Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
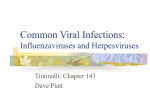
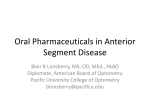
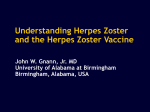
Volume 2 Issue 1 February 2011 Herpes Zoster Case report Herpes zoster along Maxillary Nerve with Osteonecrosis Dr K.R.Kashinath1, Dr.Chandra Shekar.L2 1 Prof. & HOD, Dept of Prosthodontics, 2Senior Lecturer, Dept of oral medicine and Radiology, Sri Siddhartha Dental College, Tumkur. Abstract Herpes zoster (HZ) presents as a cutaneous vesicular eruption in the area innervated by the affected sensory nerve, usually associated with severe pain. Oral manifestations of HZ appear when the mandibular or maxillary divisions of the trigeminal nerve are affected. A case, of zoster involving the maxillary nerve with oseto necrosis of the maxilla is described. Keywords: Maxilla, Osteonecrosis, Tooth exfoliation, Varicella zoster Journal of Dental Sciences & Research 2:1: Pages 12-17 with circulating varicella antibodies Introduction: Zoster is a common, develop a localized zoster.1 and Zoster probably results most neurologic disorder caused by the often from a failure of the immune varicella-zoster virus (VZV), a virus system to contain latent varicella- morphologically and antigenically zoster virus replication. Whether identical other factors such as radiation, predominantly to dermal, the virus causing varicella (chickenpox). Difference physical in clinical manifestations between medications, other infections, or varicella stress also can trigger zoster has and zoster apparently trauma, depends on the immune status of not individual patients; those with no certainty. Nor is it entirely clear prior why circulating varicella antibodies immunologic varicella children, virus, exposure most develop to commonly the clinical syndrome of varicella, while those and been cell-mediated mechanisms recurrent 12 Journal of Dental Sciences and Research determined certain do overt not disease, with immune prevent as is Volume 2 Issue 1 February 2011 Herpes Zoster common with most other On examination extra orally viral 1 illnesses. scarring and pigmentation was Pathophysiology seen on right cheek region one commonly centimetre below the lower eye lid manifests in 1 or more posterior spreading inferiorly towards the ala spinal ganglia or cranial sensory of the right nose and commissure ganglia, presumably because viral of the right lip, superolaterally a particles scar was also seen on right temple Zoster most have been preserved within these ganglia in a dormant region (fig-1a &1b). state since the original episode of varicella. This results in pain and characteristic cutaneous findings along the corresponding sensory dermatomes of the involved Fig -1a On ganglia. Less often, involvement of Fig-1b intra oral examination anterior and posterior horn cells, open tooth socket with respect to leptomeninges, 13 nerves is and peripheral observed, with tooth region (fig -2) and exposed alveolar bone with respect consequent muscle weakness or to palsy, pleocytosis of spinal fluid, receded and/or with respect to 14,15,16 (fig -3) sensory loss. Rarely, myelitis, meningitis, encephalitis, or visceral involvement 14,15,16 region palatal along gingival with margin was seen. may occur.1,2,3,4 Case report: A 58-year-old male Fig -2 Fig -3 presented to the Oral medicine Department with complaints of pain and exfoliation of the upper right front teeth since two days . On enquiry patient gave history of severe pain along with vesicular eruptions over the right cheek for 12 days. Eruptions were 13 Journal of Dental Sciences and Research Volume 2 Issue 1 February 2011 Herpes Zoster noted in successive crops over the right cheek, side of the nose, upper lip and temple. Eruptions were heralded by mild fever, malaise, Fig -4 and piercing pain over the right Intra cheek for initial two days. The vesicles were followed by pain in the right upper teeth with difficulty in chewing, on consultation with a dermatologist vesicular the pain eruptions and oral radiograph periapical showed sever destruction of the alveolar bone extending to 11 mesially and 14 distally with missing 12,13 (fig -5). reduced gradually and later he was referred to the dentist with a clinical diagnosis of herpes zoster along Fig -5 the neural distribution of the right Discussion: maxillary nerve. Zoster The patient was treated with may begin systemic day for seven days, supplemented anorexia, and lassitude, although by non- symptoms frequently are mild and anti-inflammatory may not be associated by either steroidal B1-B6-B12, analgesics along application of eg, a oral acyclovir 800 mg. five times a injection response, with fever, local patient or physician with the classic ciprofloxacin zoster signs and symptoms that with ointment 0.3% over the vesicles. On radiographic examination follow. Symptoms typically include prodromal sensory phenomena panoramic image showed missing along 1 or more skin dermatomes 12, 13 and severe alveolar bone lasting 1-10 days (averaging 48 h), destruction in the 12, 13 region which usually are noted as pain or, (fig -4). rarely, pain paresthesias. typically is Prodromal described as muscle or toothache like in origin 14 Journal of Dental Sciences and Research Volume 2 Issue 1 February 2011 Herpes Zoster Unfortunately, resolution of but may simulate headache, iritis, pleurisy, brachial neuritis, cardiac the pain, always accompany appendicitis or other associated pain does not resolution of intraabdominal disease, or sciatica, erythema and vesiculation. PHN, which which usually is confined to the can result in incorrect tentative diagnoses. The prodromal area interval of pain prior to onset of involvement, can persist for weeks, cutaneous been months, or years and often is believed to represent spread of severe. The reason some patients viral with findings particles has along sensory of original zoster, dermatomal and not others, approximately experience PHN is not understood 10% of patients report onset of fully, but patients who are older pain and rash simultaneously. After (>60 y), particularly patients who the onset of prodromal symptoms, are debilitated or arteriosclerotic, the following signs and symptoms are affected far more frequently occur: than patients who are younger. 1, 2 nerves; however, Patchy erythema, occasionally accompanied indurations, appears in In addition, PHN is observed by the more frequently after cases of dermatome area of involvement. herpes zoster ophthalmicus and in Regional lymphadenopathy instances appear at this stage may or of dermatomal upper body involvement. Other subsequently. The classic finding of less common postherpetic sequelae grouped include herpetiform vesicles hyperesthesia, or more develops upon the erythematous rarely, hypesthesia or anesthesia in base. the area of involvement. usually At this has inflammation point, induced of the the virus significant involved 1, 2 Zoster of the maxillary branch of the fifth CN (CN V2): Involvement is sensory nerve causing severe pain, localized to the ipsilateral cheek, stopping abruptly at the midline of lower eyelid, side of the nose, the limit of sensory coverage of the upper eyelid, upper involved dermatome.1, 2 mucous membrane of the nose, 15 Journal of Dental Sciences and Research teeth, and Volume 2 Issue 1 February 2011 Herpes Zoster nasopharynx, tonsils, and roof of trigeminal nerve involvement that the mouth. In our case similar led to a rapid loss of alveolar bone findings were found along with and exfoliation of two teeth, the severe the initial intraoral examination showed alveolar bone along with exfoliation redness of the alveolar mucosa and 13. gingiva of the lower right quadrant osteonecrosis of At times, only the oral mucus with multiple well-delimited and membrane is involved without skin painful erosive lesions affecting the manifestations. Early pre-eruptive attached gingiva around the teeth. herpetic pain can simulate a severe Two weeks later, teeth number 43 toothache in (lower right canine) and 44 (lower unnecessary oral surgery or dental right first premolar) had class III treatment. It is very unusual for mobility, flow of purulent exudate zoster from the gingival sulcus, and deep and to result involve mandibular maxillary nerve ophthalmic division or without involvement which was seen in our case.5 segment with of necrosis mandibular (>11 radiological advanced A case of 76-year-old man presenting pockets of a alveolar mm). examination alveolar The showed bone loss around both teeth. The prognosis for teeth number 27 and 28 was considered hopeless, and they bone and spontaneous exfoliation were extracted7 , which was similar of the corresponding teeth 1 month to our case except the involvement after of maxilla and exfoliation of the acute varicella zoster infection of the mandibular branch of the reported trigeminal in Japan6, nerve was which was teeth. In a extensive south African osteonecrosis study and similar to our case except the exfoliation of teeth in the area involvement innervated by the nerve affected of maxilla and exfoliation of teeth within 15 days by HZ In sero positives8, but in another woman with case HZ 63-year-old infection with 16 Journal of Dental Sciences and Research was more common in HIV our case Volume 2 Issue 1 February 2011 Herpes Zoster exfoliation of teeth was seen in HIV recrudescence of sero negative.. infection. Postgrad VZ virus Med J. Nov 1970; 46(541):653-8. Conclusion: 5. Extensive osteonecrosis and Jarrett WH. Horner's syndrome with geniculate zoster: exfoliation of teeth in the area Occuring in innervated by the nerve affected trigeminal herpes by HZ has been reported after HZ ophthalmic division infection. Am J Ophthalmol 1967;63: 326- Clinicians should be aware of this possible outcome association in with which the was spared. 30. after a trigeminal HZ infection. 6. Alveolar Osteonecrosis of the Mandible References: after Varicella Zoster Infection of the Trigeminal Nerve 1. Edgerton ophthalmicus: G. Herpes a review zoster of the Asian J Oral Maxillofac Surg. 2004; 16:204-208. literature. Arch Ophthalmol. 1945; 7. 34:40-62; 114-53. Alveolar bone necrosis and tooth exfoliation following herpes 2. Barker B. Herpes review. Arch zoster Dermatol Syphil. 1939;40:974 3. zoster infection: a review of the literature and case report. J Periodontol. 2005 Jan;76(1):148- Burgoon CF Jr, Burgoon JS, 53. Baldridge GD. The natural history 8. of spontaneous tooth exfoliation in an herpes zoster. J Am Med Assoc. May 18 1957;164(3):265-9 4. Blank Goldfaden H, Eaglstein GL. Zoster, WH, a Alveolar bone necrosis and HIV-seropositive herpes zoster. Mar;63(2):106-10 17 Journal of Dental Sciences and Research subject with SADJ. 2008