Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
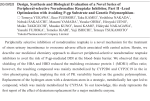
Clinical Science ( 1980) 58,3743 Sequential changes in plasma noradrenaline during bicycle exercise R . D. S. W A T S O N , C . A. H A M I L T O N , D . H . J O N E S , J . L. REID,’ T. J . S T A L L A R D A N D W. A. L I T T L E R Department of Cardiovascular Medicine, University of Birmingham and East Birmingham Hospital. and Department of Clinical Phormocology. Royal Postgraduate Medical School. Hammersmith Hospital. London (Received 11 January 1979; accepted 20June 1979) Summary vascular system. We have examined how plasma noradrenaline changes during and after bicycle exercise in both the supine and upright positions in order to determine the relationship of changes in sympathetic activity to those of blood pressure and heart rate, physiological variables which reflect sympathetic activity. 1. Forearm venous plasma noradrenaline, heart rate and intra-arterial blood pressure were measured sequentially during and after upright bicycle exercise in five normotensive and six hypertensive patients. 2. Plasma noradrenaline increased significantly between 4 and 8 min during exercise. 3. On stopping exercise blood pressure and heart rate decreased rapidly whilst plasma noradrenaline increased in each subject to reach a maximum at a median time of 108 s after exercise. 4. Plasma noradrenaline decreased in five of six normotensive patients between the end of exercise and 2 min after exercise performed in the supine position. 5. Evidence in favour of a reflex increase in sympathetic activity after upright exercise is discussed. Subjects and methods Upright exercise Upright exercise was studied in 11 untreated subjects, five normotensive and six hypertensive; supine exercise was studied in six patients during cardiac catheterization. Patients 1-5 (Table 1) were normotensive subjects referred for investigation of chest pain. Mean age was 35 years; four were male and two (patients 3 and 4) were smokers. Outpatient blood pressure was 150/95 mmHg or less. Clinical examination, resting and exercise electrocardiograms were normal and the final diagnosis was skeletal chest pain. Patients 6-1 1 (Table 1) had mild to moderate essential hypertension. Mean age was 46 years; four were male and patient 10 was a smoker. Repeated outpatient blood pressure measurements were greater than 150/95 mmHg and-all were free of target organ damage (no cerebrovascular or coronary artery disease; no left ventricular hypertrophy and normal concentrations of plasma creatine and electrolytes). Sodium intake was controlled by avoiding added salt, apart from that used in cooking, for 3 days before admission. The normotensive subjects were Key words: blood pressure, exercise, heart rate, noradrenaline, sympathetic activity. Introduction The increase in sympathetic activity during physical exercise is accompanied by increased concentrations of venous plasma noradrenaline (Vendsalu, 1960). Sudden cessation of physical activity demands rapid homeostasis by the cardioPresent address: Department of Materia Medica, Stobhill General Hospital, Glasgow G2 1, Scotland, U.K. Correspondence: Professor W.A. Littler, Department of Cardiovascular Medicine, East Birmingham Hospital, Bordesley Green East, Birmingham B9 5ST,U.K. 37 0143.522 1/80/0 lOO37-07SI .SO/ I R . D. S. Watson el al. 38 TABLE 1. Details ofpatients 1-1 1 who petformed upright exercise Patient no. Sex Age (years) Body surface area Exercise workload M M M I F M M F F M M M I1 Mean 5 SEM Heart rate (beats/min) Systolic blood pressure (mmHg) (W) (m3 2 3 4 5 6 7 8 9 10 Outpatient blood pressure (mmHg) Systolic Diastolic Control Exercise Control Exercise 79 82 74 75 135 181 133 140 162 178 156 139 120 I24 144 149 132 140 132 186 152 I60 124 172 146 203 220 I86 190 184 262 I89 219 I82 224 193 14457 14956 20557 33 31 46 37 29 46 49 43 44 44 52 2.26 1.97 2.04 1.48 1.83 1.89 1.95 I *42 1.92 1.90 1.74 150 135 I55 70 I70 160 70 55 80 95 75 131 I50 132 I25 140 190 187 I75 157 200 I70 78 95 91 75 86 122 102 101 99 I08 102 41t3 1.855 0.07 1 1 O t 13 16058 96t4 studied during a 3 h attendance at hospital and observations were commenced 30 min after arterial cannulation. The hypertensive subjects were studied 24 h after admission to hospital and whilst in hospital they received a diet containing 60 mmol of sodium daily. Subjects performed upright exercise for 8 rnin on a bicycle ergometer (Elema Schonander) at a constant load, determined as the load causing 85% of maximum heart rate during a previous upright multistage test to maximum voluntary effort. Supine exercise Patients 12- 17 (Table 3) were investigated during cardiac catheterization. Mean age was 36 years; four were male and patients 12 and 15 were smokers. They were premedicated with diazepam (10 mg orally) and sodium intake was not controlled. Bicycle exercise was performed for 6 rnin at constant load, starting 20 min after arterial cannulation. The workload was determined from a previous supine exercise test to exhaustion as for upright exercise. Arterial pressure and heart rate Arterial pressure was measured from a fine polyethylene cannula in the brachial artery connected to a Gaeltec 3EA-a transducer (frequency response flat to 20 Hz). Heart rate (from electrocardiogram) and blood pressure were recorded on a Mingograf 81 (Elema Schonander) recorder at 10 100 87 80 97 73 80 97 84+3 111 mm/s. Control observations were made after 10 min rest on the bicycle ergometer, during the last 20 s of each minute during exercise and for 10 rnin after exercise whilst the subject remained in the same position. Blood pressure was averaged by digitizing the last 15 beats recorded. Plasma noradrenaline Venous blood (10 ml) was taken into a cooled syringe from a forearm cannula (Venflon 17G) without occlusion and transferred to a heparinized tube in crushed ice until centrifugation at 4°C and storage at -2OOC within 30 min of sampling. Plasma noradrenaline was measured within 4 weeks by the method of Henry, Starman, Johnson & Williams (1975), a radioenzymatic method utilizing partially purified bovine phenylethanolamine N-methyltransferase. Samples from each patient were analysed as one batch in duplicate with internal standards. The method is specific for noradrenaline and sensitive to 0 . 3 nmol/l. For upright exercise specimens were obtained immediately before cycling and during minutes 4 and 8 of exercise; after exercise, further specimens were obtained up to 20 rnin whilst the subject remained on the ergometer; after exercise, the timing of samples varied between subjects and was more frequent in the early post-exercise period; the time was recorded as the mid-point of sampling. For supine exercise, specimens were obtained during the last minute of exercise and at 1 rnin postexercise. Informed consent for the investigation was obtained from each patient and the investigations Plasma noradrenaline during bicycling were approved by the local Hospital Ethics Committee. Data analysis All results are expressed as means f 1 SEM. The significance of differences in mean values was tested with a two-tailed Student’s t-test for paired or unpaired samples as appropriate. The Fisher exact probability test was used to compare changes in noradrenaline during supine and upright exercise. (Siegel, 1956.) Results Upright bicycle exercise The average number of blood specimens obtained after exercise was five. In patient 2, three specimens were obtained within 6 rnin after exercise before he developed postural hypotension and had to lie down. Patient 8 became exhausted after 5 min of exercise. Personal characteristics are shown in Table 1. The normotensive subjects were significantly younger than the hypertensive patients (35 f 3 against 46 f 1 years; P < 0.02) and cycled at a higher workload (136 f 17 against 85 f 15 W; 0.05 < P < 0.1). Mean heart rate increased from 84 f 3 beats/min at rest to 144 f 7 beats/min and mean systolic blood pressure increased from 149 f 6 mmHg at rest to 205 f 7 mmHg during exercise. Mean plasma noradrenaline (Table 2) before exercise was 4.18 f 0.94 nmol/l and tended to be 39 higher in the hypertensive than the normotensive patients (5.55 f 1.50 against 2-54 f 0.48 nmol/l); the difference was not significant (P > 0.05). Plasma noradrenaline increased significantly during exercise and the mean concentration at 8 rnin was 8.92 f 1.73 nmol/l (P< 0.001). In the seven patients for whom values were available at 4 and 8 rnin during exercise, plasma noradrenaline increased significantly between these times (at 4 min: 7-44 f 2.66 nm..l/l; at 8 min: 8.80 f 2.54 nmol/l; P < 0.02). An increase in plasma noradrenaline occurred in all patients after upright exercise (Table 2). Mean plasma noradrenaline increased significantly from 8.92 f 1-72 nmol/l at the end of exercise to a maximum level of 11-89 & 2.23 nmol/l after exercise (P< 0.01). The increase varied from 0 - 4 7 to 8.15 nmol/l. The median time of the peak plasma noradrenaline was 108 s after exercise and varied widely from 39 to 4 18 s. The range of plasma noradrenaline levels at rest and during exercise was wide (Table 2). Fig. 1 shows changes in plasma noradrenaline as a percentage of the maximum in each patient, together with heart rate and systolic blood pressure. Observations for patient 2, who had postural hypotension after exercise, have been excluded. On stopping exercise, both heart rate and systolic blood pressure decreased rapidly whereas plasma noradrenaline tended to increase during the first 2 rnin before decreasing towards control values by about 12 min. At 6 rnin after exercise, systolic blood pressure decreased significantly below the pre-exercise value (control: 149 f 6 mmHg; 6 rnin post-exercise: 139 f 4 mmHg; P < 0.05); heart TABLE2. Plasma noradrenaline concentrations and times of maximum values Mer upright exercise Patient Plasma noradrenaline (nmol/l) no. Before exercise During last minute of exercise Maximum aRer exercise Time of maximum plasma noradrenaline aRer exercise (S) 2 3 4 5 6 7 8 9 10 I1 3.25 4.08 1.89 1.71 1.71 12.82 3.37 3.84 3.19 4.49 5.61 8.27 8.86 4.90 3.54 5.49 23.39 5.79 10.04 6.08 6-67 15.06 11.10 9.92 9.75 4.67 9-92 30.60 6.26 18.19 6.9 1 7.44 16.07 I72 I I5 I78 418 95 95 50 Mean f SEM 4.18 f 0.94 8.92 f 1.73 11.89 f 2.23 138 f 32 I 50 39 203 108 R . D. S . Watson el a / . 40 The disappearance rate of noradrenaline from plasma was followed in eight patients (nos. 1, 3, 5, 6, 7, 8, 10 and 11). The decline was exponential with a time constant (ti) which varied from 3.0 to 19.7 (mean 9.2 i-1.9)min. Supine exercise Patients’ details are shown in Table 3. Mean workload was 118 f 19 W; mean exercise heart rate was 153 C 9 beatshin; mean exercise systolic blood pressure was 185 f 14 mmHg. When plasma noradrenaline at the end of exercise was compared with the concentration 2 min after stopping, a decrease was observed in five of the six patients. The fall in mean concentrations, from 4.44 f 1.06 nmol/l at the end of exercise to 3.02 f 1.04 nmol/l 2 min after stopping, was not statistically significant (0.05 < P < 0.1). . .150 0 8 4 Cornparisori of supine and upright exercise 12>12 Tinic post-cxcrcisc (rnin) FIG. 1. Mean plasma noradrenaline (as a percentage of the maximum concentration attained), systolic blood pressure and heart rate during and after upright exercise in patients 1-1 1. Vertical bars indicate 1 SEM; only the largest values are indicated during exercise. rate remained significantly elevated above control rates up to 10 min after exercise (control heart rate: 84 f 3 beatshin; 10 min post-exercise: 100 f 4 beats/min; P < 0.001). Changes in plasma noradrenaline between the end of supine exercise and 2 min post-exercise (patients 12-17) were compared with changes in seven of the eleven patients who performed upright exercise and in whom plasma noradrenaline measurements were made between 1.5 and 2.5 min after exercise (patients 2, 3,5,6,9, 10 and 11). After upright exercise, plasma noradrenaline increased in six of seven patients, whereas after supine exercise a decrease occurred in five of six patients. The probability of this distribution, or a more extreme one, was 0.025 (Fisher exact TABLE3. Details of patients and plasma noradrenaline concentrations (patients 12-1 7 , who perfortned supitre exercise) Subject no. Age Sex (years) Body surface area Diagnosis Workload (W) (m3 I2 13 36 42 M M 2.06 I .98 14 33 F 1.47 I5 41 35 F 16 M 1.78 2.11 17 31 M 2.19 Mean f SEM 36 f 2 1.93 f O . 1 1 Non-cardiac chest pain Two vessel coronary artery disease Atrial xptal defect (shunt 1.3:1) Non-cardiac chest pain Coronary artery disease excluded Non-cardiac chest pain Maximum exercise hean rate (beatshin) Plasma noradrenaline At end of exercise (nmolll) 2 min rest post-exercise (nmol/l) I40 I30 157 169 5.49 7.21 2.01 7.80 55 I77 7.09 3.66 70 170 118 157 1.95 3.84 1.77 2.4 I 145 I39 I .08 0.47 118 f 19 I53 f 9 4.44 f 1.06 3.02 f 1.04 Plasma noradrenaline during bicycling probability test). The mean percentage increase in plasma noradrenaline after upright exercise (21 & 15%) was significantly different from the mean decrease observed after supine exercise (35 & 12%; P < 0.025), indicating that the patterns of change in plasma noradrenaline after upright and supine exercise were different. Discussion It is important to emphasize that the normotensive subjects were significantly younger than the hypertensive subjccts who performed upright bicycle exercise; although differences with respect to exercise heart rate, exercise workload and resting plasma noradrenaline concentrations were . not significant, we d o not consider that it is possible to compare the changes in two groups of this size, except to demonstrate that they were qualitatively similar. The high plasma noradrenaline concentrations in patient 6 are unexplained; there were no clinical features of phaeochromocytoma and urinary catecholamine excretion was normal. We attempted to standardize the workload in each subject, since the increase in plasma noradrenaline during exercise is related to the intensity of work (Kotchen, Hartley, Rice, Mougey, Jones & Mason, 1971). This was only partly successful in that the exercise heart rate varied from 1 1 1 to 18 1 beats/min. However, the approximately twofold increase in plasma noradrenaline during exercise suggested that the intensity of exercise was sufficient to cause a substantial increase in sympathetic activity. The increase in plasma noradrenaline during exercise confirms the observations of others (Vendsalu, 1960; Kotchen et al., 1971). However, our observations showed that after stopping bicycle exercise and remaining in the upright position, plasma noradrenaline increased during the early post-exercise period in every subject; the increase between the end of exercise and the maximum concentration of plasma noradrenaline after exercise was statistically significant. Most investigators have examined changes in plasma noradrenaline during, rather than aAer, exercise; however, Cryssanthopoulos, Barboriak, Fink, Stekiel & Maksud (1978) noted that plasma noradrenaline was higher 5 min after exercise than at the end of exercise, although the increase was not significant. The timing of the peak plasma noradrenaline after upright exercise varied considerably between individuals. Although the exact timing of samples was not standardized, at least one specimen was 41 taken within 1 min and three specimens within 5 min after exercise. More frequent sampling would define the peak time more accurately; the fact that an increase was observed in each subject without more frequent sampling suggests that the increase is sustained for 1-2 min. There are a number of possible explanations of why plasma noradrenaline concentrations were highest after exercise. In the' upright position, reduced venous return to the heart due to pooling of blood in the vasodilated lower limbs, together with the fall in blood pressure on stopping exercise, will result in reduced stimulation of the low pressure cardiopulmonary and the high pressure sino-aortic receptors and a reflex increase in sympathetic vasoconstrictor activity would be expected. Although the activity of the sino-aortic baroreflex is inhibited during exercise, its activity returns quickly on stopping (Bristow, Brown, Cunningham, Howson, Strange Petersen, Pickering & Sleight, 1971). Changes in the level of sino-aortic baroreceptor resistance (Carlsten, Folkow, Grimby, Hamberger & Thulesius, 1958; Bjurstedt, Rosenhamer & Tyden, 1975) and alterations in cardiopulmonary afferent discharge rate have greater effects on systemic and renal vascular resistance at low than at high carotid sinus pressures in the dog, indicating an important interaction between the reflexes (Mancia, Shepherd & Donald, 1976). The observation that the pattern of change in plasma noradrenaline differed between supine and upright exercise would support a reflex increase in sympathetic activity since more marked pooling of blood after upright exercise would be expected. Two other explanations need to be considered; first, an increase in plasma noradrenaline after upright exercise could be due to delayed washout of noradrenaline from the tissues. However, this mechanism would not explain the difference observed between supine and upright exercise. The plasma noradrenaline concentrations during upright exercise were much higher than during supine exercise and an alternative explanation is that the mechanisms responsible for clearance of noradrenaline from the circulation may become saturated at high plasma concentrations (Vane, 1969); this would explain the fall in plasma noradrenaline after supine exercise but would not explain the increase observed after upright exercise. The disappearance rate of noradrenaline in our patients was considerably longer than that seen after cessation of a 10 h infusion of noradrenaline in normal resting subjects (Fitzgerald, Hossman, 42 R . D. S . Watson et al. Hamilton, Reid, Davies & Dollery, 1978). The slower decline after exercise is consistent with continuing sympathetic activity or could be due to a reduction in noradrenaline clearance. Although circulating concentrations of noradrenaline at rest are unlikely to have significant effects on heart rate or blood pressure, those achieved after exercise were similar to the concentrations, which, after intravenous infusion, caused an increase in blood pressure (Dargie, Davies, Dean, Dollery, Maling & Reid, 1977). The delay in reaching maximal concentrations of plasma noradrenaline after upright exercise may be relevant to the development of exercise-induced asthma and arrhythmias. The effects of a-adrenoreceptor antagonists in preventing exercise-induced asthma are consistent with the existence of an abnormal balance between a- and Preceptor tone in bronchial smooth muscle in susceptible individuals (Bianco, Griffin, Kamburoff & Prime, 1974; Gross, Souhrada & Farr, 1974; Patel, Kerr, MacDonald & MacKenzie, 1976). Symptoms occur most commonly after stopping exercise at a time when plasma noradrenaline concentrations are higher and it is possible that meceptor effects of sympathetic stimulation or circulating plasma noradrenaline may explain why bronchoconstriction becomes more severe at this time. Anderson, Lee, Campion, Amplatz & Tuna (1972) and Goldschlager, Cake & Cohn (1973) observed that the highest incidence of ventricular arrhythmias occurred shortly after exercise stress testing, and again it is possible that the high sympathetic tone and plasma noradrenaline concentration at this time may be important in causing arrhythmias. Additionally, plasma free fatty acid changes after exercise resemble those of plasma noradrenaline, reaching a maximum within 5 min of stopping exercise (Carlson & Pernow, 1961); although decreased effiux from the circulation is partly responsible for this increase, increased mobilization due to sympathetic activity may contribute (Havel, Naimark & Borchgrevink, 1963). Finally, our observations emphasize that the timing of blood specimens is of critical importance in comparing the effects of drugs on exerciseinduced changes in plasma noradrenaline, not only because the sequential changes in plasma noradrenaline are rapid and the timing of the peak noradrenaline concentration varies considerably between individuals, but also because the effects of drugs on plasma noradrenaline Concentrations during exercise may be different from those on the concentrations after exercise. Acknowledgments We thank Dr S. Hill for technical assistance and Miss A. Strong for secretarial assistance. We are grateful for financial support from the Wellcome Trust, the British Heart Foundation and May and Baker Ltd. References ANDERSON, M.T., LEE, G.B., CAMPION, B.C.. AMPUTZ, K. & TUNA, N. (1972) Cardiac dysrhythmias associated with exercise testing. American Journal of Cardiology, 30. 763767. BIANCO.S.. GRIFFIN,J.P., KAMBUROFF, P.L. & PRIME,FJ. (1974)Prevention of exercise induced asthma by indoramin. British Medical Journal, iv, 18-20. BJURSTEDT, H., ROSENHAMER, G. & TYDEN.G. (1975)Cardiovascular responses to changes in carotid sinus transmural pressure in man. Acta Physiologica Scandinavica. 94,497505. BRISTOW,J.D., BROWN,E.B.. CUNNINGHAM. DJ.C., HOWSON, M.G.. STRANGEPETERSEN.E., PICKERING. T.G. & SLEIGHT, P. (1971) Effect of bicycling on the baroreflex regulation of pulse interval. Circulation Research, 28.582-592. CARLSON,L.A. & PERNOW,B. (1961)Studies on blood lipids during exercise. (ii) The arterial free fatty acid concentration during and after exercise and its regulation. Journal of Laboratory and Clinical Medicine, 58,673-68 1. CARLSTEN.A., FOLKOW, B.. GRIMBY. G., HAMBERGER, C.-A. & THULESIUS.0. (1958) Cardiovascular effects of direct simulation of the carotid sinus nerve in man. Acta Physiologica Scandinavica, 44, 138-145. CRYSSANTHOPOULOS, C.. BAREORIAK, J.T.. FINK,J.N.. STEKIEL, W J . & MAKSUD,M.G. (1978) Adrencrgic responses of asthmatic and normal subjects to submaximal and maximal work loads. Journal of Allergy and Clinical Immunology, 61, 17-22. DARGIE,HJ., DAvIes, D.S.. DEAN, C.R.. DOLLERY.C.T., MALING.T.J.B. & REID, J.L. (1977) The effect of noradrenaline infusion on blood pressure and plasma noradrenaline following clonidine administration in man. British Journal of Pharmacology, 60,389~390~. FITZGERALD, G.A., HOSSMAN, V., HAMILTON, C.A., REID,J.L., DAVIES. D.S. & DDLLERY.C.T. (1978) Interindividual variation in noradrenaline kinetics. Proceedings of the 7th International Congress of Pharmacology, vol. 2. p. 549. Pergamon Press, Oxford. GOLDSCHLAGER. N., CAKE,D. & COHN.K. (1973)Exerciseinduced ventricular arrhythmias in patients with coronary artery disease: their relationship to angiographic findings. American Journal of Cardiology, 31.434-440. GROSS,G.N., S O U H R A D J.F. ~ & FAR&R.S. (1974)The long term treatment of an asthmatic patient using phentolamine. Chest, 66.397401. HAVEL.J.H.. NAIMARK, A. & BORCHGREVINK, C.F. (1963) Turnover rate and oxidation of free fatty acids of blood plasma in man during exercise: studies during continuous infusion of palmitate-I-C". Journal of Clinical Investigaiion, 42,1054-1063. HENRY,D.P., STARMAN,BJ., JOHNSON,D.G. & WILLIAMS, R.H. (1975) A sensitive radioenzymatic assay for norepinephrine in plasma and tissues. L r e Science. 16,375-384. KOTCHEN, T.A.. HARTLEY,C.H., RICE,T.W.. Mouoey. EH., JONES,L.G. & MASON,J.W. (1971)Renin, norepinephrine and epinephrine responses to graded exercise Journal o/ AppliedPhysiology, 2,178-184. MANCIA.G., SHEPHERD, J.T. & DONALD,D.E. (1976)Interplay among carotid sinus, cardiopulmonary, and carotid body reflexes in dogs. American Journalof Physiology, 230.19-24. Plasma noradrenaline during bicycling PATELK.R.. KERR, J.W.,MACDONALD, EB. & MACKENZIE, A.M. (1976) The effect of thymoxamine and cromolyn sodium on post-exercise bronchoconstriction in asthma. Journal of Allergy and Clinical Immunology, 51,285-292. SIEGEL. S. (1956) In: Non-Parametric Statistla for the Eelrauioural Sciences. McGraw-Hill Kogakusha, Tokyo. 43 VANE, J.R. (1969) The release and fate of vaw-active hormones in the circulation.Brltish Journal of Pharmacology, 35,209242. VENDSALU, A. (1960) Studies on adrenaline and noradrenaline in human plasma. Acra Physiologica Scandinavlca, 48 (SUPPI.173). 8-1 14.