Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
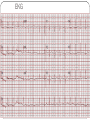
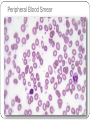
LSU INTERNAL MEDICINE CASE CONFERENCE CASE CONFERENCE APRIL 17th 2012 Raisa C. Martínez, M.D. Neurology PGY-1 Chief Complaint “My chest hurts and I’ve been having trouble breathing.” History of Present Illness This is a 46-year-old woman with PMHx of vitiligo, endometriosis, and irritable bowel syndrome, who was in her usual state of health until 2 months prior to admission when she started feeling short of breath, tired and weak. The patient does report one episode of feeling light headed about 2 months ago in Atlanta while walking her dog. She thought that she was going to pass out but did not lose consciousness. Following this episode she went to the ED where a work-up failed to explain her symptoms. She moved to New Orleans about one month prior to admission. Her symptoms continued to worsen She also began to experience intermittent chest pain and shortness of breath that was more pronounced with exertion. Worsening of these symptoms prompted the patient to present to the emergency department. HPI (continued)… She described her chest pain as: left sided in location; 6-7/10 in intensity; radiated to the neck and left arm; and associated with shortness breath, nausea, diaphoresis. She also described an uncomfortable sensation pressing against her left collar bone. Always tired…. Denied fever, chills, or cough. No headache. No hemoptysis or gum bleeding. No vaginal bleeding. No dark tarry stools or blood in her stool. She has noticed that the white of her eyes have become yellow. Past Medical History Endometriosis Vitiligo Chronic pelvic pain Irritable bowel disease after bowel resection Medications: None Allergies None Past Surgical History Ectopic pregnancy resection Chocolate cyst removal x 2 Partial hysterectomy secondary to endometriosis Ex-lap with lysis of adhesion secondary to prior abdominal procedures as well as resection of a portion of bowel. The location is unknown to the patient (as per the patient about 8 cms of length of her bowel was removed). Family History Non-contributory Social History One pack of cigarettes weekly x 15 years Occasional alcohol. Occasional marijuana use Regular diet Review of Systems: (+) Gen: Decreased energy, feeling listless, decreased appetite, unintentional weight loss, lightheadedness CV: chest pain, syncope, diaphoresis Pulm: Progressive worsening shortness of breath x 2 months, especially upon exertion x 2 weeks, wheezing Endocrine: Increased desire for ice cold water, but no pica GI: Nausea and emesis, alternating diarrhea and constipation GU: Increased frequency with irritation upon urinating Neuro: Generalized weakness without focal deficits Heme: No easy bruising, soft tissue infections or edema Review of Systems: (-) Gen: No fevers, chills or night sweats, no jaundice Eyes: No changes in vision, no photophobia ENT: No dysphagia, epistaxis or tinnitus CV: No palpitations Pulm: No cough with or without sputum, no paroxysmal nocturnal dyspnea, no orthopnea GI: No abdominal pain or distension, no changes in stool color or caliber GU: No dysuria, no flank pain, no hematuria or vaginal discharge Neuro: No seizures, tremors or recurrent headaches Heme: No easy bruising, soft tissue infections or edema Physical Exam: VITAL SIGNS: BP-118/84 HR-103 Temp- 98.3 O2 sats on RA-98% GENERAL: AAO x3. No apparent distress. HEENT: Positive minimal scleral icterus, and in the soft palate and hypoglossal fossa as well No appreciated thyromegaly or cervical lymphadenopathy. No paranasal tenderness. No oropharyngeal erythema or exudate. Moist mucous membranes. Positive skin change and vitiligo to the face. PERRL. EOMI CARDIOVASCULAR: Regular rate and rhythm. S1, S2 normal. No murmurs,rubs, or gallops appreciated on auscultation. RESPIRATORY: Clear to auscultation bilaterally. No wheezes, rales, or crackles appreciated. Physical Exam (continued)… ABDOMEN: Nondistended. Positive bowel sounds. No hepatosplenomegaly appreciated; nontender to palpation. EXTREMITIES: No cyanosis, clubbing, or edema. 2+ pulses x4 extremities. Poor capillary refill with resting pallor, positive vitiliginous changes to the bilateral upper extremities and lower extremities with islands of amelanotic patches surrounded by hyperpigmented areas. No rashes, no petechiae. Physical Exam (continued)… Chest X-ray EKG Laboratory Work Up… 10 140 103 10 3.4 26 0.39 Mg = 1.8 N = 3.0 82 L = 2.7 6.9 5.9 M = 0.1 Peripheral Smear: 32.8 + tear drop cell 20.7 E = 0.1 Phos = 5.1 97.8 99 RBC = 2.12 MCH = 32.4 B=0 • Amylase = 19 • Lipase = 25 44 + schistocytes Hypochromic Polychromasia Tpro Alb Tbili AST AlkP ALT 7.4 4.9 3.2 154 Microcytes, macrocytes Decreased platelets 77 11.6 • Hep Panel = (-) • U/A: 1.008/7.0/+nitrites/+leukocytes/ many bacteria, 3-5 wbc, 2-20 squam, 0 casts 21.1 1.0 D-dimer = 5640 Trop #1 = 0.03 LDH = 2730 Trop #2 = 0.03 Haptoglobin = 7 Retic % = 0.8 More laboratory work-up… Iron Profile: Iron = 132 Transferrin = 238 TIBC = 309 Iron Sat = 43 • Vit B 12 = <12 • Ferritin = 177.5 • Folate = 15.8 • TSH = 1.45 • ANA = (-) • Methylmalonic acid = 1363 • Homocysteine = 45 Chest CT Angiogram 1. No evidence of intra-arterial pulmonary thrombus. 2. No pulmonary mass, pneumothorax, pleural effusion, or lymphadenopathy 3. Mild cardiomegaly. Abdominal U/S Hepatomegaly. Heterogeneous hepatic echotexture. This limits evaluation of the underlying hepatic parenchyma and therefore detection of focal abnormality. Further evaluation with contrast-enhanced MRI or CT can be performed as clinically warranted. The SPLEEN is normal in size and appearance , measuring 11-12 cm. The left KIDNEY is normal borderline size measuring 13.1 cm. thickness of the parenchyma is normal. No stones are seen. There is no evidence of hydronephrosis. No significant solid masses are noted. Peripheral Blood Smear Additional lab data Celiac Sprue = (-) Electrophoresis = Normal A = 95% A2 = 2.3% Intrinsic Factor AB = (+) Hospital Course Day: 1-2 Blood Transfusion x 2 with appropriate response Hematology/Oncology Consult Vit B12 dose given Diagnosis… Vitamin B-12 Deficiency secondary to Pernicious Anemia Follow-Up… Patient received Vit B12 for 1-1/2 months At present time the patient’s vitamin B12 levels are within normal limits. The patient will require vitamin B12 for the rest of her life and should take 1000 mcg of vitamin B12 subcutaneously every month THANK YOU