Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
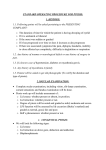
■증례보고■ Anesth Pain Med 2009; 4: 87~90 Persistent ptosis following stellate ganglion block with local anesthetic −A case report− Departments of Anesthesiology and Pain Medicine, *Ophthalmology, College of Medicine, The Catholic University of Korea, Seoul, Korea Seung Yong Kim, M.D., Young Hoon Kim, M.D., Suk Woo Yang, M.D.*, and Dong Eon Moon, M.D. A 45-year-old woman underwent stellate ganglion block (SGB) for treatment of anosmia. She was treated with standardized SGB two to three times a week for two months. Although her anosmia improved slightly, she complained of discomfort and persistent ptosis in her left eye after the fourteenth block. After a five-month observation period, she was evaluated in the department of ophthalmology for persistent ptosis. A phenylephrine test suggested a neurogenic origin for the ptosis. Surgical repair was performed. Clinicians should be careful when performing SGB with local anesthetics to avoid microtrauma, ischemic injury, and neurotoxic injury of the sympathetic nerve fibers. (Anesth Pain Med 2009; 4: 87∼90) CASE REPORT A 45-year-old woman complained of anosmia lasting for one year. Her anosmia developed shortly after a mild upper respiratory tract infection. She was evaluated in the department of neurosurgery with brain magnetic resonance imaging (MRI), but the probable cause of sensorineural anosmia was not determined. Although she underwent treatment with acupuncture, herbal medicine, and medication from the department of otolaryngology, her symptom did not subside. Key Words: anosmia, complication, Horner’s syndrome, phenylephrine, ptosis, stellate ganglion. After failing all other treatments, she visited the pain clinic. We performed a series of SGB’s on each side alternately two to three times a week for two months using the paratracheal Stellate ganglion block (SGB) is a procedure for blocking technique with a 25-gauge needle inserted at Chassaignac’s the lower cervical and upper thoracic sympathetic chain, and it tubercle on the sixth cervical vertebra. We injected 6 ml of is capable of increasing the cerebral blood flow and modifying 1.0% lidocaine for each block. After the eleventh block, the the immunologic reaction.1,2) It is applicable in the treatment of patient’s anosmia improved slightly. olfactory dysfunction caused by sensorineural impairment in the However, after the fourteenth block on her left side, she olfactory nerves.3) complained of discomfort and persistent ptosis in the ipsilateral Successful block induces a typical Horner’s syndrome on the eye. Anhidrosis was not demonstrated. Signs of miosis and treated side that usually disappears spontaneously after a short conjunctival hyperemia were transient. SGB was stopped since period of time. unexpected complication happened. After observation for five We report a case of persistent Horner’s syndrome, an months, she was evaluated in the department of ophthalmology. uncommon complication, which we corrected through surgical Before phenylephrine testing, the marginal reflex distance repair. (MRD1) and interpalpebral fissure height (IPF) of her left eye were noted to be 0.5 mm and 5.5 mm, respectively, suggestive of significant ptosis (Fig. 1). After two drops of 2.5% phenylephrine HCl and a 5-minute wait, the MRD1 and IPF of her affected eye increased to 2.0 mm and 7.0 mm, respectively 논문접수일:2008년 11월 24일 책임저자:문동언, 서울시 서초구 반포동 505 가톨릭대학교 의과대학 마취통증의학교실 우편번호: 137-040 Tel: 02-590-1537, Fax: 02-537-1951 E-mail: [email protected] (Fig. 2). She had persistent ptosis reversed by a phenylephrine test, which indicated a neurogenic origin. She underwent surgical repair of the ptosis, including ipsilateral levator advancement and bilateral upper blepharoplasty (Fig. 3). Six months 87 88 Anesth Pain Med Vol. 4, No. 1, 2009 Fig. 1. Preoperative findings before phenylephrine test. Persistent ptosis occurs in the left eye after stellate ganglion block with 1% lidocaine. The left eye marginal reflex distance (MRD1) measures 0.5 mm, and the interpalpebral fissure height (IPF) measures 5.5 mm. MRD1 indicates the distance from the upper eyelid margin to the corneal reflex. IPF indicates the vertical aperture height from the lower eyelid to the upper eyelid. Fig. 3. Postoperative findings. The left eye marginal reflex distance (MRD1) measures 2.5 mm, and the interpalpebral fissure height (IPF) measures 7.5 mm after ipsilateral levator advancement and bilateral upper blepharoplasty. MRD2 indicates the distance from the lower eyelid margin to the corneal reflex. syndrome consist of the central, preganglionic, and postganglionic neurons. The first-order (central) neuronal fibers begin at the posterolateral hypothalamus. They descend via the brainstem and synapse at the ciliospinal center of Budge-Waller in the intermediolateral column of the spinal cord at levels C8 to T2. The second-order (preganglionic) neuronal fibers exit the spinal cord through the ventral roots and ascend in the cervical sympathetic chain to the superior cervical ganglion. The third-order (postganglionic) neuronal fibers exit the ganglion to ascend along the carotid artery. Nerve fibers to the eyeball, eyelid, and orbit follow the internal carotid artery into Fig. 2. Preoperative findings after phenylephrine test. After a phenylephrine test, the left eye marginal reflex distance (MRD1) measures 2 mm, and the interpalpebral fissure height (IPF) measures 7 mm. the skull and pass into the cavernous sinus. They then run along the sixth cranial nerve and merge with the ophthalmic division of the trigeminal nerve (V1) to the orbit. Horner’s syndrome can result from interruption of any level of these later, ptosis correction was maintained without relapse, and she components.4,5) Since SGB is related to the preganglionic was satisfied with the result of the repair. neuronal fibers, it is important to investigate a neurogenic origin for persistent ptosis. DISCUSSION Although the diagnosis of Horner’s syndrome is established by history and clinical observation, pharmacological testing can Horner’s syndrome, also called oculosympathetic paralysis, is be used to confirm the diagnosis and to localize the lesion. caused by interruption of the sympathetic innervation to the The foundation of the pharmacological tests is the ability of eye and ocular adnexae. The relevant structures include the the normal sympathetic postganglionic nerve to synthesize and dilator pupillae muscle of the iris, Müller muscle of the upper release norepinephrine at its terminals. The cocaine or pheny- eyelid, sweat glands of the face, and smooth muscles of blood lephrine test can be used to confirm the presence of sym- vessels related to miosis, ptosis, anhidrosis, and conjunctival pathetic denervation. After confirmation of the denervation, 4,5) This patient presented with persistent ptosis after hydroxyamphetamine (Paredrine) can be used to distinguish SGB, but anhidrosis was not present, and miosis and con- central and preganglionic lesions from postganglionic lesions.4,5) hyperemia. junctival hyperemia were transient phenomena. A diagnosis of persistent Horner’s syndrome was made. The sympathetic pathways to the targets related to Horner’s Cocaine inhibits the reuptake of norepinephrine at the synaptic junction between the postganglionic fibers and the dilator pupillae muscle of the iris. A negative response to cocaine Seung Yong Kim, et al:Persistent ptosis after stellate ganglion block 89 instillation indicates the presence of sympathetic denervation. needle injury can cause ischemic injury of the sympathetic However, it does not confirm the location of the lesion.4,5) fibers. Ekatodramis et al.10) reported prolonged Horner’s syn- Phenylephrine, an alpha receptor agonist, acts on the sym- drome due to neck hematoma-induced pressure injury after pathetically innervated Müller muscle of the upper eyelid. We continuous interscalene block. They recommended ultrasono- used the phenylephrine test to evaluate the sympathetic dener- graphic examination to exclude the presence of a hematoma in vation. Normally, the upper eyelid margin overlaps the superior case of persistent Horner’s syndrome. We noted no signs of 6) When the upper eyelid hematoma formation (i.e., swelling of the neck). However, margin descends more than normal, ptosis can be quantified by Kapral et al.11) showed that the blind technique resulted in measuring the IPF and MRD1. IPF indicates the vertical height asymptomatic hematoma formation in 3 out of 12 patients, from the lower eyelid to the upper eyelid. MRD1 indicates the with no hematoma occurring during ultrasonographic guided distance from the light reflex on the cornea to the upper SGB. Gold et al.12) demonstrated that lidocaine could cause eyelid margin. Ptosis is graded according to the MRD1; mild direct neurotoxic injury to neurons in an animal study, even in when it is greater than 1.5 mm, moderate when it is between clinical concentrations. Hodgson et al.13) reported that all local corneal limbus by about 2 mm. 6) 0.5 and 1.5 mm, and severe when it is below 0.5 mm. In anesthetics have potential neurotoxic effects, especially in con- our patient, the MRD1 before the phenylephrine test was 0.5 centrations higher than those used clinically. The mechanism of mm, suggestive of moderate ptosis. It increased by 1.5 mm local anesthetics-induced neurotoxicity includes an increase in after the phenylephrine test. The IPF also increased from 5.5 intracellular Ca2+, membrane disruption, altered perineural mm to 7.0 mm, as much as the MRD1 did. This is paralleled permeability, and edema.12,14,15) Moreover, we considered the by the fact that the Müller muscle lifts the upper eyelid by possibility of neurotoxic injury caused by the alcohol used for about 2 mm as an adjunct elevator under normal conditions.6) skin preparation, but SGB was performed after the skin dried. Our findings indicated recovery of function of the Müller One case of Horner’s syndrome lasting for one year muscle. The findings of the phenylephrine test suggested a following SGB has been reported.16) The investigators believed neurogenic origin of the ptosis. inflammation might have caused blepharospasm mimicking ptosis, Hydroxyamphetamine causes pupillary mydriasis by releasing because the signs and symptoms were resolved by treatment norepinephrine from the postganglionic nerve endings. Pupillary with a nonsteroidal anti-inflammatory agent for two weeks. dilatation will not occur if a lesion exists in the postganglionic Some cases of persistent Horner’s syndrome have been re- Yet, we did not conduct the hydroxyamphetamine test ported after interscalene block or epidural block.10,17,18) Most of in this case. We believed that no central lesion was present them have spontaneously recovered after one year. Sympa- because there were no symptoms or signs suggestive of a thetic preganglionic fibers have proven capable of regenerating mass or vascular lesion, and there were no specific brain MRI after denervation in animal studies. McLachlan19) resected the findings. Moreover, hydroxyamphetamine is no longer commer- cervical sympathetic trunk of guinea pigs and reported that cially available.7) Although we were not sure if the origin of reinnervation was nearly complete after three months. In denervation was in the preganglionic or postganglionic fibers, another experiment, Purves20) cut the cervical sympathetic trunk we concluded that the persistent ptosis was due to sympathetic below the caudal pole of the superior cervical ganglion of denervation following SGB with local anesthetic. guinea pigs and showed that most synaptic responses returned fibers. 4,5) Although the etiology of Horner’s syndrome in this case to normal after six to seven months. However, if a patient has was not determined, the authors discussed the possibilities of trouble with ptosis, surgical repair is a treatment option in microtrauma, ischemic injury, and neurotoxic injury of the compliance with the patient’s request.17,18) We observed our sympathetic fibers. Iannuzzi et al.8) suggested that bony contact patient for five months and decided to perform surgical repair of spinal needle can deform the needle tip (i.e., bending, according to the patient’s needs. According to the literature, splintering, or tearing) which may be the cause of microscopic Müllectomy is the surgery of choice for the repair of ptosis dural lacerations. The damaged needle tip may cause tears of due to Horner’s syndrome.6) However, ipsilateral levator advan- the sympathetic fibers, however carefully the SGB was cement and bilateral upper blepharoplasty were performed in performed. Hadzic et al.9) showed that high injection pressure this case since the patient requested repair of her mild contra- might indicate intraneural needle placement and lead to fasci- lateral ptosis, as well. cular injury and neurologic deficits in dogs. Microvascular In conclusion, clinicians should be fully aware of the possi- 90 Anesth Pain Med Vol. 4, No. 1, 2009 bility of persistent Horner’s syndrome after SGB with local anesthetics, especially since a series of SGB’s is performed frequently by a number of pain specialists. To minimize the possibility of persistent Horner’s syndrome following SGB, we suggest that clinicians avoid needle tip deformity due to bony contact, dilute local anesthetics as much as possible, avoid high injection pressure, administer the injection after the alcohol preparation dries, and diminish the likelihood of hematoma by means of ultrasonographic guided SGB or adequate compression. REFERENCES 1. Umeyama T, Kugimiya T, Ogawa T, Kandori Y, Ishizuka A, Hanaoka K: Changes in cerebral blood flow estimated after stellate ganglion block by single photon emission computed tomography. J Auton Nerv Syst 1995; 50: 339-46. 2. Yokoyama M, Nakatsuka H, Itano Y, Hirakawa M: Stellate ganglion block modifies the distribution of lymphocyte subsets and natural-killer cell activity. Anesthesiology 2000; 92: 109-15. 3. Lee NS, Yoon HR, Park JW, Yum JH, Seo JH, Cho JH, et al: The efficacy of stellate ganglion block in olfactory disorder following upper respiratory tract infection. Korean J Otolaryngol 2003; 46: 568-71. 4. Amonoo-Kuofi HS: Horner's syndrome revisited: with an update of the central pathway. Clin Anat 1999; 12: 345-61. 5. Walton KA, Buono LM: Horner syndrome. Curr Opin Ophthalmol 2003; 14: 357-63. 6. Ahmad SM, Della Rocca RC: Blepharoptosis: evaluation, techniques, and complications. Facial Plast Surg 2007; 23: 203-15. 7. Burde RM, Thompson HS: Hydroxyamphetamine. A good drug lost? Am J Ophthalmol 1991; 111: 100-2. 8. Iannuzzi M, Viola G, Cerulli A, Chiefari M, Iannuzzi E: Deformation of the 27-gauge, 3.5 inch Whitacre spinal needle: macroscopic and microscopic findings. Minerva Anestesiologica 2007; 73: 525-7. 9. Hadzic A, Dilberovic F, Shah S, Kulenovic A, Kapur E, Zaciragic A, et al: Combination of intraneural injection and high injection pressure leads to fascicular injury and neurologic deficits in dogs. Reg Anesth Pain Med 2004; 29: 417-23. 10. Ekatodramis G, Macaire P, Borgeat A: Prolonged Horner syndrome due to neck hematoma after continuous interscalene block. Anesthesiology 2001; 95: 801-3. 11. Kapral S, Krafft P, Gosch M, Fleischmann D, Weinstabl C: Ultrasound imaging for stellate ganglion block: direct visualization of puncture site and local anesthetic spread. A pilot study. Regional Anesthesia 1995; 20: 323-8. 12. Gold MS, Reichling DB, Hampl KF, Drasner K, Levine JD: Lidocaine toxicity in primary afferent neurons from the rat. J Pharmacol Exp Ther 1998; 285: 413-21. 13. Hodgson PS, Neal JM, Pollock JE, Liu SS: The neurotoxicity of drugs given intrathecally (spinal). Anesth Analg 1999; 88: 797-809. 14. Kanai Y, Katsuki H, Takasaki M: Lidocaine disrupts axonal membrane of rat sciatic nerve in vitro. Anesth Analg 2000; 91: 944-8. 15. Myers RR, Kalichman MW, Reisner LS, Powell HC: Neurotoxicity of local anesthetics: altered perineurial permeability, edema, and nerve fiber injury. Anesthesiology 1986; 64: 29-35. 16. Lake AP, Puvanachandra K: A complication of stellate ganglion block? Pain Pract 2004; 4: 130-1. 17. Hered RW, Cummings RJ, Helffrich R: Persistent Horner's syndrome after spinal fusion and epidural analgesia. A case report. Spine 1998; 23: 387-90. 18. Sukhani R, Barclay J, Aasen M: Prolonged Horner's syndrome after interscalene block: a management dilemma. Anesth Analg 1994; 79: 601-3. 19. McLachlan EM: The formation of synapses in mammalian sympathetic ganglia reinnervated with preganglionic or somatic nerves. J Physiol 1974; 237: 217-42. 20. Purves D: Competitive and non-competitive re-innervation of mammalian sympathetic neurones by native and foreign fibres. J Physiol 1976; 261: 453-75.