Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
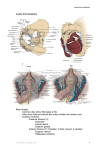
THE ISCHIORECTAL FOSSA LEARNING OBJECTIVES At the end of the lecture the student should be able to: Know the details of ischiorectal fossa Identify the boundaries and recessess of ischiorectal fossa Know the contents of ischiorectal fossa. ISCHIORECTAL FOSSA Wedge shaped spaces between skin of anal region and pelvic diaphragm Base directed downwards to the surface of the perineum Apex at the line of meeting of the obturator and anal fascia 5 to 6 cm deep, anterioposteriorly 5 cm, 2.5 cm side to side Lie below the levator ani muscles and on either side of anal canal ISCHIORECTAL FOSSA Post anal space connects the two fossae posteriorly by a horse shoe path. The space is filled with loose areolar tissue and loosely arranged large loculi of fat. The infection of this space leads to abscess formation and are least painful because swelling can occur without tension. BOUNDARIES Base is formed by the skin. Apex - Is formed by meeting of Obturator fascia with the inferior fascia of the pelvic diaphragm (anal fascia). The line corresponds to the origin of levator ani from the lateral pelvic wall. Anterior wall - The fossa is limited by the posterior border of perineal membrane. Posterior wall- (a) lower border of the gluteus maximus and (b) Sacro tuberous ligament Lateral wall is vertical and is formed by (a) Obturator internus with Obturator fascia, (b) Medial surface of ischial tuberosity below the attachment of Obturator fascia. Medial wall - Slopes upwards and laterally and is formed by (a) External anal sphincter with fascia covering it in the lower part and (b) levator ani with anal fascia in the upper part. RECESSES These are narrow extension of the fossa beyond its boundaries. 1. Anterior recess - Extends forwards above the urogenital diaphragm almost up to the posterior surface of the body of pubis. 2. Posterior recess - It is smaller than anterior recess. It extends deep to sacrotuberous ligament. 3. Horse shoe recess (deep post anal space/Post Sphincteric space) Connects the two fossae behind the anal canal CONTENTS OF ISCHIORECTAL FOSSA Inside Alcock's canal, on the lateral wall Internal pudendal artery Internal pudendal vein Pudendal nerve Outside Alcock's canal, crossing the space transversely Perineal branch of fourth sacral nerve Perforating cutaneous branch of S2, S3 nerve Inferior rectal artery Inferior rectal vein Inferior anal nerves Fatty tissue across which numerous fibrous bands extend from side to side PUDENDAL CANAL It is a fascial tunnel present in the lower part of the lateral wall of the Ischiorectal fossa, just above the sacrotuberous ligament Pudendal canal is formed by splitting of the fascia lunata. The fascial wall of the canal is fused laterally to the Obturator fascia, medially to the perineal fascia and inferiorly with the sacrotuberous ligament. It contains pudendal nerve and the internal pudendal vessels. LUNATE FASCIA It arches over the Ischiorectal fat, begins laterally at the pudendal canal and after arching the Ischiorectal fat fuses medially with the fascial covering of external anal sphincter. The fascia divides the Ischiorectal space into (a) Supra tegmental space above (b) Tegmental space below PUDENDAL NERVE S2, S3, S4. In the posterior part of the pudendal canal the pudendal nerve gives off inferior rectal nerve and then it divides into to terminal branches – Perennial nerve Dorsal nerve of penis. The inferior rectal nerve pierces the medial wall of pudendal canal, crosses the Ischiorectal fossa from lateral to medial side and supplies the external sphincter, the skin around the anus and the wall of the anal canal below the pectinate line. PUDENDAL NERVE S2-S4 • • • • • • • • • • • Supplies skin, organs and muscles of perineum Distribution similar in males and females Route: (travels with internal pudendal vessels) Passes through GSF inferior to piriformis Enters the perineum by passing around the ischial spine and sacrospinous ligament Passes through LSF Functions: Micturition Defecation Erection Ejaculation Parturition INTERNAL PUDENDAL ARTERY It is smaller of the two terminal division of the anterior trunk of internal iliac artery. It gives off a branch in the posterior part of the pudendal canal - inferior rectal artery, and then it divides in two terminal branches (a) Perineal artery and (b) Artery to penis. APPLIED ANATOMY Both the Perianal and Ischiorectal spaces are common site of abscesses. Poor blood supply and coarse lobulated fat predispose it for infection. Abscesses in this region are – (a) Perianal abscess (b) Ischiorectal abscess (c) Supra levator abscess (d) Sub mucous abscess. Fournier's Gangrene - An uncommon but potentially lethal complication of Ischiorectal abscess PUDENDAL NERVE (a) SPHINCTERIC INCONTINENCE - Injury to the inferior rectal branch of the pudendal nerve causes Sphincteric incontinence. (b) PUDENDAL BLOCK - The pudendal nerve is infiltrated with local anaesthetic solution where it crosses the ischial spine.This means that when complete perineal anesthesia is required an injection of local anaesthetic must be given around the anus. Through the inter-sphincteric longitudinal fibers the inter-sphincteric abscess tracks down and gives rise to Perianal abscess. THANK YOU