Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
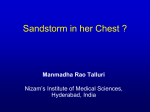
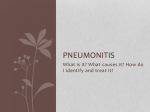
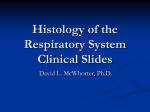
® PULMONARY DISEASE BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, PUBLISHER Bruce M.White Alveolar Hemorrhage Syndromes EXECUTIVE EDITOR Debra Dreger SENIOR EDITOR Miranda J. Hughes, PhD EDITOR Becky Krumm Series Editor: Robert A. Balk, MD, FACP, FCCP, FCCM Professor of Medicine, Director of Pulmonary and Critical Care Medicine, Department of Medicine, Rush Medical College and Rush-Presbyterian-St. Luke’s Medical Center, Chicago, IL ASSISTANT EDITOR Kathryn Charkatz EDITORIAL ASSISTANT Barclay Cunningham SPECIAL PROGRAMS DIRECTOR Barbara T.White, MBA Contributing Author: David P. Gurka, MD, PhD, FCCP Assistant Professor of Medicine, Section of Pulmonary and Critical Care Medicine, Department of Medicine, Rush Medical College and Rush-Presbyterian-St. Luke’s Medical Center, Chicago, IL PRODUCTION MANAGER Suzanne S. Banish PRODUCTION ASSOCIATE Vanessa Ray Table of Contents ADVERTISING/PROJECT COORDINATOR Patricia Payne Castle Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Case Presentations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 NOTE FROM THE PUBLISHER: This publication has been developed without involvement of or review by the American Board of Internal Medicine. Clinical Features and Initial Evaluation . . . . . . . . . . . . . . 4 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 Alveolar Hemorrhage Syndromes. . . . . . . . . . . . . . . . . . . 7 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Endorsed by the Association for Hospital Medical Education The Association for Hospital Medical Education endorses HOSPITAL PHYSICIAN for the purpose of presenting the latest developments in medical education as they affect residency programs and clinical hospital practice. Summary Points . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Board Review Questions and Answers . . . . . . . . . . . 10, 11 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Suggested Readings . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Cover Illustration by Dean Vigyikan Copyright 1998, Turner White Communications, Inc., 125 Strafford Avenue, Suite 220, Wayne, PA 19087-3391. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, mechanical, electronic, photocopying, recording or otherwise, without the prior written permission of Turner White Communications, Inc. The editors are solely responsible for selecting content. Although the editors take great care to ensure accuracy, Turner White Communications, Inc., will not be liable for any errors of omission or inaccuracies in this publication. Opinions expressed are those of the authors and do not necessarily reflect those of Turner White Communications, Inc. Pulmonary Disease Volume 5, Part 1 1 ® PULMONARY DISEASE BOARD REVIEW MANUAL Alveolar Hemorrhage Syndromes Series Editor: Robert A. Balk, MD, FACP, FCCP, FCCM Contributing Author: David P. Gurka, MD, PhD, FCCP Professor of Medicine Director of Pulmonary and Critical Care Medicine Department of Medicine Rush Medical College and Rush-Presbyterian-St. Luke’s Medical Center Chicago, IL Assistant Professor of Medicine Section of Pulmonary and Critical Care Medicine Department of Medicine Rush Medical College and Rush-Presbyterian-St. Luke’s Medical Center Chicago, IL I. INTRODUCTION Alveolar hemorrhage is the occurrence of blood arising from and pooling in pulmonary acinar sacs. This relatively uncommon finding is often associated with extrapulmonary and/or laboratory abnormalities that characterize a diverse group of disorders known as alveolar (or pulmonary) hemorrhage syndromes. Alveolar hemorrhage syndromes are frequently immune-mediated but may also involve drug or toxin exposure. Alveolar hemorrhage is often associated with renal disease. There is no universally accepted classification scheme for alveolar hemorrhage syndromes, although in general they are grouped by extrapulmonary clinical manifestations or by the histologic presence or absence of capillaritis (Table 1). Pulmonary capillaritis was first described by Spencer in 1957, in association with polyarteritis nodosa. The concept was refined by Mark and Ramierez in 1985 in their report on patients with systemic vasculitides. Pulmonary capillaritis is characterized by infiltration of the alveolar interstitium by neutrophils, which leads to fibrinoid necrosis of the capillary walls with leakage of erythrocytes and neutrophils into the alveolar septa and spaces. Fibrin thrombi can be found occluding the septal capillaries as well as lining the alveolar sacs. Erythrocytes are present in the interstitium and alveolar spaces in the 2 Hospital Physician Board Review Manual presence of acute hemorrhage, and hemosiderin-laden macrophages and free hemosiderin are markers of recent or chronic hemorrhage. Inflammation of the pulmonary vasculature is usually indicative of a systemic vasculitis. Although any form of bleeding diathesis or other condition that increases pulmonary capillary pressure (ie, mitral stenosis, pulmonary veno-occlusive disease, pulmonary capillary hemangiomatosis) can manifest as alveolar hemorrhage, this review will be restricted to those entities, with as well as without capillary inflammation, in which the alveolar epithelium or capillary endothelium is directly involved. Because the differential diagnosis of alveolar hemorrhage is broad (Table 1), only the more common of these relatively rare syndromes will be discussed. The relative frequencies of the causes of alveolar hemorrhage are not well delineated. In one 6-year series of patients from the University of Minnesota, the most common cause of alveolar hemorrhage was anti–glomerular basement membrane (anti-GBM) antibody disease, followed by the systemic vasculitides (many types), pauci-immune glomerulonephritis, and connective tissue diseases (eg, systemic lupus erythematosis).1 Another review, however, found Wegener’s disease and other vasculitides to be nearly three times as prevalent as anti-GBM antibody disease as a cause of alveolar hemorrhage.2 Alveolar Hemorrhage Syndromes II. CASE PRESENTATIONS Table 1. Classification of Alveolar Hemorrhage Syndromes Alveolar hemorrhage with capillaritis CASE PATIENT 1 A 24-year-old nurse without significant past medical history presents with progressive dyspnea on exertion associated with a nonproductive cough. For the past 2 weeks, she has had a nonresolving, flu-like illness with arthralgias, myalgias, headache, low-grade fever, nausea, and vomiting. Three weeks earlier, she had presented with a lesion on her left lateral thigh; skin biopsy results were consistent with erythema nodosum. Her laboratory results at that time were as follows: hemoglobin, 10 g/dL; blood urea nitrogen (BUN), 14 mg/dL; creatinine, 1.0 mg/dL; erythrocyte sedimentation rate (ESR), 55 mm/hour (standard reference value is < 20). Antinuclear antibody (ANA) titer was weakly positive at 1:40, and rheumatoid factor and complement (C3 and C4) levels were normal. She was taking no medications, used neither tobacco nor illicit drugs, and had no allergies. She reported an involutional weight loss of 8 lbs over the preceding 2 months. On presentation, she is quite anxious, afebrile, normotensive without tachycardia or orthostatic changes, and in no respiratory distress. With the exception of pale conjunctiva and nailbeds, the remainder of the physical examination is unremarkable. She has no skin lesions, joint abnormalities, or adventitious cardiac or pulmonary sounds. Laboratory data are significant for the following values: hemoglobin, 6.9 g/dL, BUN, 18 mg/dL; creatinine, 1.3 mg/dL; ESR, 96 mm/hour. Neither thrombocytopenia nor coagulation abnormalities are found. Urinalysis reveals hematuria (> 200 erythrocytes/low-power field) without pyuria or cellular casts. Chest radiograph and computed tomographic (CT) scan of case patient 1 are shown in Figure 1. CASE PATIENT 2 A 30-year-old man with a history of systemic lupus erythematosus (SLE) since age 23 years and previous episodes of alveolar hemorrhage presents with hemoptysis that has been present for the past 4 weeks. It initially manifested as blood-streaked sputum and progressed to pure blood expectoration of 5 to 10 mL per cough, 5 to 10 times per day. He denies fever, chills, dyspnea, chest discomfort, rash, arthralgias, epistaxis, or hematemesis. He has been treated empirically with three 1-week courses of antibiotics, and his dose of prednisone has been increased from 20 mg every other day to 40 mg daily; neither therapy has been effective. Systemic necrotizing vasculitides Microscopic polyangiitis Wegener’s granulomatosis Behçet’s syndrome Henoch-Schönlein purpura Essential mixed cryoglobulinemia Connective tissue disorders Systemic lupus erythematosus Antiphospholipid syndrome Mixed connective tissue disease Scleroderma Rheumatoid arthritis Pulmonary-renal syndromes Anti–glomerular basement membrane antibody disease Immune complex–associated glomerulonephritis Pauci-immune glomerulonephritis Alveolar hemorrhage without capillaritis Idiopathic pulmonary hemosiderosis Exogenous agents Cocaine D-penicillamine Trimellitic anhydride Lymphangiography Other disorders Diffuse alveolar damage Mitral stenosis Bleeding diatheses Bone marrow transplantation Pulmonary veno-occlusive disease Pulmonary capillary hemangiomatosis Lymphangioleiomyomatosis Tuberous sclerosis On admission, his temperature is 97.2 °F, blood pressure is 114/84 mm Hg, pulse rate is 80 bpm, and respiration rate is 14 breaths/min. He has no nasal or oropharyngeal bleeding stigmata, his lungs are clear to auscultation in all fields, he has no cardiac murmurs or rubs, and there is no evidence of lower extremity edema or asymmetry. Laboratory tests reveal a hemoglobin level of 12.1 g/dL (his baseline value is 13.1 g/dL); normal Pulmonary Disease Volume 5, Part 1 3 Alveolar Hemorrhage Syndromes A B Figure 1. (A) Standard posteroanterior chest radiograph and (B) high-resolution noncontrast computed tomographic scan of the patient described in case 1.The subtle diffuse alveolar filling shadows of the radiograph are visible in the computed tomographic scan as diffuse “ground glass” opacities involving all the lobes. platelet count, leukocyte count, and coagulation times; BUN and creatinine levels of 23 mg/dL and 0.8 mg/dL, respectively (not significantly elevated from his baseline levels); and trace hematuria (4 erythrocytes/low-power field). His complement levels are markedly depressed: C3 level is 45 mg/dL (standard reference value is 80–180 mg/dL) and C4 level is 7 mg/dL (standard reference value is 16–60 mg/dL). ANA titer was 1:640 and antibody to double-stranded DNA (dsDNA) was titered to 1:80. Chest radiograph and chest CT are shown in Figure 2. • Which features of these cases suggest a diagnosis of alveolar hemorrhage? • What additional testing is needed to confirm the diagnosis and determine the etiology? III. CLINICAL FEATURES AND INITIAL EVALUATION PRESENTING SIGNS AND SYMPTOMS Cough and dyspnea are the most common complaints in patients with alveolar hemorrhage. A complaint of “coughing up blood” must be carefully differentiated from epistaxis or hematemesis. Hemoptysis is often not noted on initial presentation but, when present, can vary from mildly blood-tinged sputum to massive bleeding. Chest pain and pleuritis may accompany 4 Hospital Physician Board Review Manual alveolar hemorrhage, and mild dyspnea can rapidly progress to respiratory failure. Malaise and fatigue are common manifestations of anemia or uremia. A slight darkening of the urine can denote hematuria. Extrapulmonary symptoms such as weight loss, arthralgias, rashes, or purpura, when accompanied by the nonspecific findings of malaise and fatigue, often focus attention on the possible presence of an autoimmune or vasculitic process. Generally, symptoms are of relatively short duration (a few weeks) and are either persistent or recurrent. Information gleaned from a careful history, such as occupational exposures, infections, and medications, often gives clues to etiology. PHYSICAL EXAMINATION Physical examination may reveal tachypnea and the moist lung crackles of alveolar fluid accumulation. Auscultatory findings of mitral stenosis (an opening snap and diastolic rumble, best appreciated with the patient in the left lateral decubitus position) should be sought. Evaluation of the nasal mucosal surfaces for bleeding sites or septal ulcers is often diagnostically rewarding. A careful survey of the skin and musculoskeletal system is warranted to uncover signs of vasculitis or connective tissue disorders. RADIOGRAPHIC EVALUATION Standard posteroanterior and lateral chest radiographs are usually the only imaging procedures Alveolar Hemorrhage Syndromes A B Figure 2. (A) Standard posteroanterior chest radiograph and (B) standard noncontrast computed tomographic scan of the patient described in case 2. The dense diffuse alveolar filling shadows of the posteroanterior film are visible in the computed tomographic scan as dense airspace filling opacities sparing the upper lobes. necessary for evaluation of alveolar hemorrhage. Diffuse or patchy alveolar filling opacities are the most common finding, although an interstitial pattern can be seen if the bleeding is recurrent or chronic. CT scan better highlights parenchymal masses, such as those found in Wegener’s disease, or areas of bronchiectasis that may account for hemoptysis. An echocardiogram may be indicated to confirm the presence of mitral stenosis. LABORATORY EVALUATION Initial laboratory evaluation should include an arterial blood gas, a complete blood cell count with platelet count, BUN and creatinine levels, coagulation studies, urinalysis with microscopic evaluation for casts and erythrocytes, and ESR. Special antibody studies, such as ANA, rheumatoid factor, anti-GBM antibody, and antineutrophil cytoplasmic antibodies (ANCAs) are appropriate in patients with systemic complaints or abnormalities of renal function. PULMONARY FUNCTION TESTS Pulmonary function tests, including the measurement of carbon monoxide diffusion (DLCO), are performed in cases of suspected occult alveolar hemorrhage, as well as for monitoring patients with recurrent hemorrhage. Spirometry results are often normal and lung volumes may be normal. In cases of recurrent alveolar hemorrhage or some of the vasculitides, lung volumes may be reduced, reflecting the restrictive ventilatory defect of many autoimmune diseases. Alveolar hemorrhage is one of the few disorders (along with congestive heart failure, left-to-right intracardiac shunts, and polycythemia) that give rise to an elevated DLCO, typically greater than 125% of the predicted value, reflecting binding of carbon monoxide to the increased amount of pulmonary hemoglobin in these disorders. Serial DLCO measurements are used to monitor for occult exacerbations of alveolar hemorrhage in those patients with a predisposition to or history of the disease. BRONCHOSCOPIC EVALUATION Bronchoscopy is necessary to confirm the presence of alveolar hemorrhage as well as to rule out focal endobronchial lesions that can present with hemoptysis. The characteristic bronchoalveolar lavage of alveolar hemorrhage is apparent when sequential aliquots of a single segmental lavage reveal fluid that becomes increasingly hemorrhagic; the initial pink lavage becomes a darker red color, often looking like pure blood at the end of the procedure. Cytologic analysis of the lavage shows a predominance of erythrocytes in acute alveolar hemorrhage and hemosiderin-laden macrophages in recent or recurrent bleeding. Transbronchial biopsies are rarely performed because the size of the specimens is usually inadequate for performing fluorescent antibody staining. Furthermore, the focal nature of some disorders may lead to sampling error. Open lung biopsy may be needed to fully evaluate some patients, although percutaneous renal biopsy is a less invasive procedure yielding sufficient tissue to diagnose those patients with renal involvement. Pulmonary Disease Volume 5, Part 1 5 Alveolar Hemorrhage Syndromes Table 2. Laboratory Characteristics of Selected Diseases Causing Alveolar Hemorrhage Disease Characteristics Anti-GBM disease Anti-GBM antibody present SLE Hypocomplementemia, ANA ↑ Wegener’s granulomatosis C-ANCA present Microscopic polyangiitis P-ANCA present Pauci-immune glomerulonephritis P-ANCA present; anti-GBM antibody absent Behçet’s syndrome Circulating IgG immune complexes Henoch-Schönlein purpura Circulating IgA immune complexes Idiopathic pulmonary hemosiderosis No extrapulmonary abnormalities, no abnormal serologies ANA = antinuclear antibody; ANCA = antineutrophil cytoplasmic antibody; GBM = glomerular basement membrane; Ig = immunoglobulin; SLE = systemic lupus erythematosis. IV. DIAGNOSIS EVALUATION OF CASE PATIENTS Case Patient 1 Prior to bronchoscopy of case patient 1, pulmonary function tests showed normal spirometry results and lung volumes but a DLCO of 157% of the predicted value. Alveolar hemorrhage was confirmed by lavage. Because of her rapid rise in creatinine, a renal biopsy was performed prior to obtaining the results of serologic studies. The biopsy showed focal segmental necrotizing glomerulonephritis; immunofluorescent and electron microscopic studies of the biopsied tissue failed to reveal immune deposits. Assay for serum antiGBM antibody was negative but assay for perinuclear (P)-ANCA was positive; a specific antimyeloperoxidase (anti-MPO) antibody was detected. A diagnosis of pauci-immune glomerulonephritis with alveolar hemorrhage (ie, without immune complex deposition in the biopsy tissue) was made. Case Patient 2 Because of the patient’s history of SLE, previous episodes of alveolar hemorrhage, and his current presentation, alveolar hemorrhage was strongly suspected. DLCO was 83% of the predicted value, but serial DLCO in the past showed his baseline to be 50% to 60% of the 6 Hospital Physician Board Review Manual predicted value, owing to SLE-induced pulmonary fibrosis. Bronchoscopy was performed to rule out infection in this immunocompromised host; only alveolar hemorrhage was found. Cytologic analysis of the lavage fluid showed a large quantity of hemosiderin macrophages. • How are the alveolar hemorrhage syndromes diagnosed? • What are the immediate and long-term treatment options for these patients? DISCUSSION The combination of cough, anemia, and a chest radiograph showing patchy alveolar opacities—with or without hemoptysis—strongly suggests alveolar hemorrhage. The differential diagnosis of hemoptysis is broad and has been addressed in Volume 4, Part 1 of the Pulmonary Disease Board Review Manual (Balk RA: Case Studies in Pulmonary Emergencies). Serologic and Immunologic Testing After bronchoscopic confirmation of alveolar hemorrhage, patients with abnormal renal findings (ie, hematuria and/or renal insufficiency) or extrapulmonary complaints require appropriate serologic testing and tissue fluorescent antibody staining to identify the correct syndrome so that therapy can be initiated (Table 2). The finding of hematuria excludes idiopathic pulmonary hemosiderosis from diagnostic consideration. The presence of serum anti-GBM antibody confirms a diagnosis of Goodpasture’s disease. Hypocomplementemia is a feature of alveolar hemorrhage due to SLE or, occasionally, mixed cryoglobulinemia. Serum ANCA levels are elevated in Wegener’s granulomatosis and in systemic necrotizing vasculitis (microscopic polyangiitis) as well as pauci-immune glomerulonephritis. Two types of ANCA can be measured. Cytoplasmic (C)-ANCA is specific for proteinase 3, a neutral protease found in cytoplasmic granules of neutrophils. C-ANCA is relatively sensitive and specific for Wegener’s granulomatosis. P-ANCA is an autoantibody to the neutrophilic MPO granule and is more likely to be found in patients with pauci-immune glomerulonephritis or microscopic polyangiitis. Fluorescent staining of tissue biopsy specimens for the deposition of immunoglobulins (Ig) can assist in narrowing the diagnosis. Linear deposition of IgG along either alveolar or renal glomerular basement membranes is found in Goodpasture’s disease. Granular deposition of IgG is characteristic of SLE and mixed cryoglobulinemia; granular IgA deposits indicate Henoch-Schönlein purpura. The absence of Alveolar Hemorrhage Syndromes immune deposits suggests systemic necrotizing vasculitis, pauci-immune glomerulonephritis, or idiopathic pulmonary hemosiderosis. V. ALVEOLAR HEMORRHAGE SYNDROMES WEGENER’S GRANULOMATOSIS Wegener’s granulomatosis is a systemic necrotizing granulomatous inflammatory illness predominately involving the upper and lower respiratory tracts and the kidneys. Cutaneous and ocular disturbances also occur in approximately 50% of affected individuals. The disease may be indolent or rapidly lead to renal failure. Upper airway symptoms of sinusitis, initially thought to be caused by allergy or infection but unresponsive to the usual therapies, are the presenting complaints of more than 70% of patients with Wegener’s granulomatosis.3 Cough and hemoptysis are early symptoms in only 15% to 20% of cases but eventually develop in 30% to 50% over the course of the illness. Pulmonary capillaritis is found in 40% to 50% of biopsy specimens, but alveolar hemorrhage is relatively rare, occurring in only 5% to 8% of cases. Hemoptysis is more often related to pulmonary nodules or infection than to alveolar hemorrhage, but alveolar hemorrhage is often an initial presentation and heralds a fulminant, rapidly progressive course. If alveolar hemorrhage is present with rapidly progressive focal segmental necrotizing glomerulonephritis, acute mortality can be as high as 65%, despite the institution of therapy. The prognosis is much better in the more common cases without alveolar hemorrhage. Remission can be induced in nearly 90% of these patients and sustained in nearly half of them. A variant of Wegener’s granulomatosis in which clinical involvement is limited to the respiratory tract carries an even better prognosis. The diagnosis requires the pathologic demonstration of vasculitis and necrotizing granulomata in the appropriate clinical context of airway, renal, and other systemic abnormalities. Tissue staining for immune deposits is negative and no circulating immune complexes are found. The demonstration of C-ANCA in serum in many cases can confirm the diagnosis, obviating biopsy. Transbronchial biopsies have been shown to have a diagnostic yield of less than 10%;4 open-lung or renal biopsies are preferred. Chest radiographs initially show nodules, frequently cavitary (25%) or fleeting alveolar opacities (25%). The frequency of these findings increases to 60% to 70% as the disease progresses. CT may better delineate the often subtle nodular pulmonary lesions and reveal sinus involvement. Standard therapy for Wegener’s granulomatosis consists of vigorous immunosuppression with high-dose corticosteroids and cytotoxic agents, usually cyclophosphamide. The finding of either alveolar hemorrhage or rapidly progressive glomerulonephritis (RPGN) warrants aggressive therapy with “pulse” steroids of 1 g per day of methylprednisolone with concomitant high-dose cyclophosphamide (3–5 mg/kg body weight per day). This regimen is continued for 3 to 5 days before lowering the doses to 1 mg/kg per day of prednisone (or equivalent corticosteroid) and 2 mg/kg per day of cyclophosphamide. Tapering of the steroid is initiated once the disease remits. Tapering of the cyclophosphamide dose should not take place until at least a year after remission has been achieved. Remission can be induced in 50% of patients within 12 months and in 90% within 24 months, and maintained in half of these patients for months to years before relapse.3,4 Serial testing of C-ANCA as an early marker of relapse or disease activity is of limited value, as is the use of trimethoprim-sulfamethoxazole to sustain remission. Patients with child-bearing potential should be advised of the teratogenic risks of cytotoxic therapy and offered sperm or ova banking procedures. MICROSCOPIC POLYANGIITIS Microscopic polyangiitis is a systemic necrotizing vasculitis of small vessels (capillaries, venules and arterioles) with RPGN and pulmonary involvement. Men are more frequently affected than women by a ratio of 2:1, and the average age of onset is 50 years. Most patients present with arthralgias or constitutional symptoms (typically fever) that often antedate the diagnosis of microscopic polyangiitis by months to years. Twenty-five percent to thirty percent of patients have alveolar hemorrhage at some point in their disease, usually from alveolar capillaritis or bronchial arteritis. It is second only to Wegener’s as a vasculitic cause of alveolar hemorrhage.2 Like Wegener’s disease, microscopic polyangiitis is a pauci-immune vasculitis, but it lacks the granulomatous inflammation of Wegener’s. Complement levels are normal. Rheumatoid factor is found in 40% to 50% of patients; ANA titer is positive less frequently. ANCA is present in 75% of patients, with anti-MPO P-ANCA being the most prevalent form. Therapy for alveolar hemorrhage associated with microscopic polyangiitis is similar to that for Wegener’s disease: “pulse” steroids with high-dose cyclophosphamide, with cyclophosphamide maintenance until remission. Pulmonary Disease Volume 5, Part 1 7 Alveolar Hemorrhage Syndromes BEHÇET’S SYNDROME Behçet’s syndrome is a multisystem disease characterized by recurrent aphthous stomatitis, genital and oral ulcers, iridocyclitis, thrombophlebitis, cutaneous vasculitis, arthritis, and meningoencephalitis. Immune complexes may be found in the circulation as well as in pulmonary and glomerular capillaries. Alveolar hemorrhage occurs in 5% to 10% of cases and can arise from pulmonary capillaritis, inflammatory destruction of pulmonary arteries, rupture of bronchial artery aneurysms, and pulmonary infarction. Pulmonary complaints of cough, hemoptysis, chest pain, and fever are more common in men than in women. Death generally occurs within 6 years of the first episode of hemoptysis. Alveolar hemorrhage was the cause of death in 40% of the patients in one series.5 Therapy of alveolar hemorrhage associated with Behçet’s syndrome is administration of corticosteroids with cytotoxic immunosuppression. HENOCH-SCHÖNLEIN PURPURA Although primarily a disease of children, HenochSchönlein purpura may occur in adults as well. It is a syndrome comprising palpable purpura (leukocytoclastic vasculitis), glomerulonephritis, arthralgias, arthritis, abdominal pain, gastrointestinal hemorrhage, and, in 5% to 10% of patients, pulmonary involvement with bleeding from capillaritis or pulmonary infarctions. Serologic tests for ANA and rheumatoid factor are typically negative. IgA immune complexes can be found in the circulation as well as in immune deposits along alveolar or renal basement membranes. Therapy is usually with corticosteroids. It is postulated that exposure to some insult (eg, tobacco smoke, inhalation injury, infection) exposes more of the basement membrane antigen for the IgG autoantibody to bind. The antigen is the carboxylterminal fragment of type IV (α) collagen, found mainly in alveoli, glomeruli, renal interstitial tubules, and choroid plexus. Linear deposition of IgG along the membrane leads to complement binding and activation with subsequent fragmentation of the basement membrane. This pattern occurs in clinically uninvolved alveolar or renal tissue as well. Granular deposits indicative of the entrapment of circulating immune complexes are not seen. Therapy is directed toward rapid reduction in the serum levels of anti-GBM antibodies and in the inflammatory response induced by their deposition. Treatment may need to be initiated before the results of serum anti-GBM tests have returned, because long-term survival depends on the extent of renal involvement, and renal function can decline dramatically. Plasmapheresis is used to quickly remove circulating anti-GBM antibodies and is often continued for 2 to 4 weeks. Treatment with high-dose pulse corticosteroids (1 g per day for 3 days) followed by at least 1 month of 1 mg/kg body weight of prednisone per day with a subsequent taper blunts the inflammation of anti-GBM antibody deposition and impairs the continued production of antibody. A 6-month course of cyclophosphamide (Cytoxan), given daily at 2 to 3 mg/kg body weight, or monthly in intravenous pulses of 750 to 1000 mg/M2 body surface area, is frequently added to provide longer-term reduction in antibody formation. ANTI–GLOMERULAR BASEMENT MEMBRANE ANTIBODY DISEASE Anti-GBM antibody disease is also known as Goodpasture’s disease. The lung and kidney are the only two organs involved in anti-GBM antibody disease. In most cases, both are affected simultaneously, although alveolar hemorrhage is often the presenting symptom. Renal disease is the sole manifestation in only 20% to 40% of cases; alveolar hemorrhage alone is extremely uncommon (< 10% of cases).7 The presence of cutaneous vasculitis or arthralgias excludes the diagnosis of antiGBM antibody disease. In general, patients are young, between 20 and 30 years of age, and male (less than one third are women). In older patients, the sex distribution is nearly equal and the disease more often spares the lungs. Smoking is an additional risk factor for alveolar hemorrhage in anti-GBM antibody disease: in 80% of nonsmokers, the disease was limited to the kidney, and almost all smokers had alveolar hemorrhage.1 GLOMERULONEPHRITIDES Two forms of idiopathic pulmonary-renal syndrome are characterized by finding an RPGN (acute renal insufficiency with erythrocyte casts in the urine) in association with alveolar hemorrhage; these are the immune complex–mediated and pauci-immune forms. In neither disorder is there involvement of any other organs, although these two entities may be variants of microscopic polyangiitis. Alveolar hemorrhage is rare in immune complex–mediated RPGN. Like Wegener’s granulomatosis and microscopic polyangiitis, pauciimmune RPGN lacks any immunoreaction product in tissue specimens. Alveolar hemorrhage is often a presenting finding and occurs in approximately 50% of afflicted individuals. Differentiation from anti-GBM antibody disease, which is also limited to lung and kidney involvement by definition, is provided by the absence of linear IgG deposition in histologic specimens and the absence of serum anti-GBM antibody. 8 Hospital Physician Board Review Manual Alveolar Hemorrhage Syndromes P-ANCA is often detected. Therapy is with combination high-dose corticosteroids and cytotoxic agents, often requiring pulse therapy to treat severe rapidly progressive renal dysfunction or life-threatening alveolar hemorrhage. SYSTEMIC LUPUS ERYTHEMATOSUS Alveolar hemorrhage is a rare (< 2%) complication of SLE. It is associated with high mortality and is recurrent in survivors. Alveolar hemorrhage is the presenting manifestation in 10% to 20% of patients but most often occurs in established cases. Unlike in acute lupus pneumonitis, which can also present with hemoptysis, dyspnea, fever, cough, and diffuse alveolar opacities on chest radiograph, pleural and pericardial effusions are absent and hemoglobin concentrations are significantly reduced. Serologic evidence for SLE as a cause of alveolar hemorrhage includes an increase in the ANA titer along with serum hypocomplementemia. In a recent review from the University of Colorado, overall mortality of patients with SLE and alveolar hemorrhage was 42%.6 Poor prognostic factors were the need for mechanical ventilation (62% mortality), the presence of any infection (78% mortality), and the use of cytotoxic therapy (70% mortality). Effective therapy consisted of prolonged (more than 3 days) pulse steroids with or without plasmapheresis. Empiric broadspectrum antibiotic therapy should be employed prior to an aggressive search for infection. ALVEOLAR HEMORRHAGE DUE TO EXOGENOUS AGENTS D-Penicillamine, used as both a chelating agent and an antirheumatic drug, has been reported to produce a complex of alveolar hemorrhage with glomerulonephritis that has been termed drug-induced Goodpasture’s syndrome. Unlike in anti-GBM antibody disease, serum anti-GBM antibodies are absent, there is a history of ingestion of the drug, and there is granular (rather than linear) deposition of IgG and C3 along involved basement membranes. Because the pathogenesis appears to be immune complex–mediated, cessation of the drug and immunosuppressive therapy combined with plasmapheresis have been used in a few cases with good effect. Trimellitic anhydride, an acid anhydride used in the manufacture of plastics, paints, and resins, has been shown to induce isolated alveolar hemorrhage, usually 1 to 3 months after exposure. It is believed that inhalation of fumes, especially when used as a spray in a hightemperature coating process, induces formation of antibodies to trimellitic anhydride–conjugated proteins. These antibodies, found in the circulation and respiratory tract, may be pathogenic. A Coombs’ test–positive hemolytic anemia is often found. Therapy is avoidance of the compound. Cocaine, especially smoking of the freebase form, has been implicated in cases of massive hemoptysis and alveolar hemorrhage. Postmortem examinations of the lungs of cocaine abusers who died from unrelated causes have demonstrated hemosiderin-laden macrophages. The etiology of the association of alveolar hemorrhage and cocaine use is unclear. IDIOPATHIC PULMONARY HEMOSIDEROSIS Idiopathic pulmonary hemosiderosis is a diagnosis of exclusion characterized by recurrent alveolar hemorrhage without other organ involvement. Pulmonary histology shows only “bland” alveolar hemorrhage with hemosiderin accumulation. Serology testing is negative, ESR is not elevated, and iron deficiency anemia is common. IgA levels may be elevated. It is predominately a disease of children, but adults older than 30 years comprise 20% of reported cases and generally have a milder course. An association with celiac disease has been recognized, and therapy of the celiac disorder has resulted in remission of the idiopathic pulmonary hemosiderosis. Chronic parenchymal bleeding can lead to the development of pulmonary fibrosis with subsequent respiratory insufficiency and finger clubbing. Magnetic resonance imaging may have a role in distinguishing alveolar hemorrhage from other causes of pulmonary radiographic abnormalities, especially in small children in whom bronchoscopy may be technically difficult. Therapy is generally supportive, with transfusions and supplementation of iron and oxygen. Immunosuppressive therapy has been advocated to treat acute hemorrhage, but the rarity of the disease precludes controlled studies. ALVEOLAR HEMORRHAGE ASSOCIATED WITH BONE MARROW TRANSPLANTATION In a review of autologous bone marrow transplant recipients for lymphoma or solid tumors, alveolar hemorrhage occurred in 21% of these patients, with a mortality rate of 80%.7 This was a relatively early finding, occurring an average of 12 days post-transplant. Patients with alveolar hemorrhage had higher platelet counts than those without alveolar hemorrhage; leukemic patients with thrombocytopenia had relatively benign alveolar hemorrhage. Risk factors for fulminant alveolar hemorrhage included: age older than 40 years, severe mucositis, transplantation for solid tumor, azotemia, and a rising leukocyte count. The hypothesis was put forth that the Pulmonary Disease Volume 5, Part 1 9 Alveolar Hemorrhage Syndromes pretransplant conditioning regimen damaged alveolar structures that were then ruptured by the increase in circulating cells as the marrow engrafted. Therapy was supportive and generally ineffective. • • VI. CONCLUSION Although relatively rare, alveolar hemorrhage can present explosively, with massive hemoptysis, or insidiously, with dyspnea and fatigue. It is most often associated with extrapulmonary—usually renal—disease. Rapid recognition is imperative because the hemorrhage itself can be life-threatening or concurrent renal dysfunction can quickly lead to renal failure. Therapy should generally be initiated with high-dose steroids and cytotoxic therapy while awaiting the results of histologic and serologic testing. • VII. SUMMARY POINTS • • Alveolar hemorrhage is the pooling of blood in the pulmonary alveoli. It frequently occurs in association with extrapulmonary diseases, most often renal disease. • Alveolar hemorrhage syndromes are frequently immune-mediated but may also involve drug or toxin exposure. • Cough and dyspnea are the most common complaints in patients with alveolar hemorrhage. Hemoptysis may or may not be present. • If alveolar hemorrhage is accompanied by extrapulmonary symptoms such as weight loss, arthralgias, or rashes, the possibility of an autoimmune or vasculitic disease process should be pursued. • Alveolar hemorrhage can usually be evaluated with plain posteroanterior and lateral chest radiographs. Diffuse or patchy alveolar filling opacities are the most common finding. • Initial laboratory testing should include arterial blood gas, complete blood cell count with platelet count, BUN and creatinine levels, coagulation studies, urinalysis with microscopic evaluation for casts and erythrocytes, and ESR. • In patients with systemic manifestations or signs of renal disease, antibody studies such as measurement of ANA, rheumatoid factor, anti-GBM antibody, and ANCA should be performed. • Pulmonary function tests (including measurement of DLCO) should be performed in cases of suspected 10 Hospital Physician Board Review Manual occult alveolar hemorrhage and to monitor patients with recurrent hemorrhage. Bronchoscopy is necessary to confirm the presence of alveolar hemorrhage and to rule out focal endobronchial lesions that can present with hemoptysis. Therapy for alveolar hemorrhage should be directed at the underlying disorder. It most frequently involves administration of corticosteroids and cytotoxic immunosuppression. Because alveolar hemorrhage and any associated renal dysfunction are lifethreatening, therapy should be initiated while awaiting the results of serologic and histologic testing. Pauci-immune vasculitides most commonly associated with alveolar hemorrhage are Wegener’s granulomatosis, microscopic polyangiitis, and pauci-immune glomerulonephritis. Other alveolar hemorrhage syndromes associated with immunologic mechanisms include Behçet’s syndrome, Henoch-Schönlein purpura, anti-GBM disease, and SLE. Alveolar hemorrhage may be caused by exposure to toxic agents, most notably D-penicillamine, trimellitic anhydride, and cocaine. BOARD REVIEW QUESTIONS Part 1. Choose the single best answer for each of the following questions. 1. Diffuse alveolar hemorrhage with capillaritis is characterized by all of the following EXCEPT: A) Lymphocytic invasion of the interstitium with fibrinoid necrosis and capillary thrombosis B) Loss of integrity of the alveolar capillary membrane with leakage of erythrocytes into the alveolar space C) Hemosiderin accumulation in the alveolar macrophages and the lung parenchyma D) Organization of the alveolar hemorrhage 2. All of the following statements regarding alveolar hemorrhage are true EXCEPT: A) It can be caused by crack cocaine B) It can be caused by use of penicillamine C) It develops with renal disease on exposure to trimellitic anhydride D) Hemoptysis can be delayed E) The presence of Kerley’s B lines implies underlying mitral stenosis Alveolar Hemorrhage Syndromes Which of the following statements regarding alveolar hemorrhage in bone marrow transplant patients is true? A) It most commonly occurs late after transplant (more than 100 days post-transplant) B) It occurs with worsening neutropenia C) It commonly occurs in association with severe thrombocytopenia D) It is less severe in patients with leukemia than in those with solid tumors or lymphoma Part 2. For the following questions, more than one answer may be correct. 9. Immune deposits can be found in lung tissue sections in which of the following alveolar hemorrhage syndromes? A) Goodpasture’s disease B) Systemic lupus erythematosis C) Idiopathic pulmonary hemosiderosis D) Henoch-Schönlein purpura E) Microscopic polyangiitis 10. Which of the following statements regarding therapy for alveolar hemorrhage are true? A) Therapy often can be held pending histologic diagnosis B) Therapy should include plasmapheresis when Goodpasture’s disease is suspected C) Empiric therapy with steroids and cytotoxic agents should be given D) Therapy should empirically include broadspectrum antibiotics E) Therapy has been established by prospective randomized trials ANSWERS 5. B 10. B, C, D All of the following statements regarding HenochSchönlein purpura are true EXCEPT: A) It presents with a purpuric rash and glomerulonephritis B) It is an immune complex–mediated disease C) Circulating antibody directed against IgG is found D) Serum tests for antinuclear antibody (ANA) and rheumatoid factor are usually negative E) Pulmonary involvement in the form of alveolar hemorrhage is relatively rare (< 10%) 8. 4. A 9. A, B, D 6. Which of the following statements regarding Wegener’s granulomatosis is true? A) A focal segmental necrotizing glomerulonephritis is uncommon B) Typical histology consists of medium-vessel involvement, tissue necrosis, and granulomatous inflammation C) There is always a cutaneous leukocytoclastic vasculitis D) Only histologic analysis can differentiate it from systemic necrotizing vasculitis Which of the following statements regarding idiopathic pulmonary hemosiderosis is true? A) The diagnosis is one of exclusion B) It is predominantly a disease of older adults C) Typical chest radiograph findings include multiple nodules D) Finger clubbing is rarely seen 3. B 8. D 5. Which of the following statements regarding Goodpasture’s disease is true? A) Lung and renal disease appear simultaneously in most cases B) The highest incidence is in women aged 30 through 40 years C) In younger age groups the disease is more likely to be limited to the renal system D) There is no relationship between severity of the renal disease and outcome 7. 2. C 7. A 4. Which of the following statements regarding alveolar hemorrhage syndromes is true? A) DLCO is initially high and increases with time if there is no further bleeding B) Henoch-Schönlein purpura is characterized by circulating immune IgA complexes C) Only 20% of patients with Goodpasture’s disease and alveolar hemorrhage are smokers D) There is evidence of systemic vasculitis in Goodpasture’s disease E) Anti–glomerular basement membrane (antiGBM) antibodies are specific for Wegener’s granulomatosis 1. A 6. C 3. Pulmonary Disease Volume 5, Part 1 11 Alveolar Hemorrhage Syndromes REFERENCES 1. Leatherman JW, Davies SF, Hoidal JR: Alveolar hemorrhage syndromes: diffuse microvascular lung hemorrhage in immune and idiopathic disorders. Medicine (Baltimore) 1984;63:343–361. 2. Dweik RA, Arroliga AC, Cash JM: Alveolar hemorrhage in patients with rheumatic disease. Rheum Dis Clin North Am 1997;23:395–410. 3. Hoffman GS, Kerr GS, Leavitt RY, et al: Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992;116:488–498. 4. Duna GF, Galperin C, Hoffman GS: Wegener’s granulomatosis. Rheum Dis Clin North Am 1995;21:949–986. 5. Schwarz MI, Cherniack RM, King TE Jr: Diffuse Alveolar Hemorrhage and Other Rare Infiltrative Disorders. In Textbook of Respiratory Medicine, 2nd ed. Murray JF, Nadel JA, eds. Philadelphia: WB Saunders, 1994:1889–1912. 6. Zamora MR, Warner ML, Tuder R, Schwarz MI: Diffuse alveolar hemorrhage and systemic lupus erythematosus: clinical presentation, histology, survival, and outcome. Medicine (Baltimore) 1997;76:192–202. 7. Young KR Jr: Pulmonary Hemorrhage Syndromes. In Textbook of Pulmonary and Critical Care Medicine. Bone RC, Dantzker DR, George RB, et al, eds. St. Louis: Mosby, 1993. Vol 2, Part M, Chapter 10. SUGGESTED READINGS Cahill BC, Ingbar DH: Massive hemoptysis: assessment and management. Clin Chest Med 1994;15:147–167. Green RJ, Ruoss SJ, Kraft SA, et al: Pulmonary capillaritis and alveolar hemorrhage: update on diagnosis and management. Chest 1996;110:1305–1316. Lhote F, Guillevin L: Polyarteritis nodosa, microscopic polyangiitis, and Churg-Strauss syndrome: clinical aspects and treatment. Rheum Dis Clin North Am 1995;21:911–947. Primack SL, Miller RR, Muller NL: Diffuse pulmonary hemorrhage: clinical, pathologic, and imaging features. AJR Am J Roentgenol 1995;164:295–300. Copyright 1998 by Turner White Communications Inc., Wayne, PA. All rights reserved. 12 Hospital Physician Board Review Manual