Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
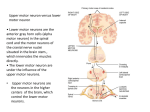
UPPER MOTOR NEURON SYNDROME Aims • Expand the participants’ understanding of upper motor neuron syndrome. • Introduce the application of the concepts of movement as used in the assessment and treatment of adults in the analysis posture and movement. Motor Neuron • Upper motor neuron - cell body lives in a CNS processing center - synapses on the lower motor neuron - activity in upper motor neuron may facilitate or inhibit lower motor neuron • - Lower motor neuron cell body lives in a nucleus of the brain stem or spinal cord triggers a contraction in innervated muscle: destruction of or damage to lower motor neuron eliminates voluntary and reflex control over innervated motor unit Upper Motor Neuron Upper motor neurons are neurons that originate in higher regions of the brain, such as the motor cortex, and synapse on the lower motor neurons to convey descending commands for movement (Mayer 2003) Lower Motor Neuron Lesions Impaired reflex actions -causes flaccidity • atrophy -can grow back • 1 mm a day Amyotrophic Lateral Sclerosis Lou Gehric, July 4, 1939 UMN Syndrome Damage to the descending motor pathways anywhere along this trajectory gives rise to a set of symptoms Upper motor neuron syndrome • Following a brain injury an individual will often have a complex presentation impacting not only on the neuromuscular system but also on the musculoskeletal, sensory-perceptural and cognitive system (Cohon 1999) • The upper motor neuron syndrome encompasses all the dyscontrol characteristics associated with a lesion affecting some or all of the descending motor pathway (Barnes 2001) • Motor dysfunction after UMN lesion is classified into positive and negative signs. (Canning et al. 2004) Negative & Positive Signs Hughlings jackson (1835~1911) UMN Syndrome • Negative signs are those represent a loss of Pre-existing function. • Positive signs relate to secondary changes (Canning et al. 2004) • This classification does not encompass cognitive or Perceptual dysfunction or psychological reaction. UMN Syndromes Negative signs Positive signs Weakness Clonus Fatigue Associated reactions Sensory loss Non-neural changes in muscle Acute hypotonia Spasticity Loss of dexterity Hyperreflexia Weakness - Constitutes a major cause of the patient’s disability. - Reduced neural excitation may cause weakness. - Muscular weakness may cause secondary weakness of neural transmission. - Reduce muscle activation may cause atrophy and change in the muscle fiber population. Weakness Muscle atrophy could be due to • Disuse • Loss of central trophic effects • Neurogenic atrophy Number of motor units reduced post stroke (Hura et al 2000) Muscle length associated with weakness at certain ranges Central Loss of Force Production Loss of central command generate and sustain force. No loss of contractile capacity: not the same as peripheral weakness, myopathy or general weakness (Sahrmann 2002) Compensatory movement patterns Sensation Action ↑ Cognition ↑ Perception ↑ Sensation Sensory Deficits Deficits in awareness, processing and interpretation and kinesthetic memory Fewer attempts at spontaneous movements Altered sense of “weight” of a limb Altered sense of timing and speed Contributes to development of pain Loss of Dexterity - Ability to solve any motor task precisely, quickly, and deftly. - To coordinate muscle activity to meet environmental demands. Fatigue - Many stroke patient suffer from fatigue. - Reduced force production causes an increase in the effort required to move. - Weakness may be another reason for fatigue. Associated Reaction - Is the abnormal muscle activation during moving, be called dyssynergic pattern of movement. - Indicate weak postural control mechanism and loss of the normal balance strategies. - Occur in response to perturbation either intrinsic or extrinsic generation - Can change the muscle type from phasic to tonic. - Promote learned non-use. Definition of spasticity • As…motor disorder characterised by a velocity dependent increase in the tonic stretch reflex(muscle tone) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one component of the upper motor neuron syndrome (Lance 1980) • What is frequently forgotten is that the Lance definition refers to only one component of the UMN syndrome (Ivanhoe & Reistetter 2004) Spasticity Before the 1970’, spasticity was seen as the major contributors to disability. Excessive antagonist activity could not have caused the observed movement abnormality (Dietz et al. 1981, Sahrmann & Norton 1977). Spasticity • Exaggerated stretch reflexes may not be the major cause of established spasticity. • Factors which are thought to contribute to the increased mechanical resistance to movement include reduced tendon compliance and physiological and histochemical change in muscle fiber (Dietz 1992) Spasticity • “Spasticity is a sensori-motor phenomenon related to the integration of the nervous system motor response to sensory input” • “It is related to hypersensitivity of the reflex arc as a result of the loss of descending inhibition” (Ivanhoe & reistetter 2004) Spasticity - Research definition is increment of muscle tone due to hyperexcitability of stretch reflex. - Clinicians definition is much broader, includes the entire UMN syndrome. - Misconception • Hyperactive stretch reflex are cause of excess muscle stiffness and associated movement • But hyperstiffness is often the result of nonreflexive factor : myoplasticity and/or muscle overactivity. Alpha-gamma coactivation New Definition “Disordered sensory-motor control resulting from an UMN lesion presenting as intermittent or sustained involuntary activation of muscles,” SPASM 2005 Mechanism of Hypertonia CNS lesion Reflex hyperexcitability Altered muscle function (eg prolonged shortening) Non-CNS factors (eg immobilization) Hypertonia Altered passive mechanical Properties(contracture) The Neurological Deficits Primary Impairments - Neurological weakness - Muscle activation deficit - Change in tone Secondary Impairments - Altered alignment - Change in muscle length and position - edema - pain Composite Impairment - Clinical hypertonicity (spastic movement disorder) - Altered postural control - Loss of selective movement Chemical Communication Neural Problem Non-Neural Problem Mechanical Impairment IMPAIRMENT Secondary impairment Primary impairment Composite impairment Movement deficits Atypical movement Compensation Primary Impairment • • • • Changes in muscle strength Changes in muscle / postural tone Changes in muscle activation Sensory changes Secondary Impairment • Orthopedic changes in alignment and mobility - Changes in alignment - Changes in joint mobility • Changes in muscle and soft tissue length Composite Impairment (Movement dysfunction) • Movement deficits • Atypical movement • Compensation References • Shumway-Cook & Woollacott: Motor control. 2007 • Janet M.Howel: Neuro-Development Treatment Approach. 2002 • Eric C. Kandel: Principle of neural science. 1999. • Geoffrey Kidd MSc :Understanding Neuromuscular Plasticity.1992. • Dr. Nigel Lawes , Ms Mary lynch-Ellerington: Changing the Nervous System “ From Cell to patient”. 2007. • Bente E. Bassoe Gjelsvik : The Bobath Concept in Adult Neurology • Mary lynch-Ellerington : Bobath course note. 2006,2007,2010 • Mary lynch-Ellerington, Sue Raine : Bobath Concept. 2009