Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
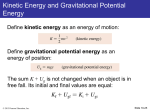
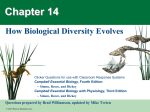
PowerPoint® Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College CHAPTER 28 Pregnancy and Human Development: Part B © Annie Leibovitz/Contact Press Images © 2013 Pearson Education, Inc. Organogenesis • Gastrulation sets stage for organogenesis – Formation of body organs and systems • At eighth week – All organ systems recognizable – End of embryonic period © 2013 Pearson Education, Inc. Organogenesis • Embryo begins as flat plate • Cylindrical body resembling three stacked sheets of paper folding laterally into tube, and at both ends © 2013 Pearson Education, Inc. Figure 28.10 Folding of the embryonic body, lateral views. Head Tail Amnion Yolk sac Ectoderm Mesoderm Endoderm Trilaminar embryonic disc Future gut (digestive tube) Lateral fold Somites (seen through ectoderm) Tail fold Head fold Yolk sac Neural tube Notochord Primitive gut Hindgut © 2013 Pearson Education, Inc. Yolk sac Foregut Specialization of Endoderm • Primitive gut formed from endodermal folding – Forms epithelial lining of GI tract – Organs of GI tract become apparent, and oral and anal openings perforate • Mucosal lining of respiratory tract forms from pharyngeal endoderm (foregut) • Glands arise further along tract © 2013 Pearson Education, Inc. Figure 28.10a Folding of the embryonic body, lateral views. Head Tail Amnion Yolk sac Ectoderm Mesoderm Endoderm © 2013 Pearson Education, Inc. Trilaminar embryonic disc Figure 28.10b Folding of the embryonic body, lateral views. Lateral fold © 2013 Pearson Education, Inc. Future gut (digestive tube) Figure 28.10c Folding of the embryonic body, lateral views. Somites (seen through ectoderm) Tail fold Head fold Yolk sac © 2013 Pearson Education, Inc. Figure 28.10d Folding of the embryonic body, lateral views. Neural tube Notochord Primitive gut Hindgut © 2013 Pearson Education, Inc. Yolk sac Foregut Figure 28.11 Endodermal differentiation. Pharynx Parathyroid glands and thymus Thyroid gland Esophagus Trachea Connection to yolk sac Right and left lungs Stomach Liver Umbilical cord Pancreas Gallbladder Small intestine Allantois Large intestine 5-week embryo © 2013 Pearson Education, Inc. Specialization of Ectoderm • Neurulation – First major event of organogenesis – Gives rise to brain and spinal cord – Induced by chemical signals from notochord – Ectoderm over notochord thickens, forming neural plate – Neural plate folds inward as neural groove with neural folds © 2013 Pearson Education, Inc. Specialization of Ectoderm • By 22nd day, neural folds fuse into neural tube – Anterior end brain; rest spinal cord • Neural crest cells migrate widely cranial, spinal, and sympathetic ganglia and nerves; adrenal medulla; pigment cells of skin; contribute to some connective tissues • Brain waves recorded by end of second month © 2013 Pearson Education, Inc. Figure 28.12a Neurulation and early mesodermal differentiation. Head Amnion Amniotic cavity Left Right Cut edge of amnion Primitive streak Tail Neural plate Ectoderm Mesoderm Notochord Endoderm Yolk sac © 2013 Pearson Education, Inc. 17 days. The flat three-layered embryo has completed gastrulation. Notochord and neural plate are present. Figure 28.12b Neurulation and early mesodermal differentiation. Neural crest Neural groove Neural fold Coelom © 2013 Pearson Education, Inc. Somite Intermediate mesoderm 20 days. The neural folds form by folding of the neural plate, which then deepens, producing the neural groove. Three mesodermal Lateral plate aggregates form on each side of the notochord (somite, mesoderm intermediate mesoderm, and lateral plate mesoderm). Figure 28.12c Neurulation and early mesodermal differentiation. Surface ectoderm Neural crest Neural tube Somite Notochord © 2013 Pearson Education, Inc. 22 days. The neural folds have closed, forming the neural tube which has detached from the surface ectoderm and lies between the surface ectoderm and the notochord. Embryonic body is beginning to undercut. Figure 28.12d Neurulation and early mesodermal differentiation. Neural tube (ectoderm) Somite Dermatome Myotome Sclerotome Kidney and gonads (intermediate mesoderm) Epidermis (ectoderm) Gut lining (endoderm) Lateral plate mesoderm • Limb bud • Smooth muscle of gut • Visceral serosa Peritoneal cavity (coelom) © 2013 Pearson Education, Inc. • Parietal serosa • Dermis End of week 4. Embryo undercutting is complete. Somites have subdivided into sclerotome, myotome, and dermatome, which form the vertebrae, skeletal muscles, and dermis respectively. Body coelom present. Specialization of Mesoderm • First evidence - appearance of notochord – Eventually replaced by vertebral column • Three mesoderm aggregates appear lateral to notochord – Somites, intermediate mesoderm, and double sheets of lateral plate mesoderm © 2013 Pearson Education, Inc. Specialization of Mesoderm • Somites (40 pairs) each have three functional parts – Sclerotome cells - produce vertebra and rib at each level – Dermatome cells - form dermis of skin on dorsal part of body – Myotome cells - form skeletal muscles of neck, trunk, and limbs (via limb buds) © 2013 Pearson Education, Inc. Specialization of Mesoderm • Intermediate mesoderm forms gonads and kidneys • Lateral plate mesoderm consists of somatic and splanchnic mesoderm © 2013 Pearson Education, Inc. Specialization of the Mesoderm • Somatic mesoderm forms – Dermis of skin in ventral region – Parietal serosa of ventral body cavity – Most tissues of limbs • Splanchnic mesoderm forms – Heart and blood vessels – Most connective tissues of body – ~ Entire wall of digestive & respiratory organs © 2013 Pearson Education, Inc. Specialization of the Mesoderm • At end of embryonic period – Bones have begun to ossify; skeletal muscles well formed, contracting; metanephric kidneys developing; gonads formed – Lungs, digestive organs attaining final shape and body position – Blood delivery to/from placenta constant & efficient – Heart and liver bulge on ventral surface © 2013 Pearson Education, Inc. Figure 28.12a Neurulation and early mesodermal differentiation. Head Amnion Amniotic cavity Left Right Cut edge of amnion Primitive streak Tail Neural plate Ectoderm Mesoderm Notochord Endoderm Yolk sac © 2013 Pearson Education, Inc. 17 days. The flat three-layered embryo has completed gastrulation. Notochord and neural plate are present. Figure 28.12b Neurulation and early mesodermal differentiation. Neural crest Neural groove Neural fold Coelom © 2013 Pearson Education, Inc. Somite Intermediate mesoderm 20 days. The neural folds form by folding of the neural plate, which then deepens, producing the neural groove. Three mesodermal Lateral plate aggregates form on each side of the notochord (somite, mesoderm intermediate mesoderm, and lateral plate mesoderm). Figure 28.12c Neurulation and early mesodermal differentiation. Surface ectoderm Neural crest Neural tube Somite Notochord © 2013 Pearson Education, Inc. 22 days. The neural folds have closed, forming the neural tube which has detached from the surface ectoderm and lies between the surface ectoderm and the notochord. Embryonic body is beginning to undercut. Figure 28.12d Neurulation and early mesodermal differentiation. Neural tube (ectoderm) Somite Dermatome Myotome Sclerotome Kidney and gonads (intermediate mesoderm) Epidermis (ectoderm) Gut lining (endoderm) Lateral plate mesoderm • Limb bud • Smooth muscle of gut • Visceral serosa Peritoneal cavity (coelom) © 2013 Pearson Education, Inc. • Parietal serosa • Dermis End of week 4. Embryo undercutting is complete. Somites have subdivided into sclerotome, myotome, and dermatome, which form the vertebrae, skeletal muscles, and dermis respectively. Body coelom present. Figure 28.13 Flowchart showing major derivatives of the embryonic germ layers. Epiblast ECTODERM MESODERM Notochord Somite Intermediate mesoderm ENDODERM Lateral plate mesoderm Somatic mesoderm • Epidermis, hair, nails, glands of skin • Brain and spinal cord • Neural crest and derivatives (e.g., cranial, spinal, and sympathetic ganglia and associated nerves; chromaffin cells of the adrenal medulla; pigment cells of the skin) © 2013 Pearson Education, Inc. Nucleus pulposus of intervertebral discs • Sclerotome: vertebrae and ribs • Dermatome: dermis of dorsal body region • Myotome: trunk and limb musculature • Kidneys • Parietal serosa • Gonads • Dermis of ventral body region • Connective tissues of limbs (bones, joints, and ligaments) Splanchnic mesoderm • Wall of digestive and respiratory tracts (except epithelial lining) • Visceral serosa • Heart • Blood vessels Epithelial lining and glands of digestive and respiratory tracts Development of Fetal Circulation • First blood cells arise in yolk sac • By end of third week – Embryo has system of paired vessels – Two vessels forming heart have fused; bent into "S" shape • Heart beats by 3½ weeks © 2013 Pearson Education, Inc. Development of Fetal Circulation • Unique vascular modifications – Umbilical arteries and umbilical vein – Three vascular shunts • All occluded at birth © 2013 Pearson Education, Inc. Development of Fetal Circulation • Vascular shunts – Ductus venosus - bypasses liver (umbilical vein ductus venosus IVC) – Foramen ovale - opening in interatrial septum; bypasses pulmonary circulation – Ductus arteriosus - bypasses pulmonary circulation (pulmonary trunk ductus arteriosus aorta) © 2013 Pearson Education, Inc. Figure 28.14a Circulation in fetus and newborn. Fetus Aortic arch Superior vena cava Ductus arteriosus Ligamentum arteriosum Pulmonary artery Pulmonary veins Heart Lung Foramen ovale Fossa ovalis Liver Ductus venosus Ligamentum venosum Hepatic portal vein Umbilical vein Ligamentum teres Inferior vena cava Umbilicus Abdominal aorta Common iliac artery Umbilical arteries Medial umbilical ligaments Urinary bladder Umbilical cord Placenta © 2013 Pearson Education, Inc. High oxygenation Moderate oxygenation Low oxygenation Very low oxygenation Figure 28.14b Circulation in fetus and newborn. Aortic arch Superior vena cava Ductus arteriosus Newborn Ligamentum arteriosum Pulmonary artery Pulmonary veins Heart Lung Foramen ovale Fossa ovalis Liver Ductus venosus Ligamentum venosum Hepatic portal vein Umbilical vein Ligamentum teres Inferior vena cava Umbilicus Abdominal aorta Common iliac artery Umbilical arteries Medial umbilical ligaments Urinary bladder © 2013 Pearson Education, Inc. High oxygenation Moderate oxygenation Low oxygenation Very low oxygenation Events of Fetal Development • Fetal period - weeks 9 through 38 • Time of rapid growth of body structures established in embryo © 2013 Pearson Education, Inc. Figure 28.15a Photographs of a developing fetus. Amniotic sac Umbilical cord Umbilical vein Chorionic villi Yolk sac Cut edge of chorion Embryo at week 7, about 17 mm long. © 2013 Pearson Education, Inc. Figure 28.15b Photographs of a developing fetus. Fetus in month 3, about 6 cm long. © 2013 Pearson Education, Inc. Figure 28.15c Photographs of a developing fetus. © 2013 Pearson Education, Inc. Fetus late in month 5, about 19 cm long. Table 28.1 Developmental Events of the Fetal Period (1 of 3) © 2013 Pearson Education, Inc. Table 28.1 Developmental Events of the Fetal Period (2 of 3) © 2013 Pearson Education, Inc. Table 28.1 Developmental Events of the Fetal Period (3 of 3) © 2013 Pearson Education, Inc. Effects of Pregnancy on the Mother: Anatomical Changes • Reproductive organs become engorged with blood – Chadwick's sign - vagina develops purplish hue – Breasts enlarge and areolae darken – Pigmentation of facial skin many increase (chloasma) © 2013 Pearson Education, Inc. Effects of Pregnancy: Anatomical Changes • Uterus expands, occupying most of abdominal cavity – Ribs flare thorax widens • Lordosis occurs with change in center of gravity • Relaxin causes pelvic ligaments and pubic symphysis to relax to ease birth passage • Weight gain of ~13 kg (28 lb) © 2013 Pearson Education, Inc. Effects of Pregnancy: Anatomical Changes • Good nutrition vital – 300 additional daily calories • Multivitamins with folic acid reduce fetal risk of neurological problems, e.g., spina bifida, anencephaly, and spontaneous preterm birth © 2013 Pearson Education, Inc. Figure 28.16 Relative size of the uterus before conception and during pregnancy. Before conception (Uterus the size of a fist and resides in the pelvis.) © 2013 Pearson Education, Inc. 4 months (Fundus of the uterus is halfway between the pubic symphysis and the umbilicus.) 7 months (Fundus is well above the umbilicus.) 9 months (Fundus reaches the xiphoid process.) Effects of Pregnancy: Metabolic Changes • Placental hormones – Human placental lactogen (hPL) (human chorionic somatomammotropin (hCS)) • maturation of breasts, fetal growth, and glucose sparing in mother (reserving glucose for fetus) • Parathyroid hormone and vitamin D levels high throughout pregnancy adequate calcium for fetal bone mineralization © 2013 Pearson Education, Inc. Effects of Pregnancy: Physiological Changes • GI tract – Morning sickness believed due to elevated levels of hCG, estrogen and progesterone – Heartburn and constipation are common • Urinary system – Urine production due to maternal metabolism and fetal wastes – Frequent, urgent urination; stress incontinence may occur as bladder compressed © 2013 Pearson Education, Inc. Effects of Pregnancy: Physiological Changes • Respiratory system – Estrogens may cause nasal edema and congestion – Tidal volume increases – Dyspnea (difficult breathing) may occur later in pregnancy © 2013 Pearson Education, Inc. Effects of Pregnancy: Physiological Changes • Cardiovascular system – Blood volume increases 25–40% • Safeguards against blood loss during childbirth – Cardiac output rises as much as 35-40% • Propels greater volume around body – Venous return from lower limbs may be impaired, resulting in varicose veins © 2013 Pearson Education, Inc. Homeostatic Imbalance • Preeclampsia – Insufficient placental blood supply fetus starved of oxygen – Woman edematous, hypertensive, proteinuria – Believed due to immunological abnormalities • Correlated with number of fetal cells that enter maternal circulation © 2013 Pearson Education, Inc. Parturition • Giving birth to baby • Labor – Events that expel infant from uterus • Increased production of surfactant protein A (SP-A) in weeks before delivery inflammatory response in cervix softening in preparation for labor © 2013 Pearson Education, Inc. Initiation of Labor • Fetus determines own birth date • During last few weeks of pregnancy – Fetal secretion of cortisol stimulates placenta to secrete more estrogen • Causes production of oxytocin receptors by myometrium • Causes formation of gap junctions between uterine smooth muscle cells • Antagonizes calming effects of progesterone, leading to Braxton Hicks contractions in uterus © 2013 Pearson Education, Inc. Initiation of Labor • Surfactant protein A (SP-A) from fetal lungs causes softening of cervix • Fetal oxytocin causes placenta to produce prostaglandins • Oxytocin and prostaglandins - powerful uterine muscle stimulants – Due especially to prostaglandins, contractions more frequent and vigorous – Anti-prostaglandins contraindicated during labor © 2013 Pearson Education, Inc. Initiation of Labor • Increasing cervical distension – Activates hypothalamus, causing oxytocin release from posterior pituitary – Positive feedback mechanism occurs • Greater distension of cervix more oxytocin release greater contractile force greater distension of cervix etc. © 2013 Pearson Education, Inc. Figure 28.17 Hormonal induction of labor. Start Estrogen Oxytocin from placenta from fetus and mother's posterior pituitary Induces oxytocin receptors on uterus Stimulates uterus to contract Stimulates placenta to release (+) Prostaglandins Stimulate more vigorous contractions of uterus © 2013 Pearson Education, Inc. Positive feedback (+) Stages of Labor: Dilation Stage • From labor's onset to fully dilated cervix (10 cm) • Longest stage of labor - 6–12 hours or more • Initial weak contractions: – 15–30 minutes apart, 10–30 seconds long – Become more vigorous and rapid • Cervix effaces and dilates fully to 10 cm • Amnion ruptures, releasing amniotic fluid • Engagement occurs - head enters true pelvis © 2013 Pearson Education, Inc. Figure 28.18 Parturition. 1a Early dilation. Baby’s head engaged; widest dimension Is along left-right axis. 1b Late dilation. Baby’s head rotates so widest dimension is in anteroposterior axis (of pelvic outlet). Dilation nearly complete Umbilical cord Placenta Uterus Cervix Vagina Slide 1 Pubic symphysis Sacrum 2 Expulsion. Baby’s head extends as it is delivered 3 Placental stage. After baby is delivered, the placenta detaches and is removed. © 2013 Pearson Education, Inc. Perineum Uterus Placenta (detaching) Umbilical cord Figure 28.18 Parturition. 1a Early dilation. Baby’s head engaged; widest dimension Is along left-right axis. © 2013 Pearson Education, Inc. Umbilical cord Placenta Uterus Cervix Vagina Slide 2 Figure 28.18 Parturition. 1a Early dilation. Baby’s head engaged; widest dimension Is along left-right axis. 1b Late dilation. Baby’s head rotates so widest dimension is in anteroposterior axis (of pelvic outlet). Dilation nearly complete © 2013 Pearson Education, Inc. Umbilical cord Placenta Uterus Cervix Vagina Pubic symphysis Sacrum Slide 3 Stages of Labor: Expulsion Stage • From full dilation to delivery of infant • Strong contractions every 2–3 minutes, about 1 minute long • Urge to push increases (in absence of local anesthesia) • Crowning occurs when largest dimension of head distends vulva – Episiotomy may be done to reduce tearing © 2013 Pearson Education, Inc. Figure 28.18 Parturition. 1a Early dilation. Baby’s head engaged; widest dimension Is along left-right axis. 1b Late dilation. Baby’s head rotates so widest dimension is in anteroposterior axis (of pelvic outlet). Dilation nearly complete Umbilical cord Placenta Uterus Cervix Vagina Pubic symphysis Sacrum 2 Expulsion. Baby’s head extends as it is delivered Perineum © 2013 Pearson Education, Inc. Slide 4 Stages of Labor: Expulsion Stage • Vertex position – head-first – Skull dilates cervix; early suctioning allows breathing prior to complete delivery • Breech position – buttock-first – Delivery more difficult; often forceps required, or C-section (delivery through abdominal and uterine wall incision) © 2013 Pearson Education, Inc. Figure 28.18 Parturition. 1a Early dilation. Baby’s head engaged; widest dimension Is along left-right axis. 1b Late dilation. Baby’s head rotates so widest dimension is in anteroposterior axis (of pelvic outlet). Dilation nearly complete Umbilical cord Placenta Uterus Cervix Vagina Slide 5 Pubic symphysis Sacrum 2 Expulsion. Baby’s head extends as it is delivered 3 Placental stage. After baby is delivered, the placenta detaches and is removed. © 2013 Pearson Education, Inc. Perineum Uterus Placenta (detaching) Umbilical cord Stages of Labor: Placental Stage • Strong contractions continue, causing detachment of placenta and compression of uterine blood vessels – Limit bleeding; cause placental detachment • Delivery of afterbirth (placenta and membranes) occurs ~30 minutes after birth • All placenta fragments must be removed to prevent postpartum bleeding © 2013 Pearson Education, Inc. Adjustments of the Infant to Extrauterine Life • Neonatal period - four-week period immediately after birth • Physical status assessed 1–5 minutes after birth – Apgar score - 0–2 points each for • Heart rate • Respiration • Color • Muscle tone • Reflexes – Score of 8–10 - healthy © 2013 Pearson Education, Inc. First Breath • CO2 central acidosis stimulates respiratory control centers to trigger first inspiration – Requires tremendous effort – airways tiny; lungs collapsed – Surfactant in alveolar fluid helps reduce surface tension • Respiratory rate ~45 per minute first two weeks, then declines © 2013 Pearson Education, Inc. First Breath • Keeping lungs inflated difficult for premature infant (< 2500 g, or 5.5 pounds, at birth) – Surfactant production in last months of prenatal life – Preemies usually on respiratory assistance until lungs mature © 2013 Pearson Education, Inc. Transitional Period • Unstable period lasting 6–8 hours after birth – Alternating periods of activity and sleep – Vital signs may be irregular during activity – Baby gags frequently as regurgitates mucus and debris • Stabilizes with waking periods occurring every 3–4 hours © 2013 Pearson Education, Inc. Occlusion of Fetal Blood Vessels • Umbilical arteries and vein constrict and become fibrosed • Proximal umbilical arteries superior vesical arteries to urinary bladder • Distal umbilical arteries medial umbilical ligaments © 2013 Pearson Education, Inc. Occlusion of Fetal Blood Vessels • Umbilical vein becomes round ligament of liver (ligamentum teres) • Ductus venosus ligamentum venosum about 30 minutes after birth • Pressure changes from infant breathing cause pulmonary shunts to close – Foramen ovale fossa ovalis up to a year after birth – Ductus arteriosus ligamentum arteriosum about 30 minutes after birth © 2013 Pearson Education, Inc. Lactation • Production of milk by mammary glands • Toward end of pregnancy – Placental estrogens, progesterone, and human placental lactogen stimulate hypothalamus to release prolactin-releasing factors (PRFs) – Anterior pituitary releases prolactin • 2-3 days later true milk production begins © 2013 Pearson Education, Inc. Lactation • Colostrum – Less lactose but more protein, vitamin A, minerals than true milk; almost no fat – Yellowish secretion rich in IgA antibodies • IgA resistant to digestion; may protect infant against bacterial infection; absorbed into bloodstream for immunity – Released first 2–3 days – Followed by true milk production © 2013 Pearson Education, Inc. Lactation • Prolactin release wanes after birth • Lactation sustained by mechanical stimulation of nipples - suckling – Suckling causes afferent impulses to hypothalamus prolactin stimulates milk production for next feeding – Hypothalamus also oxytocin from posterior pituitary let-down reflex © 2013 Pearson Education, Inc. Figure 28.19 Milk production and the positive feedback mechanism of the milk let-down reflex. Hypothalamus releases prolactin releasing factors (PRF) to portal circulation. Start Positive feedback Stimulation of mechanoreceptors in nipples by suckling infant sends afferent impulses to the hypothalamus. Hypothalamus sends efferent impulses to the posterior pituitary where oxytocin is stored. Anterior pituitary secretes prolactin to blood. Oxytocin is released from the posterior pituitary and stimulates myoepithelial cells of breasts to contract. Prolactin targets mammary glands of breasts. Let-down reflex. Milk is ejected through ducts of nipples. © 2013 Pearson Education, Inc. Milk production Advantages of Breast Milk • Fats and iron better absorbed; amino acids more easily metabolized, compared with cow's milk • Beneficial chemicals – IgA, complement, lysozyme, interferon, and lactoperoxidase (protect from infections) – Interleukins and prostaglandins prevent overzealous inflammatory responses – Glycoprotein deters ulcer-causing bacterium from attaching to stomach mucosa © 2013 Pearson Education, Inc. Advantages of Breast Milk • Natural laxative effect helps eliminate bile-rich meconium, helping to prevent physiological jaundice • Encourages bacterial colonization of large intestine • Women nursing 6 months lose bone calcium; replaced after weaning if healthy diet • Women may ovulate when nursing despite inhibition of GnRH and gonadotropins © 2013 Pearson Education, Inc. Assisted Reproductive Technology • Surgical removal of oocytes following hormone stimulation • Fertilization of oocytes • Return of fertilized oocytes to woman's body • Disadvantages – Costly, emotionally draining, painful for oocyte donor © 2013 Pearson Education, Inc. Assisted Reproductive Technology • In vitro fertilization (IVF) – Oocytes and sperm incubated in culture dishes for several days – Embryos (two-cell to blastocyst stage) transferred to uterus for possible implantation © 2013 Pearson Education, Inc. Assisted Reproductive Technology • Zygote intrafallopian transfer (ZIFT) – Fertilized oocytes transferred to uterine tubes • Gamete intrafallopian transfer (GIFT) – Sperm and harvested oocytes are transferred together into the uterine tubes • Cloning – Legal, moral, ethical, political roadblocks © 2013 Pearson Education, Inc.