Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
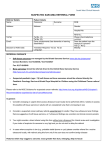
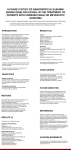
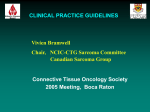
3 Worse survival in elderly patients with extremity soft-tissue sarcoma Miriam L. Hoven- Gondrie1, Esther Bastiaannet1,2, Vincent K.Y. Ho3, Barbara L. van Leeuwen1, Gerrit-Jan Liefers2, Harald J. Hoekstra1, Albert J. H. Suurmeijer4 Department of Surgery, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands 2 Department of Surgery, Leiden University Medical Center, University of Leiden, Leiden, the Netherlands 3 Comprehensive Cancer Center Netherlands, Utrecht, the Netherlands 4 Department of Pathology, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands Introduction 1 Submitted Abstract Background Nearly half of soft-tissue sarcoma (STS) patients are over the age of 65. The aim of this study was to assess the impact of age, sarcoma histotype, grade, stage and treatment modalities on survival of extremity STS (ESTS) patients. Methods Patients ≥18 years, diagnosed with ESTS between 1989 and 2008, were selected from the Netherlands Cancer Registry (NCR). Survival rates and treatment characteristics were analyzed for all patients. Treatment was categorized in no treatment, monotherapy (surgery, radiotherapy or chemotherapy) and various combined modality treatments. Relative survival and Relative Excess Risks of death (RER) were estimated. Results Overall, 3375 patients were included in this study. Histotype was different between young and elderly patients (p < 0.001). The oldest elderly were diagnosed more often with high-grade and stage IV disease (p < 0.001). The proportion of patients who received no treatment increased from 3% in the youngest group to 17% in the oldest elderly. The elderly received fewer combined modality treatments (p < 0.001). Age was significantly associated with relative 5-year survival (73.4% for younger patients and 25.8% for the oldest elderly). In multivariate analysis, adjusted for sex, histotype, grade and treatment, age still remained a significant prognostic factor for stage II and III ESTS patients. Conclusion Different distribution of sarcoma histotypes, a higher stage and more high-grade sarcomas at diagnosis, less aggressive treatment and worse survival rates in stage II and III ESTS urge the need for optimizing sarcoma care of the elderly in order to improve their prognosis. Soft-tissue sarcomas (STS) are relatively rare tumors and account for 1% of all cancers in adults. The overall incidence of STS in the Netherlands is 2.7/100,000 (European Standardized Rate 2009).1 There has been a slight increase in the incidence of STS in men. Nearly 50% of the diagnosed patients are over 65 years of age.2 Fifty to 60% of STS are localized in the extremities. The most common sarcoma histotypes are pleomorphic undifferentiated sarcoma (malignant fibrous histiocytoma), liposarcoma, leiomyosarcoma and fibrosarcoma.2,3 Important prognostic factors for STS are primary site, tumor size, histotype, grade and stage at presentation.3 Age at presentation determines survival in several distinct STS histotypes.4-9 The behavior of cancer in elderly patients is poorly understood. There is a widespread misconception that the elderly are poorly tolerant of chemotherapy and radiotherapy. In daily clinical practice, elderly patients may be undertreated compared to young or middle-aged STS patients, and this may influence their prognosis.2,10-12 Moreover, elderly patients are generally underrepresented in cancer trials, which compromises our knowledge of the effectiveness of sarcoma treatment for this age group.13 For extremity STS (ESTS) there is a well-defined role for surgery and radiation therapy.14 In ESTS removed with narrow margins or microscopically (R1) or macroscopically (R2) positive resection margins, 50-70 Gy of external-beam radiation therapy (EBRT) is indicated.15,16 The main goal of this study was to assess the impact of age on relative survival of adult ESTS patients diagnosed in the Netherlands. Relevant prognostic factors for survival of STS were included. Stage at diagnosis, sarcoma histotype, tumor grade and treatment regimens were compared between young and elderly sarcoma patients and analyzed in a multivariable fashion. Patients and methods Patients Patients (age 18 and older) diagnosed with ESTS as first primary malignancy in the period 1989-2008 were selected from the Netherlands Cancer Registry (NCR). Patients with Kaposi sarcoma, dermatofibrosarcoma protuberans and Ewing sarcoma were excluded (Table 1). PALGA, the Dutch nationwide network of histopathology and cytopathology diagnosis, regularly submits reports of all 33 3 Table 1: Morphology codes included in the selection of patients with softtissue sarcoma Group Morphology (WHO 2002) N Dedifferentiated liposarcoma 8858 22 Myxoid & round cell liposarcoma 8852 & 8853 369 Pleomorphic liposarcoma 8854 87 Mixed-type liposarcoma 8855 30 Fibrosarcoma 8825, 8811, 8814, 8810, 8812 & 8813 330 Pleomorphic undifferentiated sarcoma 8830 & 8800-8809 1055 Leiomyosarcoma 8890, 8891 & 8896 644 Rhabdomyosarcoma 8900-8902, 8910, 8912, 8920 & 8921 84 Angiosarcoma 9120 57 Synovial sarcoma 9040-9043 262 MPNST 9540 106 Other 9581, 9044, 8963, 9231, 9180 & 8850 309 Overall All 3375 MPNST, malignant peripheral nerve sheath tumor Exclusion: Kaposi sarcoma, dermatofibrosarcoma protuberans, Ewing sarcoma inhabitants’ vital status. The WHO Classification of soft tissue sarcoma was used for histopathological classification of sarcoma histotypes.19 Because the latest WHO Classification of STS appeared in 2002, the distribution of sarcoma histotypes according to age was analyzed with data from 2003-2008. Statistics Age was categorized in the following groups: patients younger than 65 and elderly aged 65-69, 70-74, 75-79, 80-84, 85-89 and older than 89. Missing data for grade and stage were imputated using multiple imputation with five imputations using a model with age, sex, year, morphology, status, stage and grade.20 Distribution of sarcomas according to age was assessed for the years 2003 to 2008. Stage at diagnosis was compared according to age categories. Treatment was categorized into no treatment, monotherapy (surgery, radiotherapy and chemotherapy) and several combinations of treatment. Relative survival was calculated and Relative Excess Risks of death (RER) were estimated using a multivariable generalized linear model with a Poisson error structure, based on collapsed relative survival data, using exact survival times. Survival time was calculated from the date of diagnosis and ended at the date of death, date of last contact, or date of most recent linkage with the municipal population registries, whichever came first. Relative mortality was calculated by the equation: (observed deaths – expected deaths) / observed deaths. National life tables were used to estimate expected survival. STATA SE 10.0 software was used to perform statistical analyses. Results diagnosed malignancies to the cancer registries. The national hospital discharge databank, which receives discharge diagnoses of admitted patients from all Dutch hospitals, completed case ascertainment. After notification, trained registry personnel collected data on diagnosis, stage and treatment from the medical records, including pathology and surgery reports, using the registration and coding manual of the NCR. Treatment was coded in sequence of administration. Stage was assigned according to the American Joint Committee on Cancer and grade according to Coindre.17,18 Vital status was established either directly from the patient’s medical record or through linkage of cancer registry data with the municipal population registries, which recorded information on their 34 Survival in young and elderly soft-tissue sarcoma patients As shown in Table 2, 3375 patients were included in this study. At first diagnosis, nearly 40% of patients were elderly, aged 65 years or older, nearly 75% had highgrade sarcomas, and 60% were diagnosed with stage I or II disease. As shown in Figure 1, there were significant differences in distribution of sarcoma histotypes in young versus elderly patients (p < 0.001). Using 65 years of age as cut-off value, myxoid and round cell liposarcoma was diagnosed more often in younger patients (p=0.002), whereas pleomorphic undifferentiated sarcoma was recorded more often in the elderly (p=0.003). Leiomyosarcoma was predominantly diagnosed in the 70-74 age group (p=0.05). 35 3 23.3 23.5 25.7 27.5 23.3 23.5 25.7 27.5 Grade Low High Missing 736 2252 387 21.8 66.7 11.5 25.2 74.8 Stage I II III IV Missing 615 451 308 322 1679 18.2 13.4 9.1 9.5 49.8 33.5 26.4 20.1 20.0 3375 100 100 Survival in young and elderly soft-tissue sarcoma patients Pleomorphic liposarcoma Pleomorphic undifferentiated sarcoma Angiosarcoma Other 785 794 868 928 Myxoid & round cell liposarcoma Fibrosarcoma Rhabdomyosarcoma MPNST, malignant peripheral nerve sheath tumor 1989-1993 1994-1998 1999-2003 2004-2008 Dedifferentiated liposarcoma Mixed-type liposarcoma Leiomyosarcoma Synovial sarcoma Year 80% 53.5 46.5 60% 53.5 46.5 40% 1806 1569 20% Male Female 3 0% Sex <65 61.4 9.5 8.8 8.6 6.5 3.7 1.6 65-69 61.4 9.5 8.8 8.6 6.5 3.7 1.6 70-74 2071 321 296 289 218 126 54 75-79 < 65 65-69 70-74 75-79 80-84 85-89 90+ 80-84 % 85-89 % Age (years) Total 36 N 90+ Variable Multiple imputation Figure 1: Distribution of sarcomas (2003-2008) according to age Original dataset 100% Table 2: Characteristics of the population (n=3375) 37 32 28 20 21 80-84 85-89 34 39 31 27 25 17 0% <65 65-69 Stage I 38 70-74 Stage II 75-79 Stage III Stage IV Survival in young and elderly soft-tissue sarcoma patients 90 and older < 0.001 0 0.6 0 0 0 0 < 0.001 0 3.4 1.3 1.4 0.5 0 < 0.001 18.5 42.7 43.9 36.3 36.2 28.6 < 0.001 0 5.0 3.4 1.7 2.7 0 < 0.001 1.8 4.4 4.7 2.4 1.8 2.4 < 0.001 1.8 1.2 2.0 4.1 4.1 2.4 < 0.001 61.1 38.3 36.5 48.4 40.4 50.0 < 0.001 16.7 4.4 8.1 5.5 14.2 16.7 p-value* % % % % % % % 90+ 65-69 70-74 75-79 80-84 85-89 < 65 3 *p-value for trend over age 29 0.8 20% 29 Chemotherapy & radiotherapy 28 40% 4.8 25 Surgery & radiotherapy & chemotherapy 26 38.1 24 Surgery & radiotherapy 60% 5.1 24 Surgery & chemotherapy 18 3.9 25 80% Chemotherapy (monotherapy) 22 23 0.6 21 26 Radiotherapy (monotherapy) 23 43.9 24 Surgery (monotherapy) 23 2.8 18 18 No treatment 100% Treatment Figure 2: Stage at diagnosis according to age groups (all years) Table 3: Treatment of soft-tissue sarcoma in the extremities Stage at diagnosis was different between age categories (p < 0.001). The relative proportion of Stage I diminished from 39% in the younger patients to 17% for the oldest elderly. Stage II was more prominent among the elderly (34% compared to 25% in patients younger than 65). The proportion of Stage III was equal between age categories, approximately 20-25%. The proportion of patients with stage IV was higher among the elderly, ranging from 18% in patients younger than 65 years to approximately 25% among the elderly (Figure 2). Elderly patients presented with high-grade disease more often, ranging from 69.9% high-grade in patients younger than 65 to 87.5% in the 85-89 age group and 83.7% in patients over 90 years (p < 0.001). As shown in Table 3, the proportion of patients that received no treatment was remarkably higher among the elderly, particularly patients older than 80. About 15% of patients older than 80 received no treatment compared to 2.8% of patients younger than 65 (p < 0.001). Surgery as sole treatment was administered more often to the elderly (ranging from 44% in the young to 61% in the oldest elderly; p < 0.001). A combination of surgery and radiotherapy was given less often to the elderly, particularly patients older than 85 years of age: 38% of patients younger than 65 compared to 19% of the oldest elderly (p < 0.001). Patients younger than 65 had a 5-year relative survival (all stages) of 73.4% (95%CI 72.5-74.3). For elderly patients the 5-year relative survival was significantly worse, decreasing with age to 25.8% for the oldest elderly (Table 4). When adjusted for sex, year, sarcoma histotype, grade and treatment in multivariate analysis, this survival difference was mainly found in stage II and III ESTS patients (Figure 3). Table 5 shows the RER for age stratified according to sarcoma histotype diagnosed in 2003-2008. For all sarcomas, age was a significant prognostic factor with an RER of 1.1 (95%CI 1.0-1.1) per 5-year increase in age. Concerning sarcoma histotype, age was a significant prognostic factor for patients with myxoid and round cell liposarcoma (RER 1.3 (1.1-1.6; p=0.002)) and pleomorphic undifferentiated sarcoma (RER 1.1 (95%CI 1.0-1.2; p=0.003)). Figure 4 clearly illustrates that the estimated deaths (the equation of observedexpected deaths/observed deaths) due to sarcoma after 10 years of follow-up rapidly decreases among the elderly, although the proportion does not decrease below 50% of all deaths. Figure 3: Relative survival according to age and stage* 3 *Adjusted for sex, histotype, grade and treatment Table 4: Relative survival (RS) according to age Age 5-years RS RER (95%CI) p-value Adjusted* RER p-value < 65 73.4 (72.5-74.3) Reference 65-69 67.7 (64.8-70.4) 1.2 (1.0-1.6) 0.06 1.1 (0.9-1.4) 0.4 70-74 58.9 (55.6-62.1) 1.8 (1.4-2.2) < 0.001 1.5 (1.2-1.9) 0.001 75-79 59.6 (55.9-63.3) 1.9 (1.5-2.4) < 0.001 2.0 (1.6-2.6) < 0.001 80-84 55.4 (50.4-60.4) 2.0 (1.5-2.7) < 0.001 1.6 (1.2-2.2) 0.001 85-89 53.7 (45.3-62.6) 2.7 (1.9-3.9) < 0.001 1.5 (1.0-2.2) 0.046 90+ 25.8 (15.2-40.5) 3.7 (2.2-6.4) < 0.001 2.1 (1.1-4.0) 0.03 Figure 4: Observed–Expected deaths (10-year follow-up) as proportion of the observed deaths in the population of sarcoma patients according to age Reference *Adjusted for sex, year, sarcoma histotype, grade and treatment. 40 Survival in young and elderly soft-tissue sarcoma patients 41 Table 5: Survival analysis to assess whether age (per 5-year increase) is a prognostic factor for relative survival according to morphology (2003-2008) Morphology RER for age (95%CI) p-value Dedifferentiated liposarcoma 1.6 (0.9-2.6) 0.08 Myxoid & round cell liposarcoma 1.3 (1.1-1.6) 0.002 Pleomorphic liposarcoma 1.0 (0.7-1.4) 0.8 Mixed-type liposarcoma 1.0 (0.9-1.1) 0.6 Fibrosarcoma 1.0 (0.7-1.4) 0.9 Pleomorphic undifferentiated sarcoma 1.1 (1.0-1.2) 0.003 Leiomyosarcoma 1.1 (1.0-1.2) 0.05 Rhabdomyosarcoma 1.1 (0.9-1.3) 0.3 Angiosarcoma 1.1 (0.9-1.3) 0.3 Synovial sarcoma 1.0 (0.8-1.2) 0.8 MPNST 1.1 (1.0-1.2) 0.2 Other 0.9 (0.7-1.0) 0.07 All soft-tissue sarcomas 1.1 (1.0-1.1) < 0.001 MPNST, malignant peripheral nerve sheath tumor Discussion Since the elderly population is growing fast and incidence of STS increases with age, elderly cancer care has become a growing challenge to the world health care systems. In keeping with most other series, we found worse survival outcomes among elderly STS patients. Several tumor and treatment characteristics have been mentioned as possible explanations for this inferior prognosis.9,21-24 Part of the reason older patients do worse is that they often present with larger and more high-grade tumors. This increased rate of high-grade tumors may reflect a different tumor biology and more genetic alterations and molecular aberrations in the older population.25 Age can also be associated with a decline in antitumor 42 Survival in young and elderly soft-tissue sarcoma patients cell-mediated immunity.26 Concerning sarcoma histotype, more pleomorphic undifferentiated sarcomas are diagnosed in the elderly, which are known to have a relatively adverse prognosis.24 Strikingly, for this histotype and for myxoid and round cell liposarcomas we found significantly worse survival rates for elderly patients compared to their younger counterparts. Growing knowledge of the molecular biology of these diseases has led to the suggestion that the various subtypes of sarcomas should be approached individually.27 As molecular testing also contributes to distinguishing between sarcomas of similar morphology, molecular-based classification of sarcoma should be as important as histological subtype classification in the future.28 For prognosis, treatment or response to treatment, molecular characterization already has clinical implications for some subtypes of sarcoma and new targets for therapy are increasingly being revealed.27 In this series the elderly patients had more stage IV and less stage I disease at presentation. This may be a function of late presentation, often seen in elderly patients with malignancy.21 However, after stratifying for stages there are still significant differences in relative survival between young and elderly ESTS patients. This survival difference was found mainly in stage II and III ESTS patients. A possible explanation might be that less extensive treatment regimens often suffice in patients with stage I disease, so age will not be the reason to withhold any patient from optimal treatment. For stage IV disease we know that overall prognosis is poor for all patients, regardless of the extent of treatment. This leads to the speculation that suboptimal treatment in the elderly might contribute to worse survival rates in stage II and III ESTS patients. A former study from the cancer registry in the northern part of the Netherlands showed that referral to a specialized center declined in a linear fashion with increased age, which might explain this possible suboptimal treatment of elderly patients.10 The mainstay of ESTS treatment is surgery.29 There might be reluctance of surgeons to perform, or of patients to accept, morbid surgeries with increasing patient age, leading to inferior surgical treatment.30,31 Lahat and colleagues already advocated radical surgery in the elderly, as properly selected patients can safely undergo extensive STS resections. Their study showed that even in the group of patients aged ≥ 75, more than half survived 5 years or more when treated with aggressive surgery.22 However, a large but highly select group of patients was investigated in this series. Patients with incomplete resection, insufficient follow-up and nonspecific pathological diagnoses were excluded; this might be a patient group with unfavorable prognostic characteristics, but which could actually benefit from 43 3 better staging, referral or customized treatment. Buchner et al. also justify extensive surgery in bone and soft-tissue sarcoma patients aged > 70. They state however that general condition and comorbidity should be given due consideration.32 Fitness for general anesthesia should be the determinant for suitability for surgery in elderly patients, rather than chronological age.33 Patients with gross disease will benefit from preoperative radiotherapy and those with less than adequate margins after surgery from adjuvant radiotherapy.29 In this study, radiotherapy in combination with surgery was particularly less administrated in the elderly. Logistical problems and patient preferences are often the reason for long courses of external radiation not being offered to elderly patients.21 Horton et al. showed that patients aged ≥ 70 with high-grade ESTS were less likely to receive radiotherapy, and furthermore that not receiving radiotherapy was associated with mortality and disease-specific death.34 In the population-based study of Al-Refaie et al., sarcoma-directed surgery and administration of adjuvant radiotherapy after limb-sparing surgery for T2 or high-grade tumors was only decreased for ESTS patients aged ≥ 85.23 The role of chemotherapy in the treatment of ESTS remains controversial, and toxicity may be significant.29 As expected, administration of chemotherapy with or without surgery and/or radiotherapy declines with age in our series. There is however a widespread misconception that the elderly are always poorly tolerant of chemotherapy. Most adult cancer patients can tolerate it with limited impact on independence, comorbidity and quality of life (QoL) levels.35 The proportion of patients who received no treatment at all increased significantly with age. Former studies from our own center show that the decision to refrain from cancer treatment was mostly disease-related and less often based on poor general health status.12 In conclusion, the principles of treatment for elderly patients are similar to those for younger patients.21 For most ESTS, a combined treatment modality is assumed to be the optimal therapy and will be offered to every patient fit enough to undergo this treatment. Sometimes single treatment (e.g. radical surgery) is the best option for the elderly. Potential undertreatment might thus be appropriate in some clinical situations.31 As there are no data on patient frailty in the cancer registry, we cannot comment on the just or unjust allocation of treatment. As elderly patients are also generally underrepresented in cancer trials, this compromises the generalizability of the effectiveness of sarcoma treatments to this age group, and future efforts should identify methods to improve low accrual 44 Survival in young and elderly soft-tissue sarcoma patients rates of the elderly in clinical cancer trials or explore other research designs to study the elderly.13,36 The results of this study are based on data from the cancer registry, used in order to gain insight into the disease and discover differences in treatment and survival for different age groups. Histopathological diagnosis and grade are most important for individual, customized therapy and require a central pathology review for optimal histopathological diagnosis and tumor grading. A study comparing primary diagnosis and systematic review by expert showed that 46% of diagnoses were modified at second reading and that in 19% of cases there was a discordance in the histological type.37 Although grade was demonstrated to be the predominant prognostic factor in STS and there is a reproducible histopathological grading system, it often remained unmentioned in the primary pathology report.18 Accurate reports in the medical records on diagnosis, staging, treatment and follow-up details are essential for reliable registration and analysis. Efforts to improve and facilitate registration are made continuously by the cancer registry and checklists for standardized pathology reporting of STS are becoming more and more available.38 Fortunately, a promising trend has been observed in recent years, with more accurate and less missing data. Furthermore, adequate staging is necessary but a complete investigation for distant metastases is not always performed, especially when small STS are completely excised without preoperative suspicion of this diagnosis (the so-called “whoops” operation) and no further treatment is needed, or when advanced STS are diagnosed in fragile patients who abandon further staging or treatment. Strikingly, in contrast to most other types of cancer and despite continuous efforts to improve sarcoma treatment, more individual customized therapy, relatively new treatment modalities (like hyperthermic isolated limb perfusion for locally advanced STS of the extremity) and better compliance with guidelines, other series show that survival rates have not improved over time for all age groups.39 Further research is thus extremely important to discover the gaps in sarcoma treatment and find out the areas accessible for improvement. Currently research efforts are directed at molecular pathways in the various sarcoma subtypes and the development of new targeted therapies.27,40 Conclusions Studies on soft-tissue sarcoma care in the elderly are extremely important to gain better insight into treatment and survival differences; the current norm of individual, customized sarcoma treatment also applies to elderly ESTS patients. 45 3 Different distribution of sarcomas, more high-grade sarcomas and a higher stage at diagnosis, less aggressive treatment and lower survival of the elderly urge the need for optimizing sarcoma care and improving survival rates among the elderly. References 1. Cancer Incidence in the Netherlands. 2013. Ref Type: Internet Communication 2. Nijhuis PH, Schaapveld M, Otter R et al. Epidemiological aspects of soft tissue sarcomas (STS)--consequences for the design of clinical STS trials. Eur J Cancer 1999; 35:1705-1710. 3. Zagars GK, Ballo MT, Pisters PW et al. Prognostic factors for patients with localized softtissue sarcoma treated with conservation surgery and radiation therapy: an analysis of 1225 patients. Cancer 2003; 97:2530-2543. 4. ten Heuvel SE, Hoekstra HJ, van Ginkel RJ et al. Clinicopathologic prognostic factors in myxoid liposarcoma: a retrospective study of 49 patients with long-term follow-up. Ann Surg Oncol 2007; 14:222-229. 5. Pautier P, Genestie C, Rey A et al. Analysis of clinicopathologic prognostic factors for 157 uterine sarcomas and evaluation of a grading score validated for soft tissue sarcoma. Cancer 2000; 88:1425-1431. 6. Brooks AD, Bowne WB, Delgado R et al. Soft tissue sarcomas of the groin: diagnosis, management, and prognosis. J Am Coll Surg 2001; 193:130-136. 7. Pisters PW, Leung DH, Woodruff J et al. Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol 1996; 14:1679-1689. 8. LeVay J, O’Sullivan B, Catton C et al. Outcome and prognostic factors in soft tissue sarcoma in the adult. Int J Radiat Oncol Biol Phys 1993; 27:1091-1099. 9. Parsons HM, Habermann EB, Tuttle TM et al. Conditional survival of extremity soft-tissue sarcoma: results beyond the staging system. Cancer 2011; 117:1055-1060. 10. Nijhuis PH, Schaapveld M, Otter R et al. Soft tissue sarcoma--compliance with guidelines. Cancer 2001; 91:2186-2195. 11. Levi F, La Vecchia C, Randimbison L et al. Descriptive epidemiology of soft tissue sarcomas in Vaud, Switzerland. Eur J Cancer 1999; 35:1711-1716. 12. Farshadpour F, Schaapveld M, Suurmeijer AJ et al. Soft tissue sarcoma: why not treated? Crit Rev Oncol Hematol 2005; 54:77-83. 13. Hutchins LF, Unger JM, Crowley JJ et al. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N Engl J Med 1999; 341:2061-2067. 14. Hoekstra HJ, Thijssens K, van Ginkel RJ. Role of surgery as primary treatment and as intervention in the multidisciplinary treatment of soft tissue sarcoma. Ann Oncol 2004; 15 Suppl 4:iv181-iv186. 15. Thijssens KM, van Ginkel RJ, Pras E et al. Isolated limb perfusion with tumor necrosis factor alpha and melphalan for locally advanced soft tissue sarcoma: the value of adjuvant radiotherapy. Ann Surg Oncol 2006; 13:518-524. 16. Yang JC, Chang AE, Baker AR et al. Randomized prospective study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of the extremity. J Clin Oncol 1998; 16:197-203. 17. Edge SB, Byrd DR, Compton CC et al. (eds). AJCC Cancer Staging Manual. New York: Springer; 2010. 46 Survival in young and elderly soft-tissue sarcoma patients 18. Coindre JM, Trojani M, Contesso G et al. Reproducibility of a histopathologic grading system for adult soft tissue sarcoma. Cancer 1986; 58:306-309. 19. WHO Classification of Soft Tissue Tumours. http://www.iarc.fr/en/publications/pdfsonline/pat-gen/bb5/bb5-classifsofttissue.pdf. 2012 20. Nur U, Shack LG, Rachet B et al. Modelling relative survival in the presence of incomplete data: a tutorial. Int J Epidemiol 2010; 39:118-128. 21. Boden RA, Clark MA, Neuhaus SJ et al. Surgical management of soft tissue sarcoma in patients over 80 years. Eur J Surg Oncol 2006; 32:1154-1158. 22. Lahat G, Dhuka AR, Lahat S et al. Complete soft tissue sarcoma resection is a viable treatment option for select elderly patients. Ann Surg Oncol 2009; 16:2579-2586. 23. Al-Refaie WB, Habermann EB, Dudeja V et al. Extremity soft tissue sarcoma care in the elderly: insights into the generalizability of NCI Cancer Trials. Ann Surg Oncol 2010; 17:1732-1738. 24. Gutierrez JC, Perez EA, Franceschi D et al. Outcomes for soft-tissue sarcoma in 8249 cases from a large state cancer registry. J Surg Res 2007; 141:105-114. 25. Marusyk A, DeGregori J. Declining cellular fitness with age promotes cancer initiation by selecting for adaptive oncogenic mutations. Biochim Biophys Acta 2008; 1785:1-11. 26. Dunn GP, Bruce AT, Ikeda H et al. Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol 2002; 3:991-998. 27. Verweij J, Baker LH. Future treatment of soft tissue sarcomas will be driven by histological subtype and molecular aberrations. Eur J Cancer 2010; 46:863-868. 28. Ducimetière F, Lurkin A, Ranchère-Vince D et al. Incidence of sarcoma histotypes and molecular subtypes in a prospective epidemiological study with central pathology review and molecular testing. PLoS One 2011; 6:e20294. 29. Mendenhall WM, Indelicato DJ, Scarborough MT et al. The management of adult soft tissue sarcomas. Am J Clin Oncol 2009; 32:436-442. 30. Biau DJ, Ferguson PC, Turcotte RE et al. Adverse effect of older age on the recurrence of soft tissue sarcoma of the extremities and trunk. J Clin Oncol 2011; 29:4029-4035. 31. Al-Refaie WB, Habermann EB, Jensen EH et al. Surgery alone is adequate treatment for early stage soft tissue sarcoma of the extremity. Br J Surg 2010; 97:707-713. 32. Buchner M, Bernd L, Zahlten-Hinguranage A et al. Primary malignant tumours of bone and soft tissue in the elderly. Eur J Surg Oncol 2004; 30:877-883. 33. Carreca I, Balducci L, Extermann M. Cancer in the older person. Cancer Treat Rev 2005; 31:380-402. 34. Horton JK, Gleason JF Jr., Klepin HD et al. Age-related disparities in the use of radiotherapy for treatment of localized soft tissue sarcoma. Cancer 2011; 117:4033-4040. 35. Chen H, Cantor A, Meyer J et al. Can older cancer patients tolerate chemotherapy? A prospective pilot study. Cancer 2003; 97:1107-1114. 36. Murthy VH, Krumholz HM, Gross CP. Participation in cancer clinical trials: race-, sex-, and age-based disparities. JAMA 2004; 291:2720-2726. 37. Lurkin A, Ducimetière F, Vince DR et al. Epidemiological evaluation of concordance between initial diagnosis and central pathology review in a comprehensive and prospective series of sarcoma patients in the Rhone-Alpes region. BMC Cancer 2010; 10:150. 38. Recommendations for the reporting of soft tissue sarcoma. Association of Directors of Anatomic and Surgical Pathology. Virchows Arch 1999; 434:187-191. 39. Weitz J, Antonescu CR, Brennan MF. Localized extremity soft tissue sarcoma: improved knowledge with unchanged survival over time. J Clin Oncol 2003; 21:2719-2725. 40. Wunder JS, Nielsen TO, Maki RG et al. Opportunities for improving the therapeutic ratio for patients with sarcoma. Lancet Oncol 2007; 8:513-524. 47 3 Attachment 1: Univariate analysis Relative Survival (RS) Univariate analysis 5-year RS RER (95%CI) p-value Age (years) < 65 65-69 70-74 75-79 80-84 85+ 73 (73-74) 68 (65-70) 59 (56-62) 60 (56-63) 55 (50-60) 46 (39-54) 1 (ref ) 1.3 (1.0-1.6) 1.8 (1.4-2.2) 1.9 (1.5-2.4) 2.0 (1.5-2.7) 3.0 (2.2-4.0) < 0.001 Sex Male Female 70 (69-71) 67 (66-68) 1 (ref ) 1.1 (1.0-1.3) 0.2 Period 1989-1993 1994-1998 1999-2003 2004-2008 67 (65-69) 69 (67-71) 68 (66-70) 71 (69-73) 1 (ref ) 1.0 (0.8-1.2) 1.0 (0.8-1.2) 0.9 (0.8-1.2) 0.9 Grade Low High 89 (88-90) 61 (60-62) 1 (ref ) 4.2 (3.1-5.7) < 0.001 Stage I II III IV < 0.001 92 (91-93) 1 (ref ) 76 (74-77) 3.0 (1.6-5.9) 60 (58-62) 5.8 (2.6-12.6) 29 (27-31) 16.4 (9.0-29.8) Morphology Dedifferentiated liposarcoma Myxoid & round cell liposarcoma Pleomorphic liposarcoma Mixed-type liposarcoma Fibrosarcoma Pleomorphic undifferentiated sarcoma Leiomyosarcoma Rhabdomyosarcoma Angiosarcoma Synovial sarcoma MPNST, malignant peripheral nerve sheath tumor Other 53 (41-65) 88 (86-90) 61 (56-67) 92 (84-97) 85 (83-88) 1.1 (0.5-2.5) 0.3 (0.2-0.4) 0.9 (0.6-1.3) 0.3 (0.1-0.8) 0.3 (0.2-0.5) 59 (58-61) 67 (65-69) 47 (41-52) 37 (30-44) 61 (58-64) 1 (ref ) 0.7 (0.6-0.9) 1.6 (1.1-2.2) 2.1 (1.4-3.1) 0.9 (0.7-1.1) 56 (50-61) 82 (79-84) 1.3 (0.9-1.8) 0.5 (0.4-0.6) Treatment 18 (15-21) 78 (77-79) 15 (10-21) 20 (17-24) 44 (40-48) 75 (74-77) 55 (50-59) 34 (24-44) 1 (ref ) 0.1 (0.1-0.1) 1.0 (0.7-1.5) 0.6 (0.4-0.7) 0.3 (0.2-0.4) 0.1 (0.1-0.1) 0.2 (0.1-0.3) 0.4 (0.2-0.8) No treatment Surgery (monotherapy) Radiotherapy (monotherapy) Chemotherapy (monotherapy) Surgery & chemotherapy (CT) Surgery & radiotherapy (RT) Surgery & RT & CT Chemotherapy & radiotherapy < 0.001 < 0.001 157