Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
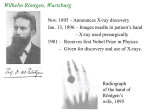
University of Wisconsin Diagnostic Imaging Research Lecture 1: Introduction (1/2) – History, basic principles, modalities Class consists of: 1) Deterministic Studies - distortion - impulse response - transfer functions All modalities are non-linear and space variant to some degree. Approximations are made to yield a linear, space-invariant system. 2) Stochastic Studies SNR (signal to noise ratio) of the resultant image - mean and variance Wilhelm Röntgen, Wurtzburg Nov. 1895 – Announces X-ray discovery Jan. 13, 1896 – Images needle in patient’s hand – X-ray used presurgically 1901 – Receives first Nobel Prize in Physics – Given for discovery and use of X-rays. Radiograph of the hand of Röntgen’s wife, 1895. Röntgen’s Setup Röntgen detected: • No reflection • No refraction • Unresponsive to mirrors or lenses His conclusions: • X-rays are not an EM wave • Dominated by corpuscular behavior Projection X-Ray attenuation coefficient Id Ioe μ ( x, y, z ) f (electron density, z) μ( x,y,z )dl Measures line integrals of attenuation Film shows intensity as a negative ( dark areas, high x-ray detection) Disadvantage: Depth information lost Advantage: Cheap, simple Sagittal Coronal Early Developments • Intensifying agents, contrast agents all developed within several years. • Creativity of physicians resulted in significant improvements to imaging. - found ways to selectively opacify regions of interest - agents administered orally, intraveneously, or via catheter Later Developments More recently, physicists and engineers have initiated new developments in technology, rather than physicians. 1940’s, 1950’s Background laid for ultrasound and nuclear medicine 1960’s Revolution in imaging – ultrasound and nuclear medicine 1970’s CT (Computerized Tomography) - true 3D imaging (instead of three dimensions crammed into two) 1980’s MRI (Magnetic Resonance Imaging) PET ( Positron Emission Tomography) Computerized Tomography (CT) Result: ID ( x, y) μ( x, y) 1972 Hounsfield announces findings at British Institute of Radiology 1979 Hounsfield, Cormack receive Nobel Prize in Medicine (CT images computed to actually display attenuation coefficient m(x,y)) Important Precursors: 1917 Radon: Characterized an image by its projections 1961 Oldendorf: Rotated patient instead of gantry First Generation CT Scanner Acquire a projection (X-ray) Translate x-ray pencil beam and detector across body and record output Rotate to next angle Repeat translation Assemble all the projections. Reconstruction from Back Projection 1.Filter each projection to account for sampling data on polar grid 2. Smear back along the “line integrals” that were calculated by the detector. Modern CT Scanner From Webb, Physics of Medical Imaging Computerized Tomography (CT), continued Early CT Image Current technology Inhalation Exhalation Nuclear Medicine Grew out of the nuclear reactor research of World War II Discovery of medically useful radioactive isotopes 1948 Ansell and Rotblat: Point by point imaging of thyroid 1952 Anger: First electronic gamma camera a) Radioactive tracer is selectively taken up by organ of interest b) Source is thus inside body! c) This imaging system measures function (physiology) rather than anatomy. Example in medical imaging: Consider a nuclear study of a liver with a tumor point source at x1= , y1= Radiation is detected at the detector plane. To obtain a general result, we need to know all combinations h(x2, y2; , ) By “general result”, we mean that we could calculate the image I(x2, y2) for any source input S(x1, y1) Nuclear Medicine, continued Very specific in imaging physiological function - metabolism - thyroid function - lung ventilation: inhale agent Advantage: Direct display of disease process. Disadvantage: Poor image quality (~ 1 cm resolution) Why is resolution so poor? Very small concentrations of agent used for safety. - source within body Quantum limited: CT 109 photons/pixel Nuclear ~100 photons/pixel Tomographic systems: SPECT: single photon emission computerized tomography PET: positron emission tomography Combined CT / PET Imaging Necessary Probe Properties Probe can be internal or external. Requirements: a) Wavelength must be short enough for adequate resolution. bone fractures, small vessels < 1 mm large lesions < 1 cm b) Body should be semi-transparent to the probe. transmission > 10-1 - results in contrast problems transmission < 10 -3 - results in SNR problems λ > 10 cm - results in poor resolution λ < .01Å - negligible attenuation Standard X-rays: .01 Å < λ < .5 Å corresponding to ~ 25 kev to 1.2 Mev per photon Necessary Probe Properties: Transmission vs. λ Graph: Medical Imaging Systems Macovski, 1983 Probe properties of different modalities NMR • Nuclear magnetic moment ( spin) • Makes each spatial area produce its own signal • Process and decode Ultrasound • Not EM energy • Diffraction limits resolution • resolution proportional to λ Introduction (2/2) – Comparison of Modalities Review: Modalities: X-ray: Measures line integrals of attenuation coefficient CT: Builds images tomographically; i.e. using a set of projections Nuclear: Radioactive isotope attached to metabolic marker . Strength is functional imaging, as opposed to anatomical Ultrasound: Measures reflectivity in the body. Ultrasound Ultrasound uses the transmission and reflection of acoustic energy. prenatal ultrasound image clinical ultrasound system Ultrasound • A pulse is propagated and its reflection is received, both by the transducer. • Key assumption: - Sound waves have a nearly constant velocity of ~1500 m/s in H2O. - Sound wave velocity in H2O is similar to that in soft tissue. • Thus, echo time maps to depth. Ultrasound: Resolution and Transmission Frequency Tradeoff between resolution and attenuation - ↑higher frequency ↓shorter wavelength ↑ higher attenuation dB Power loss: 1 cm MHz Typical Ultrasound Frequencies: Deep Body 1.5 to 3.0 MHz Superficial Structures 5.0 to 10.0 MHz e.g. 15 cm depth, 2 MHz, 60 dB round trip Why not use a very strong pulse? • Ultrasound at high energy can be used to ablate (kill) tissue. • Cavitation (bubble formation) • Temperature increase is limited to 1º C for safety. Magnetic Resonance Imaging Main Magnetic Field B0 Magnetic Resonance Imaging There are 3 magnetic fields of interest in MRI. The first is the static field Bo. 1) polarizes the sample: M( x,y,z) ( x,y,z) 2) creates the resonant frequency: γ is constant for each nucleus: γ 2π density of 1H ω = γB 42.57 MHz/Tesla for 1H Proton Spin Creates Signal Source B0 B0 w = gB 64 MHz for H+ at 1.5T Second Magnetic Field : RF Field B1 An RF coil around the patient transmits a pulse of power at the resonant frequency ω to create a B field orthogonal to Bo. This second magnetic field is termed the B1 field. B1 field “excites” nuclei. Excited nuclei precess at ω(x,y,z) = γB (x,y,z) Transmit Coils RF Coil Demodulate A/D Preamp Spin Encoding Magnetic Resonance The spatial location is encoded by using gradient field coils around the patient. (3rd magnetic field) Running current through these coils changes the magnitude of the magnetic field in space and thus the resonant frequency of protons throughout the body. Spatial positions is thus encoded as a frequency. The excited photons return to equilibrium ( relax) at different rates. By altering the timing of our measurements, we can create contrast. Multiparametric excitation – T1, T2 Brain Glioma Non-contrast-enhanced MRI Sagittal Carotid Coronal Contrast-enhanced Abdominal Imaging Time-resolved Abdominal Imaging Contrast-enhanced MR Cardiac Imaging Fat Coronal Knee Image Water Coronal Knee Image Comparison of modalities Why do we need multiple modalities? Each modality measures the interaction between energy and biological tissue. - Provides a measurement of physical properties of tissue. - Tissues similar in two physical properties may differ in a third. Note: - Each modality must relate the physical property it measures to normal or abnormal tissue function if possible. - However, anatomical information and knowledge of a large patient base may be enough. - i.e. A shadow on lung or chest X-rays is likely not good. Other considerations for multiple modalities include: - cost - safety - portability/availability Comparison of modalities: X-Ray Measures attenuation coefficient μ ( x, y, z ) Safety: Uses ionizing radiation - risk is small, however, concern still present. - 2-3 individual lesions per 106 - population risk > individual risk i.e. If exam indicated, it is in your interest to get exam Use: Principal imaging modality Used throughout body Distortion: X-Ray transmission is not distorted. Comparison of modalities: Ultrasound Measures acoustic reflectivity R( x, y, z ) Safety: Appears completely safe Use: Used where there is a complete soft tissue and/or fluid path Severe distortions at air or bone interface Distortion: Reflection: Variations in c (speed) affect depth estimate Diffraction: λ ≈ desired resolution (~.5 mm) Comparison of modalities: Magnetic Resonance (MR) Multiparametric M(x,y,z) proportional to ρ(x,y,z) and T1, T2. (the relaxation time constants) Velocity sensitive Safety: Appears safe Static field - No problems dB 10 T/s - Some induced phosphenes dt Higher levels - Nerve stimulation RF heating: body temperature rise < 1˚C - guideline Use: Distortion: Some RF penetration effects - intensity distortion Clinical Applications - Table Chest + widely used + CT - excellent Abdomen – needs contrast + CT - excellent Ultrasound – no, except for + heart + excellent – problems with gas Merge w/ CT X-Ray/ CT Nuclear + extensive use in heart MR + growing cardiac applications + minor role Head + X-ray - is good for bone – CT - bleeding, trauma – poor + PET + standard Clinical Applications – Table continued… Cardiovascular X-Ray/ + X-ray – Excellent, with CT catheter-injected contrast Ultrasound + real-time + non-invasive + cheap – but, poorer images Nuclear + functional information on perfusion Skeletal / Muscular + strong for skeletal system MR + excellent + getting better High resolution Myocardium viability – not used + functional - bone marrow Economics of modalities: Ultrasound: ~ $100K – $250K CT: $400K – $1.5 million (helical scanner) MR: $350K (knee) - 4.0 million (siting) Service: Annual costs Hospital must keep uptime Staff: Scans performed by technologists Hospital Income: Competitive issues Significant investment and return