Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
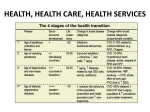
Case No. 15 1 Author: Kanawat Kanjanapiboon, M.D. Chakkrapong Chunhasewee, M.D. Patient: A 66-year-old Thai woman from Samut Prakarn Chief complaint: Bilateral symmetrical linear firm plaques on the radial side of the index fingers for 10 years Present illness: The patient developed bilateral asymptomatic symmetrical plaques on the distal part of radial side of both index fingers for 10 years. The lesions gradually extended to proximal part of radial side of both index fingers. Past history: The patient denies any underlying diseases Family history: No family members experienced with this condition similar to the patient. Physical examination: Unremarkable Dermatologic examination: Bilateral symmetrical ill-defined border glistening skin color hyperkeratotic plaques distributed in linear pattern along the radial side of the index fingers and extended to the ulnar side of both hands. Histopathology: Slide No. 58-3275, 58-3275* Sections display slightly acanthotic acral epidermis with hyperkeratosis. Neither spongiosis nor interface change is seen. The dermis shows increased bluish material with entrapped collagen bundles. No cellular component is observed. Verhoeff van Gieson demonstrates decreased numbers of elastic fibers. Diagnosis: Degenerative collagenous plaques of the hands Treatment: Topical treatments with retinoids, urea and salicylic acid creams have been applied and avoiding sunlight and wearing gloves were also advised. Avoidance of repetitive pressure or friction is suggested to prevent disease progression. Discussion: Degenerative collagenous plaques of the hands (DCPH) develop in the sixth to seventh decade of life.1 Men are more predominantly affected than women. A high proportion of cases are reported in Caucasians. There is no familial predisposition. The clinical manifestations are bilateral with symmetrical linear plaques at the junction of the dorsal and palmar skin from the medial aspect of the thumb distally onto the lateral aspect of the index finger. The lesions extend to the distal interphalangeal joint of the index finger. The ulnar side of the hand and other sites on the fingers are rarely involved. The course of this disease is slowly progressive and asymptomatic. The pathological findings of DCPH show an acellular zone of haphazardly arranged collagen with some bundles running perpendicular to the epidermis.2 The bundles of collagen are admixed with fragmented elastic fibers and distinctive angulated amorphous basophilic elastotic masses in the upper dermis. These masses are composed of degenerative elastic fibers and calcium.1 Chornic actinic damage and repetitive long-term trauma and pressure inducing degenerative collagenous and elastotic processes are implicated in the pathogenesis.3,4 Acrokeratoelastoidosis (AKE) and focal acral hyperkeratosis are two important entities in the differential diagnosis of DCPH. Table1. The differential diagnosis of DCPH5 Disorder Clinical features Histologic features Degenerative collagenous More common in older Marked degeneration of plaques patients (40-60 years), collagen and elastin usually associated with fibers chronic sun exposure Acrokeratoelastoidosis Small round-oval to Hyperkeratosis, (AKE) rhomboid-shaped, epidermal hypertrophy, yellowish papules on and decreased elastic palmar/plantar surfaces fibers in the dermis of the hands and feet Focal acral hyperkeratosis Identical to AKE, except Lack of elastorhexis in (FAH) it is more common in the dermis, elastic tissue blacks is intact According to the table shown above, this case is clinically and histologically compatible with DCPH. Interhospital Conference 2016 Institute of Dermatology 35 References: 1. Jordaan HF, Rossouw DJ. Digital papular calcific elastosis: A histopathological, histochemical and ultrastructural study of 20 patients. J Cutan Pathol 1990; 17: 358-370. 2. Richie EB, Williams HM. Degenerative collagenous plaques of the hands. Arch Dermatol 1996; 93: 202-203. 3. Mehregan AH. Degenerative collagenous plaques of the hands. Arch Dermatol 1966; 93: 633. 4. Koscard E. Keratoelastoidosis marginalis of the hands. Dermatologica 1964; 131: 169-175. 5. Weimin Hu, Thomas F. Cook, Gary J. Vicki, and Dee Anna Glasser. Acrokeratoelastoidosis. Pediatric Dermatol 2002; 19: 320-2. Interhospital Conference 2016 Institute of Dermatology 36