , lookup
Patient safety wikipedia , lookup
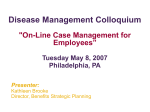
• Cognizant 20-20 Insights Medication Adherence in the Real World Medication non-adherence is a growing concern, as it is increasingly associated with negative health outcomes and higher cost of care. Tackling the burden of non-adherence requires a collaborative, patientcentric approach that considers individual patient needs and results in intelligent interventions that combine high-tech with high-touch. Executive Summary It’s 11:00 AM, and Jack — diagnosed just last week with diabetes — is in a state of uncertainty. His doctor prescribed multiple meds: the critical insulin shot, oral anti-diabetics and multivitamins to build immunity, with a total of five doses to be taken per day. Having just finished a late breakfast, Jack is pondering the instruction to take his meds with breakfast every morning, followed by another dose before noon. He takes out his pill box but wonders, “Should I take both doses together or skip the first one?” Adherence to medication is one of the most intriguing and complex of patient behaviors. Nonadherence to a therapeutic regimen can result in negative outcomes, and it can be compounded in populations with chronic illness because of the extended duration of multiple drug therapies. This white paper explores key issues and provides solutions to crucial challenges concerning medication adherence, including: • How changing industry dynamics are reshaping healthcare delivery. • The impact of non-adherence on healthcare’s so-called Triple Aim. • How non-adherence is being managed today. cognizant 20-20 insights | october 2014 • The causes of non-adherence behavior by patients. • The emerging paradigm of patient centricity in adherence. • How the healthcare industry should tackle the burden of non-adherence. • How adherence is related to return on investment (ROI). Industry Dynamics Reshape Healthcare Delivery The burden of chronic disease is rapidly increasing worldwide. Expected to account for three-fourths of all deaths globally by 20201, chronic illness is straining the healthcare capacity of many countries that lack the resources to provide adequate healthcare services. By 2035, the global shortage of healthcare providers is expected to be 12 million.2 These problems, coupled with increase expenditures on health and long-term care, will continue to put pressure on public budgets over the coming years, with healthcare costs in the U.S. alone expected to reach nearly 4.8 trillion in 2021.3 As these trends continue, more healthcare systems will seek innovations to combat these challenges. Quick Fact A recent study shows that nearly half of the pharmaceuticals industry (45.7%) believes that value-added services and a ”beyond the pill” strategy will show a financial return within two to three years.7 Growth Opportunities Meanwhile, industry growth has been fostered by an aging population, the prevalence of chronic disease and increased physician acceptance of home care, a market that was estimated at nearly $74 billion in 2013.4 The industry will continue to transition toward cost-efficient treatment options from public and private payers.5 Increasing adoption of smartphones, as well as the prevalence of 3G and 4G networks, are significantly boosting the use of mobile platforms for providing healthcare services; indeed, by 2015, approximately 500 million people will use healthcare apps on their mobile device.6 All of these trends are culminating in a digital revolution and sparking a set of innovative services to combat the challenges facing the healthcare system. Industry interest in patient engagement has spiked, influenced by the release in late August 2012 of the Meaningful Use Stage 2 Final Rule by the U.S. Centers for Medicare & Medicaid Services (CMS). Now that patient engagement is being called the biggest blockbuster drug of the century, pharmaceuticals and healthcare industry players need to reconfigure their resources to develop innovative business models that are based on value-added services related to prescription drugs for chronic conditions. Non-adherence and the Triple Healthcare Aim Understanding and addressing the impact of medication non-adherance dovetails perfectly with healthcare’s Triple Aim, a framework developed by the Institute for Healthcare Improvement that is intended to optimize health system performance. Its three tenets include improving the patient experience, improving population health and reducing the per capita cost of healthcare. cognizant 20-20 insights Non-adherence increases the cost burden on all major stakeholders in the healthcare system, as the resulting health declines can require utilization of more expensive services, such as those found in the acute or long-term care system. This creates a vicious cycle of deteriorating health outcomes and increasing healthcare costs. For instance, non-adherance amounts to $289 billion in annual wasted costs in the U.S. alone.8 Aditionally: • Payers’ and providers’ losses due to increased hospital readmission for medicare patients is $26 billion per decade.9 • The average cost of non-adherence for adult patients diagnosed with diabetes, hypertension and dyslipidemia is $453 per adult.10 Non-adherence leads to One school of thought deteriorating health outpostulates that instead comes across patient types. In a study of of spending billions on mortality rates in dia- creating new medications betes and heart disease to cure chronic diseases, patients, non-adherers had much higher mortal- applying a fraction of ity rates (12.1%) compared that cost to helping with adherers (6.7%).11 patients adhere to their Non-adherence due to communication inef- medications would have ficiencies among care a more significant impact providers in U.S. hospitals on the health of the costs approximately $12 12 billion per annum. One population as a whole. school of thought postulates that instead of spending billions of dollars on creating new medications to cure chronic diseases, applying a fraction of that cost to helping patients adhere to their medications would actually have a much more significant impact on the healthcare system and the health of the population as a whole. 2 Plummeting Adherence Levels Across Therapeutic Areas Over Time 60 50 60% 52% 53% 48% 43% Adherence Rates (%) 47% 40 30 Cholesterol 41% 38% 41% 34% Diabetes (type 2) 35% 30% Obesity 20% 20 Hypertension 10 Depression 10% 8% 0 3 months 6 months 12 months * Adherence rates were averaged. Source: Various sources; A. T. Kearney analysis Figure 1 Traditional Management of Non-adherence Conventional health models have historically placed patients with different health conditions into distinct disease management programs. The traditional approach of designing programs that address individual adherence barriers has resulted in extremely siloed health management programs. These programs are less effective because they don’t account for the fact that nonadherence is caused by the presence of multiple factors.13 Studies reveal that many patients stop taking their medication, and adherence rates plummet, in just a few months, with 50% to 90% of patients stopping their prescribed therapies by the end of the first year of treatment (see Figure 1).14 Individual adherence solutions, such as patient education, pharmacy programs, awareness campaigns and financial rewards, can impact adherence in certain situations, but a “one-sizefits-all” approach is not effective; one-tool solutions often become marginalized if the program does not address the underlying barriers of adherence. Understanding the Causes of Non-Adherence The reasons for patient non-adherence are complex and multifactorial, and an effective coordinated care model needs to consider all of the underlying causes. Both internal factors (a patient’s intentional and unintentional beliefs) and external factors (those related to the healthcare system, family support, the therapy regimen, the condition itself and socioeconomic factors) can influence whether a patient follows the prescribed healthcare advice. All of these factors have a powerful influence on patient decisionmaking and behavioral change. Quick Fact The Health Belief Model proposes that patients act on treatment recommendations when they believe that the benefits of treatment outweigh treatment barriers. cognizant 20-20 insights 3 Quick Fact Patient adherence budgets for U.S. pharmaceuticals companies have jumped 281% from $400,000 in 2009 to $1.5 million in 2012. In a study of 18 small, medium and large pharmaceuticals companies, 12 had dedicated patient adherence teams. Human health behavior professionals, who can better understand patients’ motivations, psychology and emotions are increasingly a part of these teams.17 Some studies have found that several features of the therapeutic regimen are correlated with adherence. For example, the more the patient must change his or her lifestyle, the less likely he or she is to follow recommendations. In addition, the less complicated the treatment regimen, the higher the rate of adherence. Pharmaceuticals companies have more recently ventured into adherence management, in the interest of preventing patients from switching to competitive offerings, influencing positive health outcomes and reducing the overall cost of healthcare by offering a set of adherence services along with their product. The Emerging Adherence Paradigm of Patient Centricity Acquiring new patients costs pharmaceuticals companies an average of 62% more than retaining the ones they already serve.16 Since pharmaceuticals companies have limited interaction with patients The more the compared with healthcare providers and payers, they patient must change sometimes work collab- his or her lifestyle, oratively with ACOs and the less likely he payers to reduce the cost of therapies and improve or she is to follow outcomes. However, sever- recommendations. al major pharmaceuticals In addition, the less companies are now working to engage with patients complicated the directly. treatment regimen, In the patient-centric model, patients are empowered to participate in their own care alternatives, and healthcare providers are there to support patients and engage in joint decision-making based on individual patient situations. This new model also places greater emphasis on leveraging healthcare technologies to engage patients in the management of their own healthcare spending by encouraging them to pursue healthier choices and lifestyles that can help contain longterm medical costs. Approximately 69% of total healthcare costs are heavily influenced by consumer behaviors.15 Thus, in the new patient-focused paradigm, the basic driver is to get patients to change their behavior by making healthier choices and seeking appropriate preventive and primary care to manage their health conditions. What Patient Centricity Means for Various Stakeholders Today’s healthcare environment has led hospitals, physician groups and payers to develop accountable care organizations (ACOs), which are designed to slow spending growth and improve care quality. Each of these stakeholders (payers, providers, ACOs, pharma companies) has a role to play in increasing patient adherence. Traditionally, providers have educated patients on adherence. However, payers are increasingly working to ensure their members have better health outcomes and lower costs. ACOs are also heavily incentivized to manage overall patient health, making adherence an important factor for them. cognizant 20-20 insights the higher the rate An example is the active collaboration between of adherence. Medco Health (a pharmacy benefit manager) and Sanofi (a leading global pharma company). Working together, these companies launched a head-to-head clinical trial of Plavix (clopidogrel) and Effient (prasugrel) that highlighted not just which molecule is more efficacious but also which patients would be best suited to which drug. Plavix showed poor efficacy in 25% of patients, who might respond better to Effient; however, the other 75% could therapeutically benefit from the generic version of Plavix and thus reduce their treatment costs. Such collaborative approaches will demonstrate the value of determining appropriate treatment pathways for a particular condition rather than just randomly assessing the efficacy of individual drugs in a sample representing all patients.18 4 Three-Pronged Approach to a Coordinated Care System TECHNOLOGY Personal instrumentation (BYOhD) BEHAVIOR CHANGE Social, gamification, analytics CONNECT Virtual and human health coaches • Improved Health Outcomes • Lower Costs • Enhanced Experience Figure 2 Achieving a Patient-centric Approach To develop a collaborative and patient-centric accountable care system, stakeholders need to adopt a three-pronged approach that combines pure technology tools, behavioral modification and a connected health ecosystem (see Figure 2). Devices and sensors can increase self-monitoring and management; gamification and analytics techniques can be used to identify and engage patients and bring about behavior change; and a well-developed IT infrastructure can help connect various stakeholders in the healthcare ecosystem — physicians, paramedic staff, care providers, payers, pharmaceuticals companies, pharmacies and health coaches — whose support is necessary to develop an all-inclusive integrated support system for the patient. An Adherence Framework To address the issue of medication non-adherence, we have developed a patient-centric model that is sensitive to patient needs and wants. An effective adherence model must use a holistic patient engagement framework that is designed to address the causes of non-adherence from a patient’s point of view. Understanding the Patient Journey and Identifying Moments of Truth Developing a patient-centric adherence framework starts with understanding the patient’s beliefs and motivation levels throughout the care journey. For any disease state, patients progress through different stages, including diagnosis, treatment and care. Patients also experience several “moments of truth:” They want to be heard, receive feedback on their progress and share their experiences. All of these interactions need to be seamless so that patients can focus on their care rather than being caught in a web of interaction challenges. To resolve these challenges, key ecosystem players must leverage the many sources of rich data available to them, as well as the latest technologies to collect and analyze this data. We call this the “5 C’s”: collect data, capture events, connect stakeholders, compress time and create opportunities. Patient-centric Adherence Framework Patient interactions within the healthcare ecosystem are exceedingly complex; therefore, a holistic medication adherence framework is needed to facilitate critical interactions with and collabo- Quick Fact The collaboration of multiple stakeholders (physicians, nurses, pharmacists and payers) is essential for patient adherence, especially to prescription medications, as well as increasing patient-centricity. With physicians and pharmacists involved in the patient recruitment cycle, organizations can expect a jump in program enrollments in the range of 17% to 36% based on regions and disease type.19 cognizant 20-20 insights 5 An Approach for Monitoring Patient Adherence allows for the fact that each patient enters the care cycle with different beliefs and motivation levels (see Figure 3). Framework considerations should include: Patient enters with specific beliefs and motivations. • Patient stratification: Patients need to be categorized in different ways, and customized engagement programs need to be designed for the different segments. Different adherence methods are applicable to different situations, depending on the type of adherence being assessed, the precision required and the intended application of the results. As there is no “gold standard” for measuring patients’ adherence to medicines, and no single tool to detect all types of non-adherence, the choice of method for measuring adherence to a medication regimen should be based on its usefulness and reliability for a particular patient profile, therapeutic area, drug under consideration, etc. • Data collection: Data received from predictive surveys and past behavior (self-reported, “quantify-me” device data, EHR integration) can be used to segment patients into different strata (see Figure 4). Patients should be able to use their own health devices and smartphones to measure, integrate and track their health data; we call this a BYOhD platform (or “bring your own healthcare device”). Such a platform provides the flexibility to capture patient Patient stratification Outcome monitoring Intelligent interventions Delivering insights to patients Self-help and education Figure 3 ration among various stakeholders. The guiding principle for such a framework is enabling patient engagement to improve health outcomes. An effective patient-centric adherence framework Adherence Assessment Methods DIRECT INDIRECT Direct Observation Behavior/Physiological Markers Assessment Measurement of Biological Markers Figure 4 Secondary Data Self Reporting Data Collection • Surveys • Interviews • Patient diaries Assessment • General scales (e.g., Morisky, MARS) • Therapy-specific (e.g., Hill-Bone Compliance Scale for hypertensive patients) cognizant 20-20 insights 6 Data Collection • Rx refill data • Claims data Assessment Parameters • Drug adherence index • Medication possession ratio • Proportion days covered Electronic Monitoring “Gold Standard” of Adherence Assessment • BYOhD-based self-monitoring devices (e.g., smartphone apps, Fitbit, etc.) • E-pills Industry-Approved Predictive Surveys Illustrative List of Validated Predictive Surveys Scale Name Description ASRQ Scale (Adherence Self Report Questionnaire) Outpatients taking anti-hypertensive ARMS (Adherence to Refills and Medication Scale) Patients with coronary heart disease / hypertension Brooks Medication Adherence Scale Adults with asthma Composite Self Report Measure Homecare patients over 65 years of age MAQ (Medication Adherence Questionnaire) Used across populations Shortest scale MARS (Medication Adherence Rating Scale) Psychiatric disorders Morisky 4 and Morisky 8 Across populations BMQ (Brief Medication Questionnaire) Patients with hypertension, diabetes mellitus, hypercholesterolemia, hypothyroidism or condition requiring HRT SEAMS (Self-efficacy for Appropriate Medication Use) Low-literacy patients VAS (Visual Analogue Scale) Across populations Figure 5 surveys, health providers can obtain deep insights into patient behavior. Advanced analytics techniques, such as causal networks and group-based therapy modeling, can be applied to this data to further help organizations segment patients based on behavioral patterns and their risk of non-adherence, which in turn helps to develop better intervention strategies designed to improve adherence. data across different systems and channels to develop a unique virtual identity, or Code Halo.TM 20 Metadata from a patient’s Code Halo (i.e., diagnostic codes, treatments, elements of the electronic medical record, etc.) can be used to create a profile within a particular segment to help personally manage the patient’s wellness. Predictive surveys are questionnaires supplied to patients that can help predict their behavior and enable segmentation. A list of industryapproved predictive surveys is presented in Figure 5. • Self-help and education: Enabling patients with self-help tools and an understanding of their condition is critical to helping them manage and maintain wellness. While most medical literature is written at a college (14thgrade) level, patient education should be made By using the “big data” created and leveraged by BYOhD platforms and predictive Quick Fact Pharmaceuticals companies Boehringer Ingelheim and Eli Lilly launched the largest ever global survey to investigate early Type 2 diabetes. The study was conducted in partnership with the International Diabetes Federation in December 2013 and involved more than 10,000 people with Type 2 diabetes and more than 6,500 treating physicians from 26 countries. The intent was to investigate how early conversations between physicians and patients with Type 2 diabetes could be optimized. Insights from the survey will be used to develop solutions to support primary care physicians and people with Type 2 diabetes. cognizant 20-20 insights 7 Quick Fact Pharmaceuticals companies are increasingly using gamification to engage patients to improve adherence and outcomes. Merck, for example, developed a game called the “Type 2 Travelers Project” to encourage patients to follow the treatment regimen of its diabetes drug Januvia, as well as manage other aspects of their health. them to review the progress of patients’ selfmanagement and predict behavior patterns in order to identify high-risk patients who are likely to stop engaging and design intervention models to motivate them. By analyzing the patient’s Code Halo, organizations can not only predict non-adherence among high-risk patients but also correlate how multiple events are interconnected, and then share these insights with patients to help them embrace healthier habits. more engaging by simplifying medical and clinical content to a fifth-grade level. Emerging technologies and tools enable effective education delivery to patients, including: >> Collaboration tools among healthcare providers (HCP), caregivers and patients. >> Multiple access mechanisms such as Web portals and mobile devices (BYOhD). >> Multichannel communications (SMS, email and IVR) that enable patients to use their channel of choice. For example, a diabetic patient who experiences a hypoglycemic attack may discover that the episode is correlated to poor diet and medication non-adherence, perhaps as a result of an underlying attitude that the patient has toward the drug. Correlating this information and developing an effective intervention using an analytics engine can help providers deliver insights to patients that encourage them to change their behaviors. Strong analytical and segmentation capabilities are also important for tracking and understanding changes in adherence levels and behavior patterns over time. As patients change, organizations must map them to new segments and design new interventions. >> Gamification techniques to increase engagement and adoption. Pharmaceuticals companies often use interactive games and other reward systems within their mobile initiatives to keep patients engaged with their healthcare. While self-reporting data is essential to tracking and measuring patient outcomes and behaviors, self-reporting rates are usually very poor due to low patient motivation levels. Gamification can provide a driving force for patients to involve themselves in the process and benefit from it. >> Use of social media such as Facebook and Twitter to create forums and user communities. • Delivering insights to patients: Health providers need to develop analytics that enable Quick Fact When a U.S.-based PBM wanted to optimize expense management on therapy adherence programs, it set a goal of offering the “right” programs to the “right” members. The PBM used a statistical predictive model to predict member adherence behavior and deployed different retention strategies for patients on the basis of observed behavior patterns. The improved targeting resulted in high rates of adherence for diabetes/lipids therapies and a high ROI for the adherence programs. cognizant 20-20 insights 8 • • Providing intelligent interventions: Actively engaging patients with self-help tools for health management can be achieved through captology21 concepts, in which virtual coaches deliver alerts, notifications and motivational messages to drive positive behavior change. If virtual health coaches do not significantly impact positive behavior change, real health coaches can intervene to offer a human element. Outcome monitoring: It is critical for organizations to understand the impact of active interventions on the health and well-being of patients. Tracking which interventions are effective and revising the ones that aren’t is critical to properly monitoring outcomes. The B.J. Fogg model helps to deliver small behavioral changes that eventually drive large behavioral change in patients.23 Personalized delivery of these interventions can be achieved by building AI-based causal models that increase understanding of the causes of the current behavior and target the right areas for intervention. Reusable models such as the Health Action Process Approach (HAPA) can also help explain causality in health behavior.24 Just as it is important to influence outcomes, it is equally important to track the ROI of patient segments to make adherence monitoring programs financially viable. Identifying “high-value” patients and revising rewards mechanisms to meet their needs is an equally important component. Measuring ROI of Adherence Programs Adherence can be an important area of focus for pharmaceuticals companies, payers and providers to maximize their ROI. An inherent problem with adherence programs is the difficulty of obtaining and demonstrating ROI. Recent studies document the multiple issues that complicate the determination of financial ROI: • The lack of a standard approach for reporting costs. • The “healthy user” effect: Short-term studies tend to yield highly positive results. The type of patients who voluntarily enroll in a study and actually follow the experimental regimen is not typically representative of the general population. Participants can be expected, on average, to be healthier, as they are concerned about their health and are predisposed to follow medical advice, both factors that would aid one’s health. • Time preference trade-off: Stakeholders may be willing to trade short-term increases in medication costs and complementary goods and services for long-term savings or health gains. • The time required to attain ROI differs across stakeholders: Increased medication adherance might result in an instantaneous ROI for pharmaceuticals companies, but adherence over a longer timeframe is required for patients to observe a reduction in their disease-related health costs. Quick Fact Health coaching can improve lifestyle behaviors known to prevent or manage chronic conditions. A study conducted by AtlantiCare, a large not-for-profit healthcare system in New Jersey, suggests that the involvement of primary care physician and health coach teams can improve outcomes and reduce costs for complex patients. The study found that improvements in self-management behaviors and clinical outcomes led to lower utilization, a significant slowdown in the annual rate of cost increases and markedly higher levels of patient satisfaction. Patients enrolled in the program reported much higher levels of satisfaction compared with their previous experience, with gains of 30 to 40 percentage points on questions related to access and timeliness of care, respect for the patient, time spent with the provider, communication and coordination of care between the primary care team and specialists.22 cognizant 20-20 insights 9 Adherence Studies Included in Meta-analysis Study Research Author Year Sample Disease Study 1 Costs of Chronic Disease Sokol 2005 15,085 Diabetes Hypertension Hypercholesterolemia CHF Study 2 CVS Caremark and CSM Roebuck MC 2010 135,008 CHF Diabetes Hypertension Study 3 Blood Pressure Reduction, Persistence and Costs in the Evaluation of Hypertension Bramlage P 2009 7,981 Hypertension Figure 6 An ROI framework should take into account common measures, such as annual medication costs, direct medical costs and total healthcare costs, as well as the savings associated with each. An ROI calculation can be performed using the following formula: Financial Outcomes Resulting from Increased Medication Adherence We conducted a meta-analysis of a sampling of studies related to adherence. The mean, median, standard deviation, minimum observed value and maximum observed value were calculated for total healthcare savings, total medical savings and increased pharmaceuticals revenue (see Figure 6). The cost-related benefits of proper medication adherence included a mean increase in pharmaceuticals revenue of $1,129; a mean medical cost Rx Revenue / (Medical Costs + Pharmacy Costs + Intervention Costs) = ROI Meta-Analysis of Adherence Studies Covering Cost-Related Benefits of Medication Adherence Study 2 Study 3 Mean Total medical cost >80% adherent Total medical cost <79% adherent Total medical savings Rx costs >80% adherent Rx costs <79% adherent Increased Rx revenue Total health cost savings / increased drug cost ROI Total healthcare savings Study 1 Prescription revenue Total healthcare savings <79% adherent Study Total medical cost Total healthcare cost >80% adherent Total healthcare cost Diabetes 8,886 16,498 7,612 6,377 15,186 8,809 2,510 1,312 1,198 6.4 Hypertension 8,386 9,747 1361 6,570 8,831 2,261 1,817 916 901 1.5 Hypercholestrolemia CHF 6,752 10,916 4,164 4,780 9,849 5,069 1,972 1,067 905 4.6 22,164 23,964 1,800 19,056 22,003 2,947 3,107 1,961 1,146 1.6 CHF 37,762 45,823 8,061 33,113 42,549 9,436 4,649 3,274 1,375 5.9 Disease Diabetes 19,311 21,116 1,805 14,725 18,501 3,776 4,586 2,615 1,971 0.9 Hypertension 14,292 19,006 4,714 11,041 16,835 5,794 3,251 2,171 1,080 4.4 Hypertension 4,871 6,062 1,191 6,570 10,286 3,716 489 31 458 2.6 $1,668 $1,129 3.5 $15,303 $19,142 $3,839 $12,779 $18,005 $5,226 $2,798 Figure 7 cognizant 20-20 insights 10 savings of $5,226; a mean total healthcare savings of $3,413; and a mean ROI of 3.5 (i.e., every additional dollar spent on medicines by highadherence patients resulted in $3.50 in savings on total healthcare-related costs). The maximum adherence-related ROI was observed in diabetes, followed by congestive heart failure), hypertension and hyper-cholesterolemia (see Figure 7, previous page). A wide range of cost offsets and healthcare savings for patients demonstrating adherence to medications across chronic conditions are often observed. • A collaborative patient-centric approach. • A solid foundation of cutting-edge technology, such as BYOhD, gamification and analytics. • Customizable, scalable services for patients. and sustainable • Multi-channel capabilities and multi-modal messaging to facilitate personalized patient communications. • Live health coaches to support and augment virtual interventions to bring about behavior change. • Strong governance and capabilities to integrate and support the entire value chain across geographies. Looking Forward Medication adherence programs offer a vast potential for reducing healthcare costs and improving health outcomes. However, the design and implementation of an adherence program that engages patients and results in sustainable change requires both expertise and experience to determine which behavioral factors are relevant in each therapeutic area and for each brand. When designing an adherence program, organizations need to ensure a focus on: Patient-centered care is about enhancing the patient experience. It enables players across the healthcare landscape to better meet patients’ needs by respecting their time, informing them, understanding them as individuals, answering their questions, connecting them with their data — and their ecosystem — and allowing caregivers to actively participate in patient well-being. Footnotes 1 “Global Burden of Chronic Disease,” World Health Organization, http://www.who.int/nutrition/topics/ 2_background/en/. 2 “A Universal Truth: No Health without a Workforce,” Global Health Workforce Alliance and World Health Organization, November 2013, http://www.who.int/workforcealliance/knowledge/resources/ hrhreport2013/en/. 3 “National Health Expenditure Projections,” Centers for Medicare & Medicaid Services, 2011-2012, http://www.cms.gov/Research-Statistics-data-and-Systems/Statistics-Trends-and-Reports/ NationalHealthExpendData/Downloads/Proj2011PDF.pdf. 4 “Home Care Providers in the U.S.: Market Research Report,” IBIS World, September 2014, http://www.ibisworld.com/industry/default.aspx?indid=1579. 5 Bobbi Coluni, “Save $36 Billion in U.S. Healthcare Spending through Price Transparency,” Thomson Reuters, February 2012, http://www.hreonline.com/pdfs/06022012Extra_ThomsonReutersStudy.pdf. 6 “Mobile Health Trends and Figures 2013-2017,” Research2Guidance, http://www.research2guidance.com/ shop/index.php/mobile-health-trends-and-figures-2013-2017. 7 “Value Added Services Report,” Eyeforpharma, Sept. 16, 2013, http://www.eyeforpharma.com/ value-added-services-report/?utm_source=PR+WEB&utm_medium=External+website&utm_ content=press+release&utm_campaign=2445. 8 “Interventions to Improve Adherence to Self-administered Medications for Chronic Diseases in the U.S.,” Annals of Internal Medicine, Dec. 4, 2012, http://www.ncbi.nlm.nih.gov/pubmed/22964778. 9 Jordan Rau, “Medicare Prepares Rule to Penalize Hospitals with High Readmission Rates,” Kaiser Health News, July 30, 2011, http://www.kaiserhealthnews.org/stories/2011/july/30/medicare-and-hospital-readmissions.aspx. cognizant 20-20 insights 11 10 Kamyar Nasseh, Sharon Glave Frazee, Jay Visaria, Anna Vlahiotis and Yuhong Tian, “Cost of Medication Nonadherence Associated With Diabetes, Hypertension, and Dyslipidemia,” American Journal of Managed Care, March 29, 2012, http://www.ajmc.com/publications/ajpb/2012/AJPB_MarApr2012/ Cost-of-Medication-Nonadherence-Associated-With-Diabetes-Hypertension-and-Dyslipidemia. 11 “The Role of Medication Adherence in the U.S. Healthcare System,” Avalere Health, June 2013, http:// static.correofarmaceutico.com/docs/2013/06/24/adher.pdf. 12 R. Agarwal, D. Z. Sands and J. D. Schneider, “Quantifying the Economic Impact of Communication Inefficiencies in U.S. Hospitals” Journal of Healthcare, July-August 2010 , Vol. 55, No. 4, pp 265-81. 13 “Patient Adherence: The Next Frontier in Patient Care,” Capgemini, 2011, http://www.pt.capgemini.com/ resource-file-access/resource/pdf/Patient_Adherence__The_Next_Frontier_in_Patient_Care.pdf. 14 Various sources; A.T. Kearney analysis. 15 “Medication Adherence: Managing for Total Value,” The Foundation for Managed Care Pharmacy, 2011, http://amcp.org/uploadedFiles/FMCP/Resources/FMCP_Adherence_Slides.pdf. 16 “Patient Adherence: The Next Frontier in Patient Care,” Capgemini, 2011 http://www.pt.capgemini.com/ resource-file-access/resource/pdf/Patient_Adherence__The_Next_Frontier_in_Patient_Care.pdf. 17 Stephanie Baum, “Pharma Patient Adherence Budgets Have Increased 281 Percent in Four Years,” Medcity News, Oct. 12, 2012, http://medcitynews.com/2012/10/pharma-patient-adherence-budgetshave-increased-281-percent-in-four-years/. 18 Warren K. Williams, “Key PBM Functional Areas Require Radical Transformation,” Managed Care, August 2012, http://www.managedcaremag.com/archives/1208/1208.pbm-functions.html. 19 Sundiatu Dixon Fyle, Shonu Gandhi, Thomas Pellathy and Angela Spatharou, “Changing Patient Behavior: The Next Frontier in Healthcare Value,” McKinsey & Co., 2012, http://www.google.co.in/url?sa=t&rct=j&q= &esrc=s&frm=1&source=web&cd=1&ved=0CC0QFjAA&url=http%3A%2F%2Fwww.mckinsey.com%2F~% 2Fmedia%2Fmckinsey%2Fdotcom%2Fclient_service%2FHealthcare%2520Systems%2520and%2520 Services%2FHealth%2520International%2FIssue%252012%2520PDFs%2FHI12_64-73%2520PatientB ehavior_R8.ashx&ei=Uj1hUoqNHsnsrAe7qoGwCg&usg=AFQjCNFa25xhB96amLMHyfqc3xp9xVH7NA&bv m=bv.54934254,d.bmk. 20 For more on Code Halos, read “Code Rules: A Playbook for Managing at the Crossroads,” Cognizant Technology Solutions, June 2013, http://www.cognizant.com/Futureofwork/Documents/code-rules.pdf, and the book, “Code Halos: How the Digital Lives of People, Things, and Organizations are Changing the Rules of Business,” by Malcolm Frank, Paul Roehrig and Ben Pring, published by John Wiley & Sons. April 2014, http://www.wiley.com/WileyCDA/WileyTitle/productCd-1118862074.html. 21 Captology is the study of computers as persuasive technologies. This includes the design, research and analysis of interactive computing products (computers, mobile phones, Web sites, wireless technologies, mobile applications, video games, etc.) created for the purpose of changing people’s attitudes or behaviors. B. J. Fogg derived the term “captology” in 1996 from an acronym: Computers as Persuasive Technologies, or CAPT. Source: Stanford Persuasive Tech Lab. 22 “Primary Care Physician and Health Coach Teams Improve Outcomes and Reduce Costs for Complex Patients,” Agency for Healthcare Research & Quality, http://search.ahrq.gov/search?q=cache:he gBt4Z85noJ:innovations.ahrq.gov/content.aspx%3Fid%3D2941+health+coach&output=xml_no_ dtd&proxystylesheet=AHRQ_GOV&client=AHRQ_GOV&site=default_collection&access=p&ie=UTF8&oe=UTF-8. 23 B. J. Fogg’s Behavior Model shows that three elements must converge at the same moment for a behavior to occur: motivation, ability and trigger. When a behavior does not occur, at least one of those three elements is missing. Fogg founded the Persuasive Technology Lab at Stanford University, where he directs research and design. In addition, he devotes at least half his time to industry projects and innovations, all of which focus on using technology to change behaviors in positive ways. For more information, see “B. J. Fogg’s Behavior Model,” http://www.behaviormodel.org/. 24 The health action process approach (HAPA) is a psychological theory of health behavior change. It was developed by Ralf Schwarzer, professor of Psychology at the Free University of Berlin in Germany. HAPA is an open framework of various motivational and volitional constructs that are assumed to explain and predict individual changes in health behaviors such as quitting smoking or drinking, and improving physical activity levels. For more information, see “The Health Action Process Approach,” http://web.fu-berlin. de/gesund/publicat/ehps_cd/health/hapa.htm. cognizant 20-20 insights 12 About the Authors Nagaraja Srivatsan has more than 25 years of experience in the information technology industry and deep knowledge of the healthcare and life sciences domain. Currently, he is part of Cognizant’s Emerging Business Accelerator (EBA) leadership team. In this role, he identifies, incubates and grows innovative and transformational ventures for new markets, platforms and solutions within the healthcare and life sciences industry. In addition, he is the venture partner guiding Cognizant’s efforts to penetrate the government and energy-utilities sectors, globally. Siva Thiagarajan is a team member of Cognizant’s patient engagement solutions team within its Life Sciences Business unit. He has 18 years of experience in life sciences across the pharmaceuticals, biotech and medical device sectors and has worked across the business consulting, technology and business process services spaces, leading consulting engagements in the area of patient engagement. Siva earned an M.B.A. from Columbia University. Suresh Ganesan is an Associate Vice-President at Cognizant and heads the company’s Solutions Architecture & Technology Practice within the Life Sciences and Healthcare Business Unit. He is also CTO of Cognizant’s connected health, patient engagement and BYOhD ventures within the EBA organization. He holds a master’s degree in computer science from Indian Institute of Science, Bangalore, India. Arvind Kumar is a Manager and a subject matter expert within Cognizant’s patient engagement ventures, working to incubate innovative and transformational businesses for Cognizant’s healthcare and life sciences customers. Arvind holds a master’s of business administration in marketing and in bioinformatics and completed a graduate degree in biotechnology. Shweta Seth is a Business Analyst and a subject matter expert in Cognizant’s patient engagement ventures. She has played a pivotal role in the development of Cognizant’s patient engagement platform. She works closely with venture leads and currently supports the go-to-market team in its business development activities. Shweta is a pharmacist and has received education in pharmaceuticals marketing. Dr. Elby Nash is a Solutions Partner with Cognizant's Life Sciences Solutions Architecture & Technology (SAT) practice. Dr. Nash has been a senior management consultant, executive and technology innovation leader in the pharmaceuticals, medical device and other industries for over 30 years. He is an expert on mobile technology, connected health and the deployment of wireless and mobile technologies to drive business differentiation and productivity. For more information, contact us at [email protected]. About Cognizant Cognizant (NASDAQ: CTSH) is a leading provider of information technology, consulting, and business process outsourcing services, dedicated to helping the world’s leading companies build stronger businesses. Headquartered in Teaneck, New Jersey (U.S.), Cognizant combines a passion for client satisfaction, technology innovation, deep industry and business process expertise, and a global, collaborative workforce that embodies the future of work. With over 75 development and delivery centers worldwide and approximately 187,400 employees as of June 30, 2014, Cognizant is a member of the NASDAQ-100, the S&P 500, the Forbes Global 2000, and the Fortune 500 and is ranked among the top performing and fastest growing companies in the world. Visit us online at www.cognizant.com or follow us on Twitter: Cognizant. World Headquarters European Headquarters India Operations Headquarters 500 Frank W. Burr Blvd. Teaneck, NJ 07666 USA Phone: +1 201 801 0233 Fax: +1 201 801 0243 Toll Free: +1 888 937 3277 Email: [email protected] 1 Kingdom Street Paddington Central London W2 6BD Phone: +44 (0) 20 7297 7600 Fax: +44 (0) 20 7121 0102 Email: [email protected] #5/535, Old Mahabalipuram Road Okkiyam Pettai, Thoraipakkam Chennai, 600 096 India Phone: +91 (0) 44 4209 6000 Fax: +91 (0) 44 4209 6060 Email: [email protected] © Copyright 2014, Cognizant. All rights reserved. No part of this document may be reproduced, stored in a retrieval system, transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the express written permission from Cognizant. The information contained herein is subject to change without notice. All other trademarks mentioned herein are the property of their respective owners.