Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
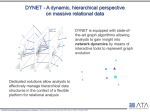
Background and follow-up of the drug court case in South Africa Dr Wilbert Bannenberg WHO Technical Adviser Pharmaceuticals “The goal of the National Drug Policy is to ensure an adequate and reliable supply of safe, costeffective drugs of acceptable quality to all citizens of South Africa and the rational use by prescribers, dispensers and consumers” 1996: NDP implementation strategy Technical support (WHO/SADAP) Legislation (Act 90 of 1997) Standard Treatment Guidelines, Essential Drug Lists Training, capacity building programmes Transformation of Medicines Control Council WHO access framework 1. Rational 3. Sustainable selection financing ACCESS 2. Affordable prices 4. Reliable health and supply systems What Act 90 was to achieve... Parallel import (15C) Generic substitution Preventing perverse incentives (bonusing, sampling) Licensing dispensing doctors Pricing Committee Why did Industry block Act 90? South Africa sets dangerous precedent: 1st TRIPS compliant developing country “TRIPS does not allow parallel import” “Unfettered powers of the Minister are unconstitutional” Perverse incentives = marketing tool Delay generic substitution (R 2m / day) 1. Selection 1. Rational selection ACCESS Good selection practices priority for essential drugs evidence based standard treatment guidelines provide objective information accompanying training systems consult widely mostly accepted by industry New drugs needed! big needs: – growing resistance problems (MDR-TB) – new diseases (HIV/AIDS) limited progress: – R&D geared towards developed countries – few drugs for diseases of poverty if invented, drugs are patented, and often unaffordable 2. Affordable prices ACCESS 2. Affordable prices 1998: Affordable prices? HAART: R 70,000 / year Cryptococcus: R 13,500 pp / year MDR-TB: R 25,000 pp / year CMV retinitis: R 12,000 / 2 weeks 1998 data Discount for public sector? 140 120 124 100 80 Fluconazole, Rands 60 40 29 20 0 SA private SA public 1.8 Thai generic Patents keep drugs expensive! 6 5.59 5 4 3 Ciprofloxacin, Rands 2 1 0.4 0 SA public Indian generic What can the public sector afford? Preventive care: yes Testing, counselling: yes Opportunistic infections: almost all Palliative care: yes Needlestick injuries: yes MTCT: yes Antiretrovirals for AIDS: needs further price reductions (generics) and additional drug budget < Trevor Manual Can the private sector afford ARVs? up to 37% of health expenditure already spent on drugs & medical supplies 14,000 AIDS patients receive ARVs from “Aid for AIDS” project in SA After recent price reductions, ARVs are affordable (USD 900 pp/yr) and costeffective. Politics of competition: d4T pricing 300 250 BMS: $274 US$ 200 150 Brazil: $197 100 BMS: $55 50 Cipla: $69 Hetero: $47 0 Oct 2000 Nov Dec Jan 2001 Feb March April d4T brand d4T generic Other price reduction strategies Information service - UNICEF/WHO/UNAIDS negotiation: equity pricing for poorer countries: based on need and ability to pay tiered vaccine prices a model? reduction of taxes and duties application of TRIPS “health safeguards”: – early working / Bolar, – compulsory licenses, – parallel imports Impact of TRIPS on drugs Higher prices for new drugs Generics competition delayed Weaker local pharmaceutical industry in developing countries Drug production concentrated in a few rich countries (17 countries 84%) Parallel import World-wide shopping for same drug Cause: differential pricing by industry Principle not (yet) enabled in Patent Act Act 90, 15C allows parallel import Private sector: 5% savings (R400m?) Public sector: modest saving (R 20m?) Compulsory licenses Limits to exclusive rights in case of: – public health emergency – non-commercial government/public use – excessively high prices (abuse) Savings 10-97% (depends on pricing) Was always legal under SA Patent Law Bilateral trade pressures prevented its use; court case reversed this! Early working (Bolar provision) Testing, registering generics (before patent expiry) currently illegal in SA but not outside SA (competitive advantage foreign companies!) Unnecessary delay 1-2 years Early working provision agreed by DTI and DOH (amendment Patent Act?) 1997: TRIPS-plus pressures TRIPS = minimum agreement USA: 301 Watch list; bilateral pressure for more patent protection – patent extensions (USA: 23 years) – no compulsory licensing – no parallel import EU: trade pressure – no Bolar 1999: International opinion shifts AIDS activists follow Al Gore Clinton “allows” parallel import for AIDS crisis in Africa (if TRIPS compliant) USA stops bilateral trade pressures EU also reverses trade pressures 2000: Accelerating access (?) 10 May 2000 UNAIDS announcement Few hard data - bilateral negotiations Senegal, Uganda, Kenya, Rwanda: less than 2000 HIV+ people benefit from 75-90% price reductions SA: industry offers, but politicians not interested in ARVs SA: private sector prices down (USD 900 pp/year) 2001: Why drop the court case? AIDS is a crisis beyond proportion Moral outrage on profits drug companies Parallel import accepted by WTO USA, EU changed position Legal arguments are weak Bad PR: “stop case whatever it takes” Multinationals press local PMA Donations Pfizer: fluconazole for cryptococcal meningitis, oesophageal candidiasis (2 years) Boehringer Ingelheim: nevirapine for MTCT (5 years) prevent loss of control at any cost (compulsory licensing) more profitable to donate than to sell cheap! Compulsory license or price reduction? Compulsory License Patents Act SA controls non-exclusive allows generics clear procedure prices cheaper? Conditions, royalties Reduced price offer voluntary offer international control exclusive brandname only terms not yet clear prices higher? Conditions? Current Patent Acts in Africa? Many African countries have no preTRIPS patent Act – <2006: free import of all generics – >2006: free import of all drugs patented before 1995 Is the drug patented? (e.g., ddI in SA) Namibia, Mozambique: ARVs not patented (bus trips, Internet pharmacy?) 3. Financing 3. Sustainable financing ACCESS Sustainable financing? Public Private Turnover R 2 billion R 8 billion Per capita R 64 R 952 Drugs % of Health 9% 36-43% Health spending in Africa 1977-1997 (% of GDP) 4 3.5 3 2.5 Private 2 1.5 Public 1 0.5 0 1977 1987 1997 Financing: sustainable? Declining total public health funding in Africa, changing public and private shares. Substantial out of pocket spending Four principal sources of finance for health: out of pocket, tax-funding, insurance contributions, external support (donations, loans (debt?)). National “pooling” strategies recommended by WHR2000. Public finance offers greatest pooling potential in LDCs; rarely achieved ARVs for SA’s public sector? 250 200 150 100 USD (millions) 50 0 ARV Prices have dropped 90%, but... Big farma USD 600/yr Generics USD 250/yr 500,000 AIDS cases needing ARVs cost >>USD 125m / year (and increasing!) need additional drug budget! Botswana example? drug budget 4. Health infrastructure ACCESS 4. Reliable health and supply systems Infrastructure, supply, training new ARV drugs need more than $$: – more, better trained doctors – dedicated infectious disease nurses? – VCT, laboratory services (CD4, VL?) – informed patients – COTS, FOTS, NOTS? controlled distribution 95% adherence needed… pilot projects, then scale up? Court case follow-up Act 90 Regulations to be gazetted (December?) Sections of Act 90 to be promulgated by President Pricing Committee? Political climate more conducive for voluntary (and compulsory?) licensing Pricing Committee Minister to appoint members Committee’s tasks: – draft Regulations – study Pricing Systems (public+private) – monitor prices – recommend action where needed (PI, CL, negotiations, etc) Pharmaco-economic evaluation Licensing Dispensing Doctors NDP objectives: – Separate prescribing / dispensing – Remove financial incentives for Rx Licenses for services in rural areas and where there is no pharmacy License requires training, inspection Emergency administration allowed So what? The TRIPS compliance debate is over Doha to review health issues TRIPS Country support needed to include public health safeguards into law Drug prices will drop to prevent CL Access to ARVs = next debate – private sector (SA): cost-effective – public sector: Botswana test case? Thank you!