Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
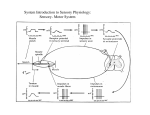
Clinical Pathways for Successful Orthotic Therapy Contracture Management John Kenney, BOCO Clinical Pathway to Orthotic Therapy Success 1. 2. 3. Comprehensive assessment of joint pathology & rehab potential Setting realistic therapy goals based upon in depth assessment Selecting the most appropriate orthotic therapy to achieve rehabilitation objectives RA, RSD, Severe OA = Static Therapy Where disease significantly limits use, support, protect, and correctly position the joint(s) to relieve pain, reduce inflammation, and prevent further joint deformity. Where therapeutic stretch is contraindicated for any reason. Must be light, comfortable, and able to be easily modified as the “position of comfort” may need to be changed frequently. Bend to fit in all planes (i.e., ulnar) Use SoftPro™ “Bend to Fit” Orthotics RA Hands RA w/ Ulnar Drift – Wrist -35°; Thumb Adduction – Support & Position Static Bracing Static orthotics are most appropriate for support, protection, and positioning of the joint(s) Orthotic type of choice where therapeutic stretch is contraindicated for any reason Brace of choice for optimizing limb positioning; provides positioning therapy. Adaptive Tissue Shortening Connective tissue, tendons, and muscles adapt to immobility by shortening and thickening Bio-mechanical changes in tissue occur over time with a significant loss of tissue elasticity Shortening and loss of elasticity can be reversed if the contracture is not “fixed” or ankylosed 10˚ of joint movement indicates joint is likely not ankylosed Strategy for Treatment Tissue shortening: create demand to lengthen connective tissue, tendons and muscle Muscle length will adapt to daily demands for muscle length Use manual techniques, modalities, and appropriate bracing to create muscle lengthening. Brace should initiate gentle stretch to tissue (AirPro. DynaPro) Muscle Fiber - Myofibril Sarcomere Muscle Shortening Sarcomeres at either end of the myofibrils fall off if not needed Muscle length depends on demands placed on the muscle Muscle length is constantly adapting depending on need Rehabilitation should include strategies to re-lengthen muscle Muscle Elasticity Loss of glycogen in muscle: addition of lactic acid = reduced ability to work and sore limbs Decreased ATP reduces elasticity efficiency Approximately 7% of water content is lost in 30 days of immobility Muscle becomes relatively inelastic Treatment Strategy Improve elasticity of tissue by significantly increasing cellular metabolism (biological activity) Use manual techniques (activity), modalities, and therapeutic bracing to rehabilitate tissue (therapeutic tension) Muscle Growth / Elongation Muscle protein is continuously recycled with a half life of 7 to 15 days. Muscle can easily adapt to a change in conditions due to new demands or a lack of demand. The rate of protein synthesis in muscles can be increased by stimulating muscle growth or exercise. Therapeutic stretch is one very important factor is reversing tissue shortening Stretch must be held for 1 hour or more to have a “carry over” effect. Treatment Expectations Need a minimum of 15 treatments over 30 days to see significant improvement Expect 5 to 8° improvement in 30 days w/ Low Load prolonged Stretch bracing alone. Double expected outcome w routine modality use (10 to 16°) Do “elasticity” test and goniometer measurements weekly to chart progress Treatment Focus Stimulate biological activity to the affected tissue to improve elasticity Incrementally improve cellular equilibrium – increase water content; increase glycogen in tissue Add sarcomeres to increase muscle length w/ positioning & prolonged stretch w/ brace Increase protein synthesis to recycle poor muscle with healthier muscle tissue Improve tissue elasticity Lay down new healthy collagen Neurological Contracture Usually related to upper motor neuron (brain) dysfunction or injury Results in disruption of inhibitory pathway from the brain Limb becomes movement sensitive (rate & degree of stretch) Hypertonicity and frequent occurrence of episodes of tone can significantly limit functional use of the affected limb(s) Motor Control Alpha motor system: Volitional movement Gamma motor system: Tone, proprioception and coordination Muscle Spindle Senses muscle length Senses velocity of change in muscle length Initiates muscle contraction Stretch Reflex Contraction of a muscle in an attempt to resist a change in muscle length Golgi Tendon Organ Senses muscle tension Initiates muscle inhibition Gentle tension initiated by a brace can have an inhibiting effect on the joint Neuro-Rehabilitation Strategy Re-Activate GTO’s – NeuroStretch PROM – Non Thermal Ultasound over GTO’s – Nerve block e-stim – Electro-acupuncture – Static Flex Orthotics, Air Orthotics Stimulate GTO / Muscle Spindle Communication – Movement therapy – PENS – Static Flex Orthotics, Air Orthotics Neuro Contractures Neuro contractures may be “mixed”, meaning that there is neurological opposition to stretch and adaptive tissue shortening End range post stretch is less than full range indicating tissue shortening Must treat neurological dysfunction first; tissue shortening after spasticity is managed Stretch Reflex Implications Traditional ROM techniques may be ineffective and painful Normal passive ROM may facilitate muscular contraction via the stretch reflex Passive ROM is best obtained by encouraging muscle inhibition and avoiding the stretch reflex when applying device New Neuro-Rehab Paradigm Constraint Induced Therapy (Taub) Modified Constraint Induced Therapy (Levine) Robot Assisted Therapy (MIT) Massed practice leads to functional recovery years after CVA or TBI Joint Assessment Neurostretch An Alternative Passive Range of Motion & Joint Assessment Technique NeuroStretch as an Assessment Tool Palpation the Joint for Structural Changes in End Feel Evaluation – Elasticity Check Tonal Assessment – determine degree of abnormal tone or spasticity PROM Objective for Neuro- Contractures Avoid Stretch Reflex during PROM PROM is completed comfortably for patient Manipulated joint is relaxed and remains extended post PROM Improved joint positioning post PROM NeuroStretchTM Technique Begin with the joint in a relaxed position Give 90 seconds of manual joint stimulation at the acupressure point Slowly move joint to point of resistance Hold joint at sub maximal stretch until release End Feel Assessment Check “play” at relaxed end range post NeuroStretch May need to continue stimulating NS point(s) while assessing end feel Compare to unaffected side if possible; evaluate relative to unaffected side List as poor, fair, good, or excellent and measure w/ goniometer NeuroStretch - Shoulder Proximal to Distal NeuroStretch - Elbow NeuroStrech - Wrist / Hand NeuroStretch - Post Stretch Application of Orthotic Two Hours Later - Post Orthotic Therapy NeuroStretch - Lower Extremity NeuroStretch - Knee Submaximal Stretch Application of Orthotic NeuroStretch Lab End Feel & Tonal Assessment Orthotic Therapy Goals Support & protect: stop further declines in LROM; support and protect the joint from further injury/deformity; reduce pain & discomfort; reduce the risk of more serious problems (pressure sores) Restoration of LROM: achieve incremental permanent lengthening of the connective tissue, tendons, and muscles to restore joint range of motion; provide neuro-rehabilitation by managing spasticity Orthotic Selection Joint pathology and rehabilitation goals drive orthotic brace selection Orthotic braces are designed to provide specific types of therapy Matching the type of therapy provided by the brace to joint pathology and the rehabilitation objectives results in the optimal patient outcome Types of Orthotic Braces & Therapy Provided by Brace Type Static: protect, support, and position joint or provide progressive extension stretching ROM: 2 stop hinge for controlled range of motion therapy in the brace; controlled movement and support in brace for ambulation support (orthopedic indications) Air Bladder: gentle Low Load Prolonged Stretch Dynamic: spring loaded Low Load Prolonged Stretch (LLPS); creep therapy Static/Neuro-Dynamic: flexible static brace w/ dynamic LLPS and neuro-inhibiting properties Clinical Pathways to Orthotic Success – Non-Orthopedic Joint Pathology / Rehab Objective stretch not indicated / desired stretch therapeutic Support & Position Joint(s) Restore LROM Good = Progress. Extension Better = Air Bladder Stretch Best = Dynamic LLPS Benefits of Static Orthotic Therapy Pain & discomfort due to contracture can be significantly reduced Improved joint alignment w/o brace use Joint is protected from further injury and additional LROM w/ daily use Skin integrity issues can be managed more effectively Improved quality of life Full Contact End Range Static Fit Rehab Therapy Bracing Most important time to use a therapeutic brace is immediately after therapy treatment Joint mobilization therapy; heat, and use of modalities significantly improve joint elasticity Treatment improvement is significantly improved w/”carry over” when post treatment lengthening is held for 1 hour or more w/ a brace Restorative Orthotic Therapy 1. 2. 3. Fair to good end feel indicates that there is the potential to restore ROM with treatment Progressive Extension static orthotic therapy provides the most conservative restorative therapy; frequent modification of the device is required. GOOD Air Bladder Low Load Prolonged Stretch provides adjustable gentle stretch which is very appropriate for adaptive tissue shortening contractures, especially is LROM is severe. BETTER Dynamic Low Load Prolonged Stretch provides the best option for restored LROM by providing more clinically effective stretch; brace usually requires significantly less frequent modification compared to progressive extension braces (dynamic or static/dynamic orthotic technology). BEST Elastic Stretch Force is applied to the tissue, then released When the force is removed, the tissue returns to its original length Plastic Deformation Elongation of tissue produced under loading that will remain after the removal of a load. Tissue undergoing plastic deformation will remain stretched, yielding a permanent increase in length Stress – Relaxation Phenomena When a gentle tension or stress is applied to a muscle that does not risk injury to the muscle, the muscle will adapt, and “relax” or elongate as opposed to opposing the gentle stress or stretch. This phenomena (relaxed elongation) will usually occur within several minutes of applying the gentle stress. Progressive Extension Fitting Set angle of static brace progressively ahead of end range by 5° to 10° Elongation of tissue after the stress – relax phenomena can be 5° to 8° Use adjustable elastic leverage strap to initiate gentle tension into joint, applying a therapeutic stretch Progressive Extension orthotic therapy; conservative stretch therapy. Clinical Pathways to Success LROM Rehabilitation Restore LROM w/ Therapeutic Stretch (no - mild stasticity) Maintain Stretch from Therapy Good Low Load Prolonged Stretch Better Low Load Prolonged Stretch Best Low Load Prolonged Stretch Best Progressive Extension Air Bladder Static / Dynamic Spring loaded dynamic braces SoftPro™ AirPro™ DynaPro™ Low Load Prolonged Stretch (LLPS) A low load tension is delivered by a brace to a joint that when maintained for a prolonged period results in permanent elongation of the affected tissue. LLPS Brace Fitting The brace initiates a therapeutic stretch to the shortened tissue to permanently elongate or lengthen the tissue. After the stress-relaxation release of tissue, the brace maintains stretch Prolonged Stretch = 3 to 6 hours / day Low Load Prolonged Stretch therapy is the optimal therapy to reverse tissue shortening Low Load Prolonged Stretch Bracing Options Air Technology: usually most gentle stretch, ideal for severe contracture of 90° or more. Static–Flex: bio-engineered dynamic stretch; very effective for tissue shortening or neuro contractures. Must be modified every 4 – 6 weeks for best results. Dynamic: best for post surgical tissue shortening; constant linear tension can be effectively used for neuro contractures. Very little modifications required. DME, so not allowed in nursing homes. AirPro Orthotics Use of pneumatic air bladders to provide a gentle Low Load Prolonged Stretch to the shortened tissue Appropriate for spasticity treatment as air “gives” during episode of tone Recommended 90° or more for contractures of Static – Dynamic Braces DynaPro™ braces are static but flexible braces that have dynamic properties. Tension is adjusted by setting the brace “ahead” of end range (15°) The brace flexes into the contracture to provide dynamic Low Load Prolonged Stretch Static/Neuro-Dynamic Orthotics Static braces fabricated from flexible materials (no springs) with dynamic LLPS properties Brace is set to “flex” into the LROM to provide a dynamic stretch (+15°) Dynamic tension initiates inhibition Bio-engineered to “give” or reduce stretch force on the joint w/ involuntary muscle contraction; ideal for spasticity DynaPro™ Orthotics Brace will flex or “give” w/ dynamic stretch reflex to accommodate spasticity Bioengineered to reduce tension or flex force with a dynamic muscle contraction Best option for severe spasticity due to negative tension dynamics Case Study: Lateral Neck Flexion Contracture Immediately Post Fit 10 Minutes Post Fit 30 Minutes Post Fit CP Severe WHF Spasticity Post DynaPro Fit Palpation Method of Orthotic Fitting Evaluation of Stress – Relaxation Release Palpate Stretched Tissue to Assess Fit IMMEDIATELY post fit, palpate the stretched tissue to assess the stretch Stretched Patient tendons should be taut should feel “stretch”, but no discomfort or pain Re-Palpate 5 to 10 Minutes Post Fit Fitter must re-palpate stretched joint 5 to 10 minutes post fit at crease in elbow (bicep tendon) to confirm stress-relax phenomena indicating brace is holding relaxed tissue at optimal resting length Tendons should demonstrate significant softening or improved pliability Adjust fit as necessary Device should be worn 3 to 6 hours per day for best results Design Selection Criteria Brace must deliver three point leverage stretch to each affected joint. Middle “lever” should have elastic properties. Strapping should align with the apex of each affected joint (i.e., wrist, MCP’s of fingers & thumb). Optional finger straps may be necessary to optimize WHFO therapy. 3 Point Leverage Stretch to Correct Wrist Flexion Upwards leverage point on forearm Upwards leverage point in palm of hand Downwards adjustable elastic leverage point at apex of wrist 3 point leverage = adjustable stretch at wrist w/ 5° to 10° of stretch Setting the Wrist Strap Secure the forearm strap first to position the wrist/hand/finger brace Secure the hand / finger strap w/ the thumb properly aligned to hold the hand / fingers in place Pull the wrist strap “up” at the wrist, stretching the wrist strap. Wrap the wrist strap around the wrist and secure. Wrist strap should provide a gentle downwards force on the wrist Wrist Palpation – Flexion Contracture Brace is set straighter than wrist at all affected joints Finger should easily fit under wrist and over brace if fit correctly Wrist strap adjusts stretch tension MCP strap adjusts MCP tension Optional Ulnar Drift Strap may be needed for PIP stretch Wrist Palpation – Flexion Contracture Palpate tendons at crease in the wrist joint Initially, tendons should be taut 5 to 10 minutes post fit, tendons are slightly softer and more pliable Adjust brace as necessary Finger Palpation Fingers will initially oppose shape of brace set “ahead” of comfortable end range 10 mins. post fit, fingers should be relaxed, often move beyond end stretch Elbow 3 Point Leverage Downwards leverage point on bicep Downwards leverage point on forearm Upwards adjustable leverage point at elbow cap 3 point leverage = adjustable stretch at elbow w/ 5° to 10° of stretch Elbow 3 Point Leverage Adjustable gel/foam elbow cap brings the elbow up into the brace when tightened Bicep cuff, forearm cuff and elbow cap provide a 3 pt. leverage stretch of the elbow Center elbow cap; snug up all 4 straps to bring elbow up into brace Elbow Palpation - Flexion Contracture Palpate biceps tendon at crease in the joint immediately post fit to check applied stretch Initially, bicep tendon should be taut Elbow Palpation – 10 Mins.Post Fit 5 to 10 minutes post fit tendon and surrounding tissue is significantly softer and more pliable Hip Abduction Anatomical exception to 3 pt. leverage rule Minimizing pressure thru = distribution key in static or pro ex fit Thigh cuffs must rotate or have gel to accommodate changes in abduction setting Ease of application and adjustment important Hip Palpation Palpate hip adductors on both legs immediately post fit Muscle stretch should be apparent Re-palpate after 10 mins.; muscles should be more pliable Knee 3 Point Leverage Upwards leverage point on back of thigh Upwards leverage point on calf Downwards adjustable leverage point at knee cap; center knee cap, then snug up all straps 3 point leverage = adjustable stretch at knee w/ 5° to 10° of stretch Knee Palpation - Flexion Contracture Palpate medial hamstring on the medial crease in the joint immediately post fit Initially, tendon should be taut 5 to 10 minutes post fit, medial hamstring and surrounding tissue is softer and more pliable Ankle / Foot 3 Point Leverage Upwards leverage point on bottom of foot Upwards leverage point on calf Downwards adjustable leverage point at anterior bend in the ankle 3 point leverage = adjustable stretch at knee w/ 5° to 10° of stretch Ankle / Foot 3 Point Leverage Ankle/Foot Palpation - Plantarflexion Palpate tissue between malleolus and Achilles tendon on both sides of the ankle (soft spot unstretched) Initially, tissue should feel stretched or taut Re-Palpate 5 to 10 Minutes Post Fit Fitter must re-palpate stretched joint 5 to 10 minutes post fit Tissue should demonstrate significant softening or improved pliability Adjust fit as necessary Questions