Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
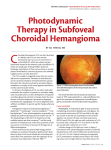
Choroidal Rupture Secondary to Ocular Paintball Injury Michele Avila, O.D. Optometry Resident 09/01/2009 Abstract: Ocular trauma due to paintball injuries can have devastating visual outcomes. This case report will focus on one such injury, a choroidal rupture. This is a condition in which hydraulic shockwaves, usually from blunt force trauma, cause tears in Bruch’s membrane exposing the underlying sclera. I. Case History a. 24 year old African American male b. Referred by the ER due to pain, redness, photophobia, and decreased vision secondary to being hit in the right eye by a paintball the previous day. Patient had not been wearing protective eyewear c. Ocular and medical history was unremarkable, and the patient did not wear contact lenses or spectacles d. Current medications included hydrocodone Q4h and Pred Forte Q4h, both given to the patient by the emergency room e. No known drug allergies f. The patient was oriented to time, place, and person II. Pertinent Findings a. Uncorrected VA was Count Fingers at 4 feet OD and 20/25 at distance OS. There was no improvement with pin hole OD, 20/20 OS b. Pupils were equally round and reactive to light, no afferent pupil defect was noted OU c. Extraocular muscles were unrestricted in all gazes d. Confrontation VFs showed a slightly decreased superior-nasal field OD, and a full field OS e. Intraocular pressure was 18 mmHg OD and 15 mmHg OS by Goldmann Applanation Tonometry f. Anterior segment evaluation by slit lamp examination revealed i. 3-4+ bulbar conjunctiva hyperemia 360° OD and quiet conjunctiva OS ii. Lashes were quite with no debris OU iii. The cornea OD had a large 3 mm abrasion inferior-temporal with surrounding edema, several areas with paint embedded into the corneal stroma, and negative for Seidel’s sign; Cornea OS was intact and clear iv. OD iris had a hemorrhage from 1 to 2 o’clock with a blood/inflammatory membrane extending from the site of hemorrhage thru the pupil into the posterior chamber; iris was flat OS v. Anterior chamber OD was deep but positive for RBC with a 2 mm settling hyphema and blood dusting on the inferior corneal endothelium; OS was clear without cells or flare and the estimate of the anterior chamber angles was 4/4 by VonHerrick. g. The patient was dilated with 1% Atropine OD in office but the posterior segment was unable to be evaluated at the first visit secondary to the hyphema and inflammatory membrane h. At the three-day follow-up visit the posterior segment was able to be examined and evaluation revealed: i. ii. iii. iv. v. Optically clear crystalline lenses OU Normal optic nerves with a cup-to-disc ratio of 0.3 round OU The neuroretinal rims were pink, full, and intact OU Retinal vessels appeared normal with arterial-venous ration of 2/3 noted OU The macula of the right eye was positive for edema with surrounding retinal hemorrhages, while the macula OS was flat and intact vi. The posterior pole OD showed a crescent-shaped sub-retinal streak laying inferior-temporal concentric to the macula with an overlying sub-retinal hemorrhage; OS was flat and intact vii. The peripheral retinal of the right eye had large areas of edema with no holes or tears noted; OS was flat and intact with no pathology III. Differential Diagnoses considered for anterior segment OD included: a. Traumatic hyphema (primary) b. Iridodialysis c. Corneal abrasion (primary) d. Ruptured globe e. Corneal stromal foreign bodies (primary) IV. Differential Diagnoses considered for posterior segment OD included: a. Commotio Retinae/Berlin Edema OD (Primary) b. Retinal detachment OD c. White without pressure OD d. Sub-Retinal Hemorrhage OD (Primary) e. Choroidal Rupture OD (Primary) f. Choroidal Neovascularization OD V. Diagnosis a. At the time of the initial visit the patient was diagnosed with traumatic hyphema and corneal abrasion with stromal foreign bodies from the paint splinters OD b. Once a view was able to be obtained of the posterior segment OD the patient was also diagnosed as having commotion retinae, sub-retinal hemorrhage, and choroidal rupture c. Two weeks after the incident the patient also suffered an intraocular pressure spike in the right eye from traumatic iritis d. Approximately two weeks after the paintball incident occurred a traumatic cataract began to form in the right eye, and the cataract was subsequently removed VI. Discussion a. Choroidal ruptures often occur as the result of blunt ocular trauma or injury. They arise when a tear occurs in Bruch’s membrane and the choriocapillaris. The breaks may be one or many and usually run concentric to the optic nerve, though radial ruptures can occur. The site of a fresh rupture may be initially obscured by retinal or vitreal hemorrhages. As the blood begins to absorb, usually after weeks to months, an underlying yellow-white crescent shaped streak of exposed sclera becomes visible. b. Vision loss and field defects are common following such damage. The extent of the visual and ocular damage can range widely depending on the extent of the foveal involvement and development of late complications such as a choroidal neovascular membrane (CNV). c. A study out of the Palmer Eye Institute at the University of Miami, Miller School of Medicine on thirty-six eyes that had sustained ocular injuries secondary to paintballs, found that the visual acuity at initial presentation correlated strongly with the final visual acuity outcome. The same study also found that the use of protective eyewear may have eliminated 97% of injuries in the study subjects1. d. ICG Angiography can be used to localize areas of choroidal rupture and identify areas of choroidal neovasuclar membrane formation. Choroidal ruptures can cause damage to the choroidal vessels such as delayed filling in choroidal veins and intrachoroidal leakage. The use of indocyanine green (ICG) angiography can help to identify early neovascular membranes and localize areas of choroidal rupture even when they are still obscured by retinal hemorrhages and cannot easily be identified with ophthalmoscopy or fluorescein angiography2. e. Epiretinal membranes (ERM) are another complication that can arise from the presence of choroidal ruptures. As retinal glial cells proliferate they can extend through the defects in the internal limiting membrane (ILM) creating the ERM3. Fibrotic scar tissue at the site of the rupture may also serve as a framework for the glial cell extensions increasing the spread of the ERM. Vitrectomy and membrane peel are usually required if the ERM becomes visually devastating, and they are often preformed with good visual success. VII. Treatment and Management a. There is no immediate treatment for choroidal rupture b. Other management includes thorough patient education, in-office monitoring at six to twelve month intervals, self-monitoring with an Amsler grid, and the diligent use of protective eyewear c. This patient had multiple other ocular injuries that needed to be addressed as well so he was instructed to continue PredForte Q2h, and begin Zymar QID and Combigan BID, all in the right eye. He was also instructed to use homatropine BID OD d. A bandage contact lens was placed on his eye for the corneal abrasion, a fox shield was placed over the patient’s right eye for protection, and he was instructed to avoid any physical activity or blood thinners, and to sleep with his head elevated at 45°-90° angle due to the hyphema e. This patient was referred to a retinal specialist once a posterior segment view was possible and choroidal rupture suspected. No CNV was noted by the retina doctor at the times of their first or second exam, but the presence of a large choroidal rupture was confirmed. The retinal specialist opted for no treatment at this time and chose close observation with continued use of the above mentioned eye drops. f. At the nine month follow-up visit to our office best corrected visual acuities were stable at 20/70- OD and 20/20 OS. He is pseudophakic OD and still has paint embedded in the corneal stroma. No changes in the Amsler grid were reported. The patient is scheduled to return to the retinal specialist for repeat angiography in two weeks, and to return to our office in six months for gonioscopy and visual fields, or sooner with any signs or symptoms of retinal detachment, decreases in vision, or changes to the Amsler grid. VIII. Conclusion a. Paintball injuries can have severe and devastating effects on a patient’s visual outcome. Some of the effects, such as the development of a choroidal neovascular membrane or epiretinal membrane, may occur several years after the initial traumatic incident. ICG angiography is beneficial in the localization of the choroidal rupture as well as any neovascular membrane formations. Removal and/or treatment of any secondary epiretinal or neovascular membranes may also help to improve the visual outcome of the patient. With the large number of people engaging in the sport of paintball, extra emphasis needs to be placed on the importance of protective safety eyewear to prevent these detrimental ocular and visual outcomes. IX. Bibliography 1. Grigorian, A. Paula MD. Ocular Trauma and Visual Outcome Secondary to Paintball Projectiles. Evidence-Based Ophthalmology. Issue: Volume 10(3), July 2009, pp 144-145 2. Takeya Kohno MD. Department of Ophthalmology, Osaka City University Medical School, Osaka, Japan. Indocyanine green angiographic features of choroidal rupture and choroidal vascular injury after contusion ocular injury. American Journal of Ophthalmology. Volume 129, Issue 1, January 2000, Pages 38-46 3. EV Gotzaridis, AN Vakalis, CS Sethi and DG Charteris. Surgical removal of sequential epiretinal and subretinal neovascular membranes in a patient with traumatic choroidal rupture. Eye (2003) 17, 790–791. doi:10.1038/sj.eye.6700472